

Introduction
Sialolithiasis refers to a type of salivary disease involving the formation of calcareous concretions, or sialoliths, within a salivary gland or its excretory duct so as to obstruct the salivary flow. This consequently yields salivary ectasia and further dilates the gland, which can be followed by ascending infection1).
Sialolithiasis is a relatively common salivary gland disease, present in an estimated 12 in 1,000 of the adult population2), with dominant prevalence in males and peak incidence between the age of 30 and 60 years. However, the overall incidence in pediatric populations is extremely rare, accounting for only 3% of all sialolithiasis. Parotid sialolithiasis is even less frequent (10% to 20%) compared to submandibular sialolithiasis (80% to 90%) and usually affects the salivary duct unilaterally rather than the salivary gland1). Parotid stones are smaller in size and more radiolucent than submandibular stones, therefore conventional X-ray is usually insufficient to detect them3).
Varied diagnosis and treatment options have recently emerged. In our case, a 2-year-old boy was diagnosed with parotid silaolithiasis using a computerized tomographic (CT) scan of the neck and treated with intraoral sialolithotomy proceeded by an empiric antibiotic regimen. We disclose one of the youngest cases of parotid sialolithiasis worldwide and discuss the disease by reviewing some of the related studies.
Case report
A 2-year-old male patient was referred from a local clinic complaining of painful swelling in the right parotid area and low grade fever. He had no past medical history except for the treatment of his right parotitis at the local clinic 2 weeks before. At that time, he had suffered from painful swelling in the same right parotid area for 5 days, which was relieved the next day after the oral antibiotic was switched.
On admission, extraoral examination revealed a broad area of swelling in the right parotid area with indurated overlying skin that was warm and tender to the touch. Intraorally, a solid mobile formation was revealed near the right parotid duct opening on palpation, possibly the calculus, as well as pus discharge at the duct opening on pressing.
A CT scan of the neck was performed, which showed an asymmetric enlargement and heterogenous enhancement in the right parotid gland (Fig. 1) and two oval sialoliths located near the orifice of the right Stensen's duct (Fig. 2), suggesting acute suppurative parotitis with duct sialolithiasis.
On laboratory test, leukocytosis (white blood cells, 17,200/┬ĄL) and elevated C-reactive protein (1.54 mg/dL) were observed. The amylase (42 U/L) level was within the normal range and the IgG/IgM antibodies of mumps virus were negative. The total serum calcium (10.3 mg/dL) level was within the normal range and the Mantoux test was negative.
Abdominal sonography showed no calculus in the regions of the gall bladder, kidneys, pancreas and other parts of the abdomen.
Medical treatment was initiated immediately with analgesic-anti-inflammatory drugs and intravenous antibiotics. The pus was drained daily by means of dilating and milking the duct orifice with a lacrimal probe.
On the third day of hospitalization, the swelling and fever began to subside. As the calculi were located near the duct orifice, and the patient continued to complain of colicky pain, we planned their surgical removal by an intraoral approach. A simple sialolithotomy was performed with no invasive incision, because the calculi were just beneath the duct orifice that had become enlarged due to the drainage of pus. Appropriate pressure on the duct orifice was on its own satisfactory to retrieve the calculi and purulent discharge.
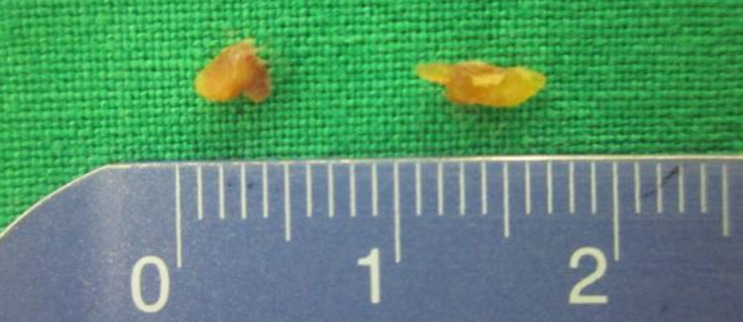
The calculi had irregular borders and a yellowish color. The fusiform-shaped one measured about 6 mm├Ś2 mm in size and the rather ovoid-shaped one measured around 3 mm├Ś3 mm (Fig. 3). Culture of the drained pus grew ╬▒-hemolytic streptococci, while the blood culture was sterile.
