




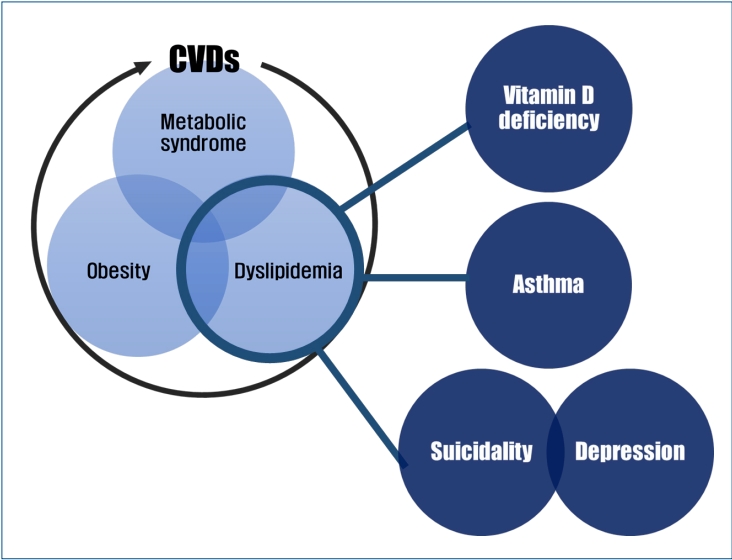
Graphical abstract.
Introduction
Cholesterol is a major structural constituent of the cell membrane and an essential molecule for the synthesis of steroid hormones, bile acids, and fat-soluble vitamins in the body. Plasma cholesterol, absorbed from dietary sources with triglycerides (TG) or synthesized in the liver, is transported by lipoproteins such as chylomicrons, very-low-density lipoprotein, low-density lipoprotein (LDL), and high-density lipoprotein (HDL). Dyslipidemia is defined as abnormal plasma levels of cholesterol, TG, or lipoproteins.
In adults, dyslipidemia is an established risk factor for cardiovascular diseases (CVDs) along with diabetes, hypertension, and obesity [1]. Increasing evidence shows that pediatric dyslipidemia is even associated with the development of atherosclerosis and premature CVDs in early childhood [2,3]. Thus, several expert committees have developed clinical guidelines for the management of childhood dyslipidemia to promote cardiovascular health in the pediatric population [3-5].
Dyslipidemia is associated with several other health problems in children. In practice, childhood dyslipidemia tends to be considered only as a complication of childhood obesity. This article reviews the current data on dyslipidemia-related pediatric health issues other than CVDs to broaden our understanding of cholesterol in childhood.
Definition of dyslipidemia in Korean children and adolescents
To define dyslipidemia in children and adolescents, the normal distribution of lipids and lipoproteins in the pediatric population must first be determined. Because lipid levels change with growth and maturation, the normal values in children differ from those in adults and vary further by age, sex, and ethnicity [6]. In the United States, the normal lipid and lipoprotein levels in childhood, adolescence, and adulthood were established based on multiple screening cohort studies [3]. In 1992, an expert panel of the National Cholesterol Education Program (NCEP) on cholesterol levels in children suggested the cutoff points to delineate total cholesterol (TC) and LDL cholesterol (LDL-C) levels and categorized them as “acceptable,” “borderline,” and “high.” [7] In 2011, the expert committee of the National Heart, Lung and Blood Institute (NHLBI) updated the NCEP pediatric guidelines and defined the TC, LDL-C, TG, and HDL-cholesterol (HDL-C) levels at which further intervention should be considered to reduce the risk of CVDs [3]. Thereafter, several academic societies including the American Academy of Pediatrics, American Heart Association, and American College of Cardiology adopted the NHLBI definition for their updated guidelines for the management of pediatric dyslipidemia [3-5]. The Korean Society of Pediatric Endocrinology recently established clinical practice guidelines in which the 2011 NHLBI guidelines were also adopted for determining the levels of screening and treatment for pediatric dyslipidemia [8]. In the population of Korean children and adolescents, dyslipidemia is defined as one of the following: serum TC level, ≥200 mg/dL; LDL-C, ≥130 mg/dL; non-HDL, ≥145 mg/dL; TG ≥130 mg/dL (in children 0–9 years of age, ≥100 mg/dL); and HDL-C, <40 mg/dL.
