




Graphical abstract
Introduction
Ever since the World Summit for Children held in 1990, there has been a strong desire to consider the child mortality rate as an index for health and human development [1]. According to the World Health Organization (WHO) and United Nations ChildrenŌĆÖs Emergency Fund, 5.4 million of children under 5 years died in 2017 [2]. Globally, it is estimated that 60,000 children die before the age of 5 from lower respiratory infections (LRIs) caused by second-hand smoke. Health consequences of secondhand smoke exposure can continue to adulthood, so that LRIs in early childhood significantly increase risk of developing chronic obstructive pulmonary disease in adulthood [3].
Over the past decade, various goals have been defined to reduce global child mortality. For example, Sustainable Development Goals (SDGs) specify that all countries should reduce the under-five child mortality to 25 per 1,000 live births by 2030 [4]. Although the number of new cases of respiratory infections in children varies in countries and different regions of the world [5], its mortality rate is one of the highest among the causes of childhood death in the world [6]. In this regard, the spatiotemporal analysis of infectious diseases has been considered as one of the effective methods of etiology of diseases [7]. It should be noted that there is growing evidence that the dynamic spatial data are a key element in monitoring and anticipating the spread of epidemics [8].
Spatial distribution of respiratory diseases has been less studied despite its considerable geographical variation [9]. However, understanding the spatial diversity of respiratory diseases can provide a proper basis for targeted preventive interventions. To this end, the areas where the hot spots of the disease and mortality are concentrated should be specifically examined [10].
Geographic information system (GIS), which features the ability to understand geometric patterns in space and time can be used to investigate the hot spots and periodic changes of mortality [11]. GIS is a potentially useful tool for assessing various aspects of health, whose features include the ability to integrate data from different sources to generate new information and intrinsic visualization applications. It also has lasting effects on the public health by offering creative solutions for problems [12]. Although various studies have been conducted about mortality and infectious diseases, few spatial studies have been done about the mortality from respiratory infections [13]. Hence, knowing about the changes in hot spots can play a key role in health planning in the future. Therefore, this study aimed to present the spatial modeling of mortality from ALRI in children under 5 years of age in 2000ŌĆō2017: a global study.
Methods
In this descriptive study, data on mortality of children under 5 years caused by ALRI were obtained as a tabular file (Excel format) through the WHO website (http://who.int/entity/gho/publications/world_health_statistics/2017/en/index.html).
In the next step, a code from 1 to 194 was defined for each country in Excel 2007. Then the geographic information system (ArcGIS 10.6) was used for spatial modeling. For this purpose, a geo-database was created in Arc-Catalog software, then using the capabilities of GIS, a code from 1 to 194 was defined for the tables of spatial layers of countries. In the next step, the coded Excel files were joined to the coded spatial layers of each country using the Join command. Then, in ArcMap software environment, spatial tests and related maps were extracted. To spatial analysis of ALRI in children under 5 years of age, we used the spatial auto-correlation analysis (Global Moran's I, GMI), Getis-Ord Gi (GOG) statistic, and geographically weighted regression (GWR).
GMI is calculated as follows (Equation 1-1 to 1-4):
Where Xi and Xj represent the variable values in the locations i and j. In addition, X shows the average of the attributes of each location, and Wij is the spatial weight of i and j. If i and j are in the neighborhood of each other, the Wij value equals one, otherwise, the value equals zero. Moreover, S0 denotes the sum of all the elements.
To determine the spatial distribution of hot spots (spatial clusters with large values) and cold spots (spatial clusters with low values), the GOG statistic was used (Equations 2-1 to 2-3):
Where Xj is the value for element j, Wij denotes the spatial weight between the elements and each of i and j, and finally n represents the total number of elements. Moreover, the value of this statistic ranges from ┬▒1 to ┬▒3 at 90%, 95%, and 99% confidence levels.
Additionally, to evaluate the trend of disease hot spots, the Spatial Deviational Ellipse was employed (Equations 3-1 and 3-2):
(Equation┬Ā3-1)
In this equation, xi and yi are the coordinates of element i, and X ¯ Y ¯
Further, GWR was used for assessing the association between child mortality and income status of countries. This regression depends on the spatial coordinates (spatial and geographic weights), with their values and signs having spatial variability. The GWR formula is as follows (Equation 4):
In this equation, (vi, ui) forms the coordinates of the i-th point in space, ╬▓ (ui,vi) is a continuous function of K (v, u), and wherever ╬▓ is at each point of i, the explanatory variables of Xi1, ...., Xip are regarded as errors at points i and Ōé¼i. For the given data set of the regional parameters K (v, u), ╬▓ is estimated using the weighted least squares. The Wij weights in each position (vi, ui) for i = 1,2 ..., n are obtained as a continuous function of the intervals between points i and other data points.
