




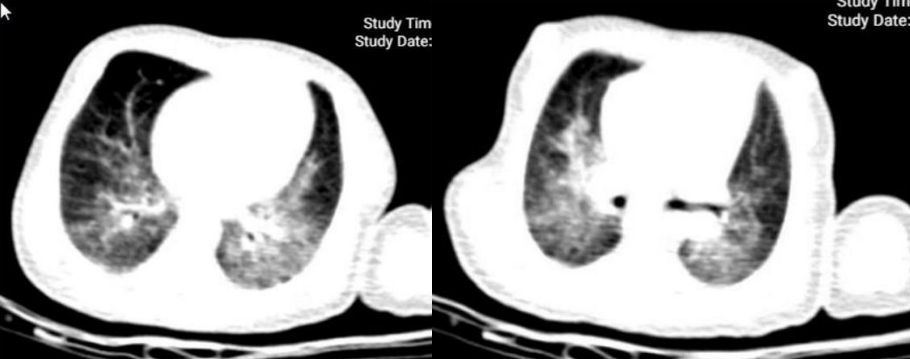
A 9-day-old male neonate with 39 weeks gestation was referred to the Emergency Department of Besat's Hospital in Hamadan City located in the west of Iran, with a history of fever and poor feeding. He was born with a delivery method of cesarean section, birth weight 3,300 g, and Apgar score of 8/9. There was no history of cough and rhinorrhea. The neonate's mother had no complications during pregnancy and delivery and they were discharged from the hospital one day after the delivery. The neonate's parents were asymptomatic, but the neonate's grandfather was infected with coronavirus disease 2019 (COVID-19). The neonate's grandfather was in contact with the neonate since birth. He was admitted to the hospital with the diagnosis of COVID-19 one day after neonate hospitalization. He was tachycardic and tachypneic. On the first day, oxygen with hood and 5 L/min volume was administered and the neonate was transferred to the neonatal care unit (Table 1). Because of the COVID-19 pandemic, a nasopharyngeal swab was sent for reverse-transcription polymerase chain reaction (RT-PCR) assay to the laboratory. RT-PCR was done 10 days after birth and the result of PCR was positive. Also, cerebrospinal fluid (CSF) analysis and urine analysis were normal. In the chest computed tomography (CT) scan bilateral, peripheral ground glass infiltration and opacity were observed (Fig. 1). Antibiotics therapy (ampicillin 25 mg/kg every 6 hours plus cefotaxim 50 mg/kg every 8 hours) was started before the result of bacterial cultures of blood, urine, and CSF. The neonate was infected with COVID-19 and gastrointestinal symptoms such as vomiting, diarrhea, and severe respiratory distress. These completed the multisystem inflammatory syndrome in children (MIS-C) criteria (Table 1). According to the protocol of Iran in the field of treatment of COVID-19, the patient with a diagnosis of MIS-C was treated with intravenous immunoglobulin (IVIG).
Multisystem inflammatory syndrome in neonates and COVID-19
The evidence suggests that most infants were not infected with COVID-19 and if they were infected had very mild symptoms [1]. However, some neonates have a severe MIS-C which can involve several vital organs. MIS-C is a condition where different body parts can become inflamed, including the heart, lungs, kidneys, brain, skin, eyes, or gastrointestinal organs. Children with MIS-C may have a fever and various symptoms, including abdominal pain, vomiting, diarrhea, neck pain, rash, bloodshot eyes, or feeling extra tired. This new syndrome can be related to COVID-19 [2,3]. MIS-C is rare, but this disease may have been observed during the COVID-19 pandemic in some studies [3,4]. In the present case, the neonate was infected with COVID-19 and gastrointestinal symptoms such as vomiting, diarrhea, and severe respiratory distress.
Difference between MIS-C and severe COVID infection in the neonate
MIS-C often occurs in age <21 years with clinical criteria: A minimum 24-hour history of subjective or objective fever ≥38.0 °C and severe illness necessitating hospitalization and 2 or more organ systems affected (i.e., cardiac, renal, respiratory, hematologic, gastrointestinal, dermatologic, neurological). Laboratory evidence of inflammation include 1 or more of the following: an elevated C-reactive protein (CRP), erythrocyte sedimentation rate, fibrinogen, procalcitonin, D-dimer, ferritin, lactate dehydrogenase, or interleukin-6; elevated neutrophils or reduced lymphocytes and low albumin [5]. The severe acute COVID-19 often occurs in children with an underlying health problem, MIS-C is found in less than 1% of children with COVID-19, mostly with no previous disease. In MIS-C, at least 2 organ systems are affected (i.e., cardiac, renal, respiratory, hematologic, gastrointestinal, dermatologic, neurological), which does not only involve the heart [6].
Treatment of MIS-C in the neonate
Some adjunct therapies have been used because of the profound inflammatory response and Kawasaki disease (KD)-like features, with IVIG. According to a Western New York guidelines [7] and our country approach, patients with KD-like illness or patients with COVID-19 diagnosis and in high-risk categories (infants, KD shock syndrome, CRP>130 g/dL, admission echo z score >2.5 or aneurysms, Asian race) should receive IVIG 1–2 g/kg as a single infusion with 3-day pulse methylprednisolone.
Result of treatment
At admission, the patient had a deceased O2 saturation (80%) that by pulse oximetry reached 85% after receiving oxygen through the hood. Respiratory distress did not improve after 2 days of treatment with antibiotics. After the PCR test result, the neonate was treated with 1 dose IVIG (1 g/kg). Two days after treatment with IVIG, oxygen saturation reached 95% and respiratory distress improved. The patient was discharged and during follow-up (2 weeks after discharge), the neonate was in good general condition.
The common symptoms in children with acute COVID-19 infection are fever and cough. Other symptoms may include sore throat, rhinorrhea, or congestion, myalgias, headache, fatigue, and gastrointestinal symptoms including nausea, vomiting, or diarrhea. Infants may also present with isolated fever, poor feeding, or fussiness [8]. A review study reported that mortality rates of MIS-C are lower compared to adult forms of severe COVID-19 disease [9].
Key message
Question: Can multisystem inflammatory syndrome in childhood (MIS-C) occur in the neonate associated with coronavirus disease 2019 (COVID-19)?
Finding: A 9-day-old neonate infected with COVID-19 had fever, respiratory distress, and gastrointestinal symptoms suggestive of MIS-C. This neonate recovered after treatment with intravenous immunoglobulin (IVIG).
Meaning: IVIG successfully treated a rare case of a 9-day-old neonate with COVID-19 and severe symptoms suggestive of MIS-C.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