As shown in Table 1, the suggested cutoff points for “borderline” and “abnormal” levels represented the 75th and 95th percentiles, respectively, while the low cutoff point for “abnormal” HDL-C represented the 10th percentile. However, according to recent reports based on data from the Korean National Health and Nutrition Examination Surveys (KNHANES, 2007–2013, 2019) of Korean individuals aged 10–19 years, the percentile value of the cutoff points for “abnormal” levels differs from that suggested in the guidelines [9-11]. For example, the cutoffs of a TC level of 200 mg/dL and non-HDL-C of 145 mg/dL are equivalent to the 90th–95th percentiles, while the cutoff of HDL-C of 40 mg/dL falls to the 10th–25th percentile among Korean children (Table 1). In addition, a TG cutoff of 130 mg/dL corresponds to the 75th–90th percentile; hence, some reports have suggested a cutoff of 150 mg/dL for TG, which corresponds to the 90th percentile for Korean children, as the “abnormal” cutoff in Korean children and adolescents [12,13].
Therefore, additional large-scale nationally representative studies are needed to define the appropriate cutoff points for the Korean pediatric population. Additionally, there are no reports on the normal distribution of lipid profiles in Korean children under 10 years of age. Definitive criteria for dyslipidemia in the Korean pediatric population should first be determined to establish effective screening or treatment guidelines for dyslipidemia in Korean children and adolescents.
Prevalence of dyslipidemia in Korean children and adolescents
According to a nationwide cross-sectional survey of the KNHANES, the prevalence of hypercholesterolemia in Korean adults aged 30 years or older has almost doubled over 10 years from 10.8% and 11.8% in men and women in 2009 to 21.0% and 23.1%, respectively, in 2019 [11]. The prevalence of hypercholesterolemia varied by sex and age in Korean adults. The prevalence of hypercholesterolemia in men is relatively high before the age of 60 years and higher in women aged over 60 years [14].
Meanwhile, the prevalence or incidence of dyslipidemia in Korean children and adolescents is unknown due to the lack of nationwide statistics. Based on a study of Korean children aged 10–18 years using data from the KNHANES IV (2007–2009), 19.7% of children had at least one abnormal lipid profile [9]. The prevalence of hypercholesterolemia, a high LDL-C, a high TG, and a low HDL-C was reportedly 6.5%, 4.7%, 10.1 %, and 7.1%, respectively. Girls were more likely to have hypercholesterolemia and higher LDL-C levels than boys (7.4% vs. 5.8% for TC; 5.5% vs. 4.1% for LDL-C). However, the cutoff points applied in the study for a high TG (≥150 mg/dL) and low HDL-C (<35 mg/dL) differed from the currently adopted definition of pediatric dyslipidemia. When the cutoffs for the low HDL-C of <40 mg/dL were applied, the prevalence of low HDL-C changed from 7.1% to 11.9% [8].
To understand the sex- and age-specific trends in the prevalence of dyslipidemia in Korean children and adolescents, further large-scale studies that include nationwide statistics are required. Most importantly, the determination of the definitive criteria for dyslipidemia among the Korean pediatric population is a prerequisite for epidemiological studies.
Etiology of dyslipidemia in children and adolescents
1. Primary dyslipidemia
Primary dyslipidemia is caused by genetic defects (i.e., monogenetic and polygenic) in lipoprotein metabolism. Patients with inherited disorders of dyslipidemia often have a family history of premature CVDs with mostly autosomal dominant penetration. Monogenic conditions include familial hypercholesterolemia (FH), familial defective apolipoprotein B, familial dysbetalipoproteinemia, and familial hypertriglyceridemia. In adults, FH is the most common single-gene mutation disease associated with CVDs [15]. A polygenic condition is caused by an interaction between multiple susceptibility genes and the environment. This includes familial combined hyperlipidemia (FCHL) and polygenic hypercholesterolemia, with FCHL being the most common primary lipid disorder, occurring in 1%–2% of the population. The phenotypes of FCHL overlap those of metabolic syndrome and diabetic dyslipidemia; in children with FCHL, they most often manifest with obesity such that their dyslipidemia is often considered associated with obesity [15].
