


Introduction
Painful legs and moving toes (PLMT) is a rare syndrome characterized by spontaneous movements of a single or all digits and pain in one or both lower extremities1,2,3). The largest case series identified 76 patients during an 18-year period2), and only one pediatric case has been reported4).
We report the first adolescent case of PLMT in Korea and review current literature on the PLMT syndrome.
Case report
A 16-year-old girl complained of tingling pain in her left leg and continuous involuntary movements of her ipsilateral great toe one month after a second untethering surgery. Extension and flexion of her great toe, which occurred when awake and in the early stages of sleep, could not be suppressed voluntarily. Walking, sitting, or straining did not exacerbate the pain.
At birth, she had a sacral dimple at the S2–3 vertebral level. Four years previously, she had a voiding difficulty and underwent untethering surgery to correct the lipomeningomyelocele at the S2 level of the conus medullaris. A nerve conduction velocity study (NCVS) showed polyradiculopathy at the left L5 level and below with axonal involvement. A needle electromyogram (EMG) showed abnormal spontaneous activities of the left gastrocnemius medial head, abductor hallucis, and tibialis anterior/posterior. She did not complain of any symptoms of movement. She also underwent plantar fasciotomy because of equinovarus deformity of both feet. Five months later, the voiding difficulty recurred, and a second untethering surgery was performed.
Postoperatively, she developed a fever and meningeal irritation signs. Cerebrospinal fluid (CSF) analysis revealed a red blood cell count of 60,000/mm3, a white blood cell count of 150/mm3 (polymorphonucleocytes 69%, lymphocytes 18%), a protein level of 274 mg/dL, and a glucose level of 39 mg/dL. No specific organisms were cultured from the blood, urine, or CSF. Her fever and meningeal irritation signs subsided after teicoplanin was administered intravenously. Since the complete blood count showed neutropenia (absolute neutrophil count=600/mm3), teicoplanin was discontinued.
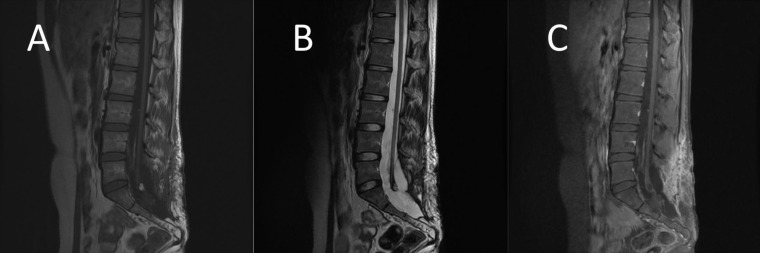
One month postoperatively, the patient presented with left leg pain and involuntary movements of her left great toe. Increased deep tendon reflex of both knees was observed with no other pathologic signs. The Babinski sign was also negative. Brain computed tomography and electroencephalography (EEG) showed no pathologic findings. Magnetic resonance imaging of the lumbar spine showed reactive inflammatory changes in the operative scar and a decreased extent and degree of reactive meningeal enhancement compared to the previous study (Fig. 1). NCVS showed no significant interval change compared to the previous study. Needle EMG showed abnormal spontaneous activities of the left gastrocnemius medial head, abductor hallucis, and tibialis anterior/posterior with no significant interval change since the previous study.
We prescribed gabapentin (100 mg three times a day); left leg pain and involuntary movements diminished within a day. Complete relief from involuntary toe movements was achieved within four months of gabapentin treatment in the outpatient department.
Discussion
Some variants of PLMT syndrome include painless legs and moving toes, painful arms and moving fingers, painless arms and moving fingers, and painful mouth and moving tongue2,3,5). In the largest case series, the mean age of onset was 58 years (range, 24–88 years)2). One pediatric case (an 11-year-old girl) was reported in 20134). In the Republic of Korea, there have only been a few adult cases of the PLMT syndrome5,6,7).
Most patients' primary complaint is pain, which is more distressing than involuntary movement2,3). Although patients' descriptions of their pain are diverse (e.g., tingling, numbness, aching, burning, etc.), all of them report that it is constant. Some patients' pain was exacerbated by certain situations, including physical positions (e.g., sitting, walking, bearing weight, or bending), diurnal variation (night or day), cold temperature, external pressure, and the Valsalva maneuver. Conversely, in other patients, the same situations have alleviated the pain2).
Voluntary and temporal suppression of symptoms by applying pressure to the sole of the foot has been reported3). In our patient, none of the aforementioned situations diminished or intensified the symptoms of involuntary movement. The involuntary movements tended to be constant, sometimes fluctuating in severity, and stereotypical to a particular individual2). Reportedly, involuntary movements include flexion/extension, abduction/adduction, wriggling/dystonia/writhing, or irregular, random, rhythmic twitching, fanning, clawing, waving, etc.3).
Underlying disorders of the PLMT syndrome have been reported at the level of the peripheral or central nervous system (e.g., peripheral neuropathy, radiculopathy, spinal cord lesions, trauma, myelitis, compressive myelopathy, Wilson disease, Parkinson disease, and Hashimoto disease)1,2,3). However, the reason why PLMT syndrome is so rare is not well understood. Recently, peripheral neuropathy was considered to be the most commonly identifiable cause of pain in 21 of 76 patients (28%); conversely, 32 (42%) had no identifiable cause of pain2). Thus, the exact mechanism is still unknown.
Clinically, the PLMT syndrome's potential origin is within the peripheral nervous system; however, the disorder's evolution suggests that the central nervous system is involved in the persistence of pain, which mediates movement of the digits. These observations support neuromodulation, with central hardwiring underlying the PLMT syndrome. This makes the condition very difficult to treat; presumably, neuromodulation drives the movement of the digits via a generator at the spinal cord or brainstem2).
There is no single electrophysiologic signature of the PLMT syndrome. Recently, the findings of an NCVS were normal in 33 of 63 cases, and the remainder showed mild abnormalities, including chronic radiculopathy (14 cases), peripheral neuropathy (9 cases), cramps and fasciculations (4 cases), isolated fasciculations/fibrillations (5 cases), mononeuropathy (3 cases), and evidence of prior poliomyelitis (1 case). An EMG showed irregular (not truly rhythmic) phasic bursts with various durations (range, 10 msec to 2 seconds), which were associated with cocontraction and digit or distal limb movements2). The bursts had broad frequencies (range, 1.5–200 Hz)2,3). In the pediatric case, NCVS and EMG were unremarkable4).
PLMT can be distinguished from other movement disorders by its characteristic clinical features. Restless leg syndrome also has both discomfort and movements of lower limbs, but the pain of PLMT is not relieved by movements. PLMT does not involve skin change or altered temperature unlike complex regional pain syndrome2). Epilepsia partialis continua is usually painless and accompanied by structural brain lesions and epileptic discharges on an EEG3). Other movement disorders that need to be differentiated from PLMT are chorea, pseudoathetosis, spinal segmental myoclonus, psychogenic movement disorder2,3).
In a recent large case series, only one-third of patients responded to pharmacologic treatment for involuntary movements or pain2). In the pediatric case and our adolescent case, the response to gabapentin was good4). The difference may originate from the onset age or the duration between onset and treatment. However, we need more pediatric and adolescent cases to verify that. There were also some case reports that gabapentin was effective for pain and movements symptoms in adult PLMT patients and the therapeutic effect started in 1-4 days6,8). There was no consensus for the duration of gabapentin therapy. In our case, we ceased gabapentin after 4 months. Since then, there has been no recurrence.
The PLMT syndrome is rare but it should be considered during differential diagnosis of children and adolescents with pain in the limbs and involuntary movements in the toes.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


