


Introduction
Brugada syndrome (BrS) is recognized as an important cause of sudden cardiac death (SCD) occurring in individuals at a relatively young age. BrS is an inherited cardiac arrhythmia condition, characterized by coved ST elevation and J point elevation of at least 2 mm in at least two of the right precordial electrocardiogram (ECG) leads (V1-3)1). It is a familial condition that displays an autosomal dominant mode of transmission. In the majority of patients, BrS is caused by mutations in the cardiac sodium channel gene SCN5A, which encodes the α-subunit of the sodium channel. There are fewer reports of pediatric BrS than adult because BrS usually develops as arrhythmia in adulthood.
Case report
The boy presented with a white pupil in his left eye and was diagnosed with retinoblastoma in the left eye at 16 months of age. He was placed on retinoblastoma chemotherapy protocol 2005 for 4 months and his left eyeball was enucleated. At 26 months of age, the boy suffered a high fever and was brought to our emergency department on the 4th day after fever developed. His vital signs in the Emergency Department were blood pressure 94/56 mmHg, heart rate 134 beats/min and temperature 37.5℃. The physical examination found no specific cause of the fever. As the patient still had a central line for chemotherapy, a catheter-related infection was initially suspected, so blood cultures were taken and empirical antibiotics was given.
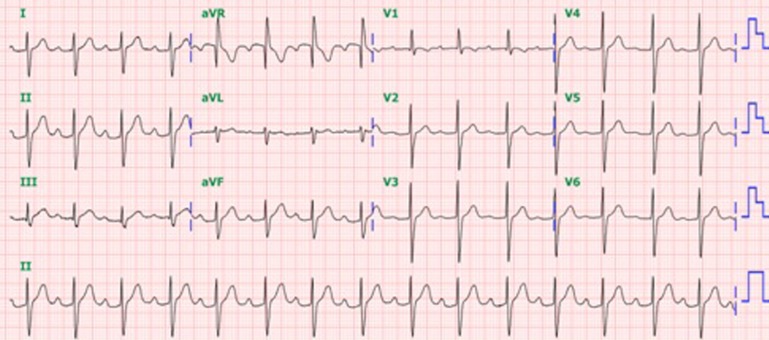
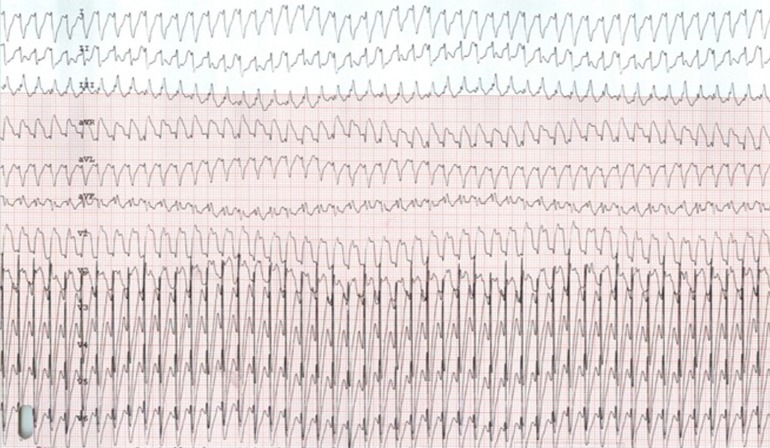
The baseline ECG showed a first-degree atrioventricular (AV) block with a PR interval of 268 ms and a QRS duration of 103 ms (Fig. 1). The echocardiographic findings were normal. On the 5th day of fever, his body temperature measured by tympanic thermometer was 41℃. The boy suddenly developed monomorphic wide QRS tachycardia, which was characterized as having right bundle branch block (RBBB) morphology with a QRS duration of 200 ms, superior axis deviation, and a tachycardia rate of 212/min (Fig. 2). The boy was alert and his blood pressure was stable at 87/45 mmHg. At first, the boy did not respond to adenosine treatment for wide QRS tachycardia; this was followed by amiodarone and lidocaine, but the wide QRS tachycardia was not corrected. After the failure of amiodarone and lidocaine, direct current (DC) cardioversion (1 J/kg) succeeded in recovering the patient's rhythm to sinus rhythm. The wide QRS tachycardia was diagnosed as ventricular tachycardia (VT) of unknown origin but related to high fever. Next day, the patient presented with fever up to 38.8℃ and VT occurred again. This second attack of VT did not respond to DC cardioversion, but responded to lidocaine. On the ECG, a transient Brugada pattern was observed shortly after DC cardioversion. Blood culture was positive for methicillin-sensitive Staphylococcus aureus, leading to a diagnosis of catheter-related infection. The boy was treated with nafcillin and cefazolin for 6 weeks. Investigation of his family history found that his grandfather was diagnosed as BrS because of frequent syncopal attacks (Fig. 3), had been taking quinidine, and had recently undergone insertion of an implantable cardioverter-defibrillator (ICD) because of his frequent syncopal attacks. The father also showed conduction delay with a PR interval of 204 ms and a QRS duration of 136 ms (Fig. 3), but had not experienced any episodes of VT. Gene analysis by direct sequencing of genomic DNA isolated from peripheral blood leukocytes revealed a mutation in the SCN5A gene in the patient, his father, and his grandfather, that was identified as a C to T base substitution at nucleotide position 3911 leading to replacement of threonine with methionine at codon 1304 (c.3911C>T, p.T1304M). The patient's elder sister and his mother had a normal ECG and no identified genetic mutation. The patient was treated with quinidine for 9 months, until the patient's parents stopped the treatment against medical advice. Fortunately, the boy had no more episodes of high fever causing VT, and we educated the parents about the need for the boy to be given antipyretics at the first sign of fever. There have been no more episodes of VT during 1 year of outpatient clinic follow-up.