The patient was kept on parenteral antibiotics for 4 days and switched to an oral alternative when discharged from the hospital. On one week follow-up, the swelling was almost normalized without any further problems and the patient was prescribed 3 additional days of oral antibiotics.
Discussion
Sialolithiasis is a relatively common disease of salivary glands, reported to account for up to 30% of this disease category, but is rarely observed in childhood and adolescence1). Zenk et al.4) found that only 6.1% of 635 patients with sialolithiasis were younger than 20 years and among these there were two cases of a solitary parotid gland stone in a 4-year-old girl and a 2-year-old boy. The patient described in our own case was 2 years old, and is therefore one of the youngest known cases of parotid sialolithiasis. Furthermore, this is one of the rare reports in which intraoral removal of a stone as large as 6 mm was successful without incision. The clinical data of young children, particularly those with parotid sialolithiasis, were summarized in Table 15-8).
Several theories have been suggested as to the pathogenesis of sialolithiasis but none have yet been firmly established. The sialolith is assumed to be formed by the deposition of organic and inorganic materials around a central core. The central core is composed of the precipitation of calcium salts around an initial organic nidus that consists of altered salivary mucins, bacteria and desquamated epithelial cells. The organic layers are composed of various carbohydrates and amino acids and the inorganic layers consist of calcium phosphate, a small quantity of carbonates in the form of hydroxyapatite, and a small amount of magnesium and ammonia9). The ratio of organic to inorganic material in a submandibular stone is 18:82, whereas that in a parotid stone is 51:493). Grossly, the sialolith has a round or ovoid shape, a porous texture and a pale yellow color, measuring from 1 mm to less than 1 cm in general. Examples larger than 15 mm are considered giant calculi, of which only a handful of cases have been reported10).
A combination of various factors is speculated to be involved in the formation of calculi. Chronic infection of the parotid gland and secondary trauma to its duct underlies the origin of calculus, whereas the anatomical and chemical properties of the submandibular gland predispose it to calculus formation, which further induces stagnation of saliva and invasion of bacteria3).
One study proposed the role of foods, bacteria or foreign bodies within the oral cavity in stone formation. These may ascend the duct system and become the nidus for calcification combined with attracted inflammatory cells in the formation of parotid stones, whereas, mucus is thought to be the nidus in the case of submandibular stones11). Another study proposed that certain unknown metabolic abnormalities can increase the alkalinity of saliva, consequently promoting the crystallization of calcium and phosphates9). Stagnation of saliva, or physical trauma to the salivary gland or its duct may also play a role in calculus formation2). Systemic diseases have not been proved to be associated with sialolithiasis except for gout, although its calculi consist mainly of uric acid9). Nephrolithiasis was reported to be linked with sialolithiasis in up to 10% of patients in one study1). Presumably, the etiologic factor of calculi in our case appears to be bacterial infection, which triggered an increase in salivary PH and an increase of organic matter as well as tissue injury and supersaturation of saliva. But the exact cause remains undetermined, since the patient's laboratory test results were unremarkable as well as his personal history except for the previous infection of parotid gland just 2 weeks before, and it seems not possible for the stone of 6 mm in size to be formed in such a short time.
The predominance of submandibular stones can be explained by the following aspects. Anatomically, Wharton's duct is longer and wider than Stensen's duct, salivary flow is slow and against gravity, and chemically saliva is more alkaline and rich in calcium, phosphate and mucin proteins2).
Careful attention should be paid to patient history and examination in order to avoid misdiagnosis. The differential diagnosis of parotid swelling or the radiopacities on radiographic examinations, could include viral sialadenitis (mumps), acute bacterial sialadenitis, lymphadenitis, dental abscess, human immunodeficiency virus sialopathy, Sj├Čgren's syndrome, calcified lymph nodes, mainly after tuberculosis infection, phlebolithiasis, myositis ossificans and, finally, salivary gland tumors or metastasis12). Sialolithiasis usually manifests with typical symptoms of swelling of the involved salivary gland, either at meal times or without any distinct reason, and accompanying occasional pain due to the obstructed flow of saliva. Sialadenitis can develop by the stasis of saliva and subsequent bacterial ascending into the parenchyma of the gland with signs of systemic infection11). Giant calculi can be organized in the setting of incomplete obstruction with salivary leakage and remain asymptomatic for a longer period of time. Prolonged obstruction may result in atrophy of the gland, secretory dysfunction and permanent fibrosis9).