2. Secondary dyslipidemia
Secondary dyslipidemia is defined as dyslipidemia caused by diseases and certain conditions, including obesity, type 2 diabetes mellitus, nephrotic syndrome, chronic inflammatory disease, hypothyroidism, hepatic disease, and the use of certain drugs (e.g., corticosteroids, isotretinoin, β-blocking agents, chemotherapeutic agents, antiretroviral agents, and psychotropic medications such as olanzapine) [3,15]. The excessive dietary intake of saturated fats is also an important cause of dyslipidemia.
Etiological studies of pediatric dyslipidemia are rare, and most cases of pediatric dyslipidemia are considered secondary dyslipidemia. In particular, obese children with dyslipidemia show a pattern of combined dyslipidemia presenting as a mild elevation in TC and LDL-C or a moderate to severe elevation in TG and a low HDL-C [3]. However, primary dyslipidemia should be considered a differential diagnosis, even in children with obesity or diabetes when there is a family history of dyslipidemia or premature CVD.
Pediatric health issues associated with lipid profiles
1. Vitamin D metabolism associated with dyslipidemia
Vitamin D is an essential component of calcium metabolism and bone health. In addition to its classical physiological function, vitamin D is involved in immune function, anti-inflammatory activities, and endocrine function [16,17]. Several mechanisms have been suggested to explain how vitamin D can affect lipid profiles. Vitamin D reportedly stimulates calcium absorption in the intestine, and increased levels of intestinal calcium inhibit the synthesis and secretion of hepatic TG and reduce the intestinal absorption of fatty acids [18,19]. The absorbed calcium then induces the conversion of cholesterol into bile acid, thereby decreasing cholesterol levels [20]. Vitamin D can influence TG concentrations by interacting with parathyroid hormone (PTH). High serum levels of 25-hydroxy vitamin D (25[OH]D) suppress serum PTH levels, which in turn increase TG levels [21]. Vitamin D deficiency may also cause insulin resistance by impairing the function of pancreatic β-cells that could affect lipoprotein metabolism, leading to increased TG and decreased HDL-C levels [22].
It is well documented that vitamin D is associated with cardiometabolic risk factors such as obesity, high blood pressure, metabolic syndrome, and CVDs [23,24]. However, in a recent cross-sectional study of 3,788 Chinese adults, vitamin D deficiency was directly associated with dyslipidemia regardless of obesity, diabetes, and hypertension status [25]. The study indicated that serum 25(OH)D levels were inversely correlated with LDL-C and TG levels and positively correlated with HDL-C levels, even after the adjustment for several other cardiometabolic risk factors. In the pediatric population, a meta-analysis of 17 cross-sectional pediatric studies of 25,394 subjects revealed a weak significant association between vitamin D status and TC, TG, LDL-C, and HDL-C levels, indicating that higher serum levels of vitamin D are associated with a more favorable lipid profile in children and adolescents [26].
On the other hand, a few Korean studies of the pediatric population yielded inconsistent findings for each lipid profile. A cross-sectional study of 310 Korean children aged 10–12 years reported a significant association between serum vitamin D levels and metabolic risk factors such as dyslipidemia and insulin resistance [27]. However, after the adjustment for body fat, sex, and age, serum 25(OH)D levels were inversely correlated with TC and TG levels but not with HDL-C levels. Another study of 1,660 Korean children aged 9 years found that low levels of vitamin D (serum 25[OH]D <15.5 ng/mL) were associated with hypertriglyceridemia but not with low HDL-C, the components of metabolic syndrome, even after the adjustment for body mass index (BMI) [28]. Additionally, data from a nationally representative sample of 1,540 Korean adolescents revealed no significant relationship between vitamin D insufficiency (serum 25[OH]D ≤20 ng/mL) and hypertriglyceridemia or low HDL-C with or without the adjustment for confounding variables such as BMI and sex [29]. In a recent study of nonobese children aged 9–18 years, vitamin D levels were significantly inversely associated with TG levels and TG/HDL-C ratios. The vitamin D-deficient group (serum 25[OH]D <20 ng/mL) showed higher serum TG levels and TG/HDL-C ratio than the normal vitamin D level group [30]. Another recent study of nationwide representative data of 2,581 nonobese children aged 12–18 years revealed that vitamin D deficiency (serum 25[OH]D ≤20 ng/mL) was associated with low HDL-C levels but not with high TC, TG, and LDL-C levels [31].