Discussion
Brugada syndrome can be classified into 3 types according to ECG characteristics. A type 1 ECG pattern is characterized by a coved ST-segment elevation greater than or equal to 2 mm and is followed by a negative T wave in more than 1 right precordial lead (V1-V3). A type 2 ECG pattern is characterized by gradually descending ST-segment elevation that results in a saddleback morphology. A type 3 ECG pattern is characterized by ST-segment elevation less than or equal to 1 mm with either a coved type or a saddleback morphology. Diagnosis of BrS is based on the appearance of a type 1 ST-segment elevation (coved type) in more than one right precordial lead (V1-V3), in the presence or absence of a sodium channel blocker, and any one of the following suggests BrS: ventricular fibrillation, VT, a family history of SCD (aged <45 years), coved type ECGs in family members, electrophysiological inducibility, and syncope or nocturnal agonal respiration2). Since BrS was first identified by Brugada and Brugada1) in 1992, many cases have been reported in adults and children3,4). The prevalence of BrS in children has not been precisely determined because of its clinical spectrum that can range from asymptomatic to sudden death3). BrS symptoms in childhood are frequently associated with fever. Probst et al.3) showed that episodes of syncope were associated with fever in 5 of 11 cases (45%). Four of 5 patients had documented arrhythmia, polymorphic VT or monomorphic VT and atrial flutter. Three of 5 patients had a family history of BrS. Zaidi5) described a 10-year-old boy with a family history of SCD who had near syncope associated with a febrile illness, and De Marco et al.6) reported a 4-year-old boy who, while feverish, showed coved ST-segment elevation in the right precordial leads and incomplete RBBB.
The role of fever as a precipitating factor for ventricular arrhythmias in BrS has been described in previous reports7). It has been reported that mutations leading to BrS affect the temperature sensitivity of the rapid inactivation of the sodium channel8). One of the theories explaining the ECG alterations seen in BrS with fever is based on an imbalance between the depolarizing and repolarizing currents during the early repolarization phase of the action potential, mainly demonstrated by a large transient outward current in the epicardial cells of the right ventricle8). However, the exact mechanism of this effect has not yet been clearly shown.
The important consideration is that as fever is the state most likely to induce ventricular arrhythmia in childhood BrS, we need a careful evaluation of this situation, and antipyretics should be used liberally in these patients.
Genetic mutations are identified in only 20%-30% of patients with BrS and all identified mutations involve the SCN5A gene7). The relationship between gene mutation and fever is uncertain. Keller et al.9) investigated the heterogeneous genetic background of BrS and the relationship between clinical manifestations of fever-induced BrS and different mutations. There was no association between clinical manifestations and any specific mutation. Meregalli et al.10) reported a relationship between the type of mutation and the severity and conduction delay in loss-of-function SCN5A channelopathies: patients carrying T and Minactive mutations had significantly longer PR and QRS intervals than those with Mactive mutations.
Mutations in SCN5A, the gene encoding the α subunit of the most prevalent cardiac Na channel, are responsible for a spectrum of hereditary arrhythmias, including type 3 long QT syndrome, BrS, cardiac conduction disturbances, and sick sinus syndrome11). Our patient had a mutation, T1304M, in the D3/S4 voltage-sensing region of SCN5A. The threonine residues at position 1304 in the wild-type sodium channels are probably critical for proper sodium channel function12). A T1304M mutation was also reported in type 3 long QT syndrome: 5 of 6 patients in that study with this mutation had syncope-like symptoms12).
We analyzed the baseline ECG of our patient, which showed a first-degree AV block with a PR interval of 268 ms and a QRS duration of 103 ms. Chockalingam et al.13) reported that conduction intervals such as the PR interval and the QRS duration were greater than the upper limit of normal for age in 28 (85%) BrS patients, and Kanter et al.14) showed that prolonged cardiac conduction intervals have emerged as the most common manifestation of the disease in infants. Therefore, a cardiac depolarizing channel defect should be considered in patients with a structurally normal heart and fever-induced VT, and analysis of conduction delay and investigation of the family history should be performed.
Further, we need to focus on how to evaluate the risk and to stratify patients at risk for SCD, to select those patients in whom to insert an ICD. An 8% occurrence of cardiac events was observed in initially asymptomatic patients7); hence, it is important to assess the risk of cardiac events to decide between treatment options, including medication only or ICD implantation. A risk stratification scheme has been proposed, including the presence of symptoms (aborted sudden death, syncope, seizure, nocturnal agonal respiration), spontaneous or drug-induced coved type ECG pattern and a family history of sudden death.
Quinidine therapy has been proposed as an alternative to ICD implantation in asymptomatic patients with BrS4), and the largest reported study in children with BrS described the results of hydroquinidine medication. Four children, who were considered high risk with a spontaneous type-1 ECG, received hydroquinidine and did not have any symptoms over a 28-month follow-up3). However, the recommendation of prophylactic quinidine therapy is still controversial, especially in children, as its use in children is limited and not well documented. However, in our case, we used quinidine because the patient was considered high risk for SCD and was too young for the insertion of an ICD. For symptomatic patients who experience cardiac arrest or unexplained syncope, implantation of an ICD is currently the only proven effective therapy. However, ICD implantation in childhood has high morbidity, and patients require ICD replacement. Some reports have shown that quinidine prevents induction of ventricular fibrillation in high-risk patients with BrS15).
We believe that this is the first report of a pediatric case of BrS in a Korean child in which VT was provoked by high fever and a family history was present. Pediatricians should be cognizant of the possibility of BrS, especially in patients with conduction delay on baseline ECG who have a family history of sudden death and unexplained syncope.

 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