Bimanual intraoral palpation is useful in detecting stones. In the direction of posterior to anterior, submandibular stones are palpable in the floor of the mouth, and parotid stones can be revealed around the orifice of Stensen's duct or along its course. Minor salivary stones are usually found in the buccal mucosa or upper lip9). The parotid stones in our case could be easily identified by virtue of their location adjacent to the orifice.
Conventional and advanced imaging techniques have been developed in diagnosing sialolithiasis. Conventional intraoral X-ray may be useful but has limited application, since 40% of parotid and 20% of submandibular stones are radiolucent3). For parotid stones, the masseter muscle and the buccinator are additional obstacles to visualizing the calculi in Stensen's duct. In such cases, sialography is an adequate replacement modality which makes it possible to visualize the whole duct system. However, sialography is not viable in the setting of acute infection or in patients allergic to contrast medium. Nor it is indicated when the stone is located in the distal part of the duct, as the injected contrast medium could push the stone proximally, hence making its removal difficult9).
CT scan and magnetic resonance imaging (MRI), although more complex and expensive than sialography, are currently emerging as the diagnostic tools of choice due to their advantages of accuracy and lower invasiveness. CT scan enables the detection of recently calcified salivary stones, which conventional radiography cannot achieve, although thick radiological slices could occult the stones. However, CT scan is neither capable of localizing the stone precisely within the duct, nor of visualizing the ducts and their anomalies13). On the other hand, MRI allows consistent and accurate visualization of salivary stones and the duct system. However, MRI has several disadvantages including distortion artifacts due to dental amalgam, equipment costs and a longer reconstruction duration14). Sialendoscopy is a new procedure that can be used either as a diagnostic means by visualizing intraductal stenosis, obstruction and inflammatory changes, or as a treatment option for pathologic conditions15).
Therapeutic strategy depends on the size and location of the calculi. Conservative treatment, rather than surgical removal, is accepted as the first choice in managing small calculi located in the distal section of the duct, expecting their spontaneous expulsion9). Hydration should be administered to patients with infrared heating and massage of the gland. Natural sialogogues such as a slice of lemon or medications such as pilocarpine are beneficial as they stimulate the production of saliva and subsequent flushing of calculi. Antibiotics should be initiated whenever infection is suspected to be combined11). Administration of penicillinase-resistant antistaphylococcal agents for 7-10 days, is generally accepted. However, many cases fail to respond to such a regimen. The success rate of spontaneous passage of stones with conservative management for a period of 3 months is only 10%16).
Therefore, a surgical approach should be considered if the stone is medium or large in size and the failure of medical treatments is anticipated, leaving only salivary colic. As the calculi in our case were near the duct orifice with superimposed infection, conservative management was started. However, salivary colic was persistent and the calculi were quite large not enough for spontaneous washout, thus surgical removal was employed.
Traditionally, surgical techniques are determined by the location of the calculi. Intraoral sialolithotomy can be performed if the stone is in the distal portion of the duct, especially submandibular, that is palpable within the oral cavity. The procedure may need incision or just forward milking to retrieve the calculus17). In the case of parotid stones, the possibility of intraoral approach is limited to those that lie anterior to the curvature of Stensen's duct above the masseter muscle. The facial nerve can be compromised depending on the location of the calculi. Extraoral approach is no longer performed due to the risk of surgical scars and a lower effectiveness compared to intraoral approach18). Interventional sialendoscopy is a new and less invasive procedure by which distal calculi can be removed with microforceps and basket, with or without laser fragmentation. This treatment option is preferably applied to the pediatric population, since the calculi in children are smaller and distally located compared to those in adults19). Sialadenectomy is required for those sialoliths which are in the proximal part of the duct or within the gland, and cannot be palpated intraorally.
Shock wave lithotripsy is a recently updated alternative technology which is minimally invasive and carries fewer risks than surgical procedure. Extracorporeal shock wave lithotripsy utilizes shockwaves from outside the body to split calculi into fragments that are small enough for spontaneous washout. Endoscopic intracorporeal shock wave lithotripsy was introduced more recently. Here, a flexible fiberscope is advanced into the duct and shockwaves are delivered from the endoscopic probe directly to stones17).
In conclusion, sialolithiasis is exceedingly rare in childhood and thus tends to be omitted in differential diagnosis. The patient in our own case had originally been diagnosed with parotitis and treated accordingly until intraoral palpation was attempted. The literature review highlights the importance of careful history taking and intraoral examination. This should inspire clinicians to assess sialolithiasis with a more comprehensive approach in clinical practice, especially in the pediatric population.



 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