Despite the inconsistent results for each lipid profile, most studies showed an overall positive association between serum 25(OH)D levels and favorable lipid profiles. However, it is unclear whether vitamin D supplementation positively affects lipid profiles [32,33]. Some clinical trials of Iranian adolescents showed inconsistent results regarding the effects of vitamin D on lipid profiles [34,35]. In a recent randomized single-blind placebo-controlled trial of Iranian boys, the monthly supplementation of vitamin D (50,000 IU) for 6 months decreased serum TG levels and increased HDL levels [36]. Meanwhile, a recent meta-analysis of randomized controlled trials showed that vitamin D supplementation increased LDL-C levels without affecting TC, HDL-C, and TG levels, highlighting the unfavorable effects of vitamin D supplementation on LDL-C [37].
In practice, obese patients with dyslipidemia tend to focus more on vitamin D replacement to improve their lipid profiles. However, adipose tissue may serve as the site of sequestration of the fat-soluble vitamin D, trapping it and lowering its serum levels. Therefore, instead of lifestyle modifications such as weight reduction, exercise, or diet change to reduce fat tissue, clinicians should be cautious of using vitamin D supplementation when dealing with obese children. Large well-designed population-based interventional studies are required by controlling for confounders that involve lifestyle variables such as dietary factors or physical activities to determine the relationship between vitamin D replacement and lipid profile improvement.
2. Respiratory diseases associated with dyslipidemia
Cholesterol has a complex effect on inflammation at the cellular level causing a proinflammatory cellular response [38]. The dysregulation of cholesterol and phospholipid transport in airway smooth muscle cells may be important in the pathogenesis of asthma [39]. The metabolic abnormalities of dyslipidemia or hyperinsulinemia may activate the innate and adaptive immunities that amplify the propagation of inflammation in the respiratory tract and subsequently increase bronchomotor tone, airway inflammation, and hyperreactivity [40].
Several reports have detailed the positive association between obesity and asthma in children [41,42]. Overweight or obesity are well-known significant risk factors for childhood asthma and wheezing. In the obesity–asthma link, diverse mechanisms have been suggested in which metabolic abnormalities such as dyslipidemia or insulin resistance have been considered possible contributing factors for the development of “obese asthma.” [43] In other words, obesity is closely linked with the development of dyslipidemia, insulin resistance, or diabetes, which in turn compromises respiratory function [44].
On the other hand, there is strong evidence that asthma is directly associated with dyslipidemia regardless of BMI [43,45]. In a study of 17,994 children aged 4–12 years, physician-diagnosed asthma was significantly associated with high serum TG levels after control for BMI and sex [45]. In a cross-sectional study of 85,555 Spanish adults, self-reported wheezing was associated with high serum TG and low HDL-C levels after adjustment for adiposity, suggesting TG and HDL-C as markers or inducers of inflammation-associated disease [46]. However, a meta-analysis of 20 studies including 9 pediatric reports revealed that asthma was associated with higher TC and LDL-C levels but not with TG and HDL-C levels [47]. In particular, accumulating evidence suggests an association of HDL-C with pulmonary function [48]. Another recent meta-analysis of pediatric studies showed that children with asthma had lower HDL levels, but no association with LDL-C levels was noted [49]. A recent nationwide population-based study of Korean adolescents using KNHANES V (2010–2012) data reported that the asthma prevalence was higher among adolescents with high TC levels and an elevated TG/HDL-C ratio, and the correlation was maintained even after the adjustment for confounding factors such as BMI and energy and fat intakes [50]. However, the opposite findings were observed in a study of healthy Korean male adolescents, including an association between high HDL-C level and reduced pulmonary function [51].
Despite the conflicting results for each lipid profile among previous reports, it has to be noted that several studies reported no association between respiratory function and dyslipidemia. A recent study of nationwide representative survey data of 23,841 children in the United States reported no association between the current presence of childhood asthma and serum lipid profiles after the control for confounders such as sex, race, and BMI z score [52]. In addition, a recent cohort study revealed that lipid levels at 6 years of age were not associated with respiratory function and physician-diagnosed asthma at 10 years of age [53].
To determine the relationship between respiratory inflammation and lipid profiles, further research is needed on other inflammatory respiratory tract diseases including asthma by controlling for confounders such as dietary intake, glucose metabolism, systemic infection, and body adiposity, which may affect the lipid profile and respiratory inflammation.
3. Mental and behavioral health problems associated with dyslipidemia
Increasing evidence supports the association between mental health problems and serum lipid levels over the past decades [54]. Cholesterol is essential to axonal functioning and myelin formation in the central nervous system [55]. Low cholesterol level–induced alteration of microviscosity in the lipid bilayer of the cell membrane causing serotonin transmission dysfunction or serotoninergic receptor alteration has been partly implicated in the pathophysiology of psychiatric illnesses such as suicidality and mood alteration [56-58].
Several observational studies have reported on the association between lipid profiles and depression, depressive mood, and suicidality, including suicide attempts, ideation, and completion, but their results are inconsistent. A meta-analysis of 65 epidemiological studies reported an inverse association between suicidality and serum lipid levels, indicating that patients with suicidal ideation had significantly lower serum lipid levels [59]. Another meta-analysis of 36 articles published through 2015 demonstrated a significant association between depression and low serum LDL levels [60]. In contrast, a recent meta-analysis concluded that the first episode of major depressive disorder in adults was significantly associated with elevated TG levels and decreased HDL levels but was not associated with TC and LDL-C levels [61].
According to Korean data, the association between lipid profiles and mental health problems may differ by age and sex. A recent nationwide representative study using KNHANES VI-2 (2014) data reported significantly higher HDL-C levels in men with depression and higher TG levels in women with suicidal ideation after the adjustment for covariates such as age, medical illness, daily intake, and vitamin D level [62]. Another nationally representative study of KNHANES V (2010–2012) data revealed that suicidal ideation was associated with lower TG levels in Korean men aged over 65 years [63].
Only a few studies have investigated the association between serum lipid levels and mental or behavioral health problems in children and adolescents [64,65]. Furthermore, most studies in Western countries focused on inpatient samples reported inconsistent results. In the case of the Korean pediatric population, a recent nationwide population-based study of KNHANES (2013–2016) data found that boys with depressive mood have higher LDL levels as categorical measurements after the adjustment for age, daily intake, and household income [66]. In a prospective cohort study of healthy Korean adolescents with an average follow-up of 6 years, consistently low or increased TC levels during adolescence increased the risk of depressive symptoms in men during early adulthood [67]. These findings indicate the different strategies to prevent depression by managing the lipid profile during adolescence. Interestingly, a recent community-based study of Korean children aged 10–12 years found that dyslipidemia with low HDL-C levels was associated with excessive daytime sleepiness regardless of age, sex, and BMI z score [68].
The discrepancies in the results of previous studies in relation to specific lipid profiles are due to the characteristics of psychiatric diseases being affected by environmental factors, while their prevalence is dependent on age and sex. Since lipid profiles are affected by age and sex as well as dietary intake, further studies investigating the relationship between cholesterol factors and mental and behavioral health issues should be designed to control for confounders such as socioeconomic status, age, and sex.
Conclusions
This article reviewed dyslipidemia-related pediatric health issues. The reviewed pediatric studies are summarized in Tables 2–4. Pediatric dyslipidemia might be associated with low serum vitamin D levels, asthma, and mental health problems such as depression and suicidality despite conflicting results for specific lipid profiles. This review provides important evidence that can increase our understanding of the impact of childhood lipid profiles. However, the studies reviewed were primarily based on association studies that do not prove cause and effect. Therefore, further large-scale population-based interventional studies are needed to establish effective screening and treatment guidelines for dyslipidemia and preventive strategies for related health problems among Korean children and adolescents.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