Results
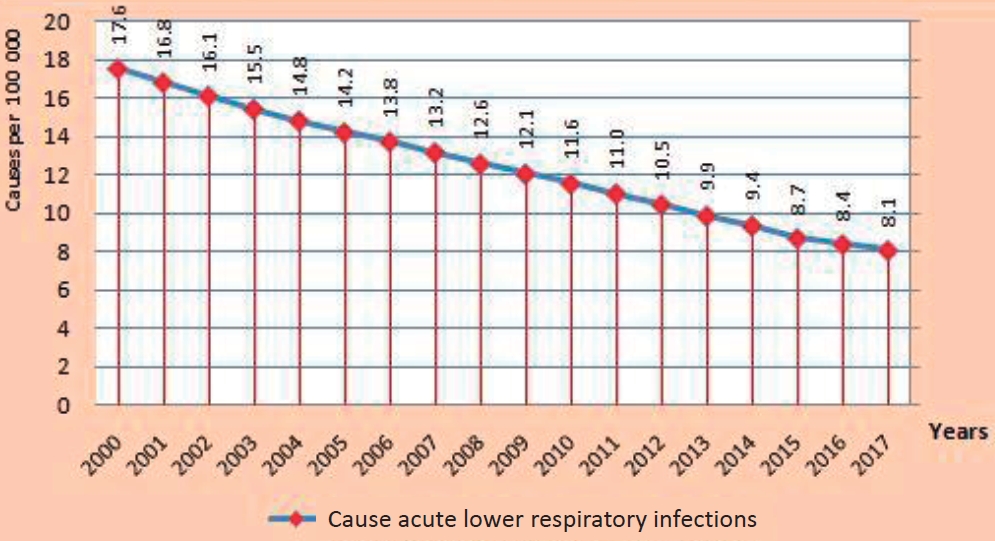
In Fig. 1, between the years 2000 and 2017, child mortality showed a downward trend from 17.6 per 100 000 children to 8.1.
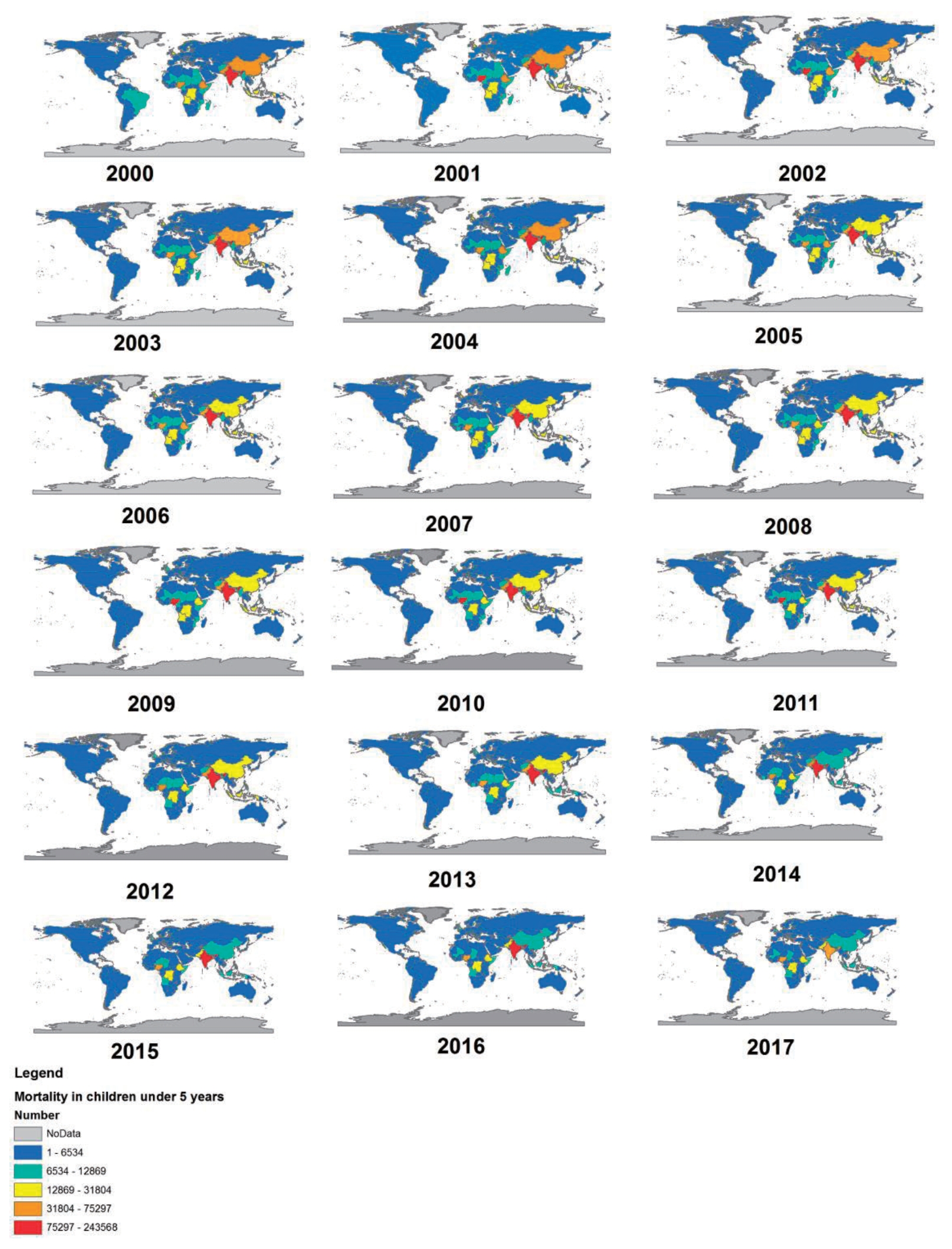
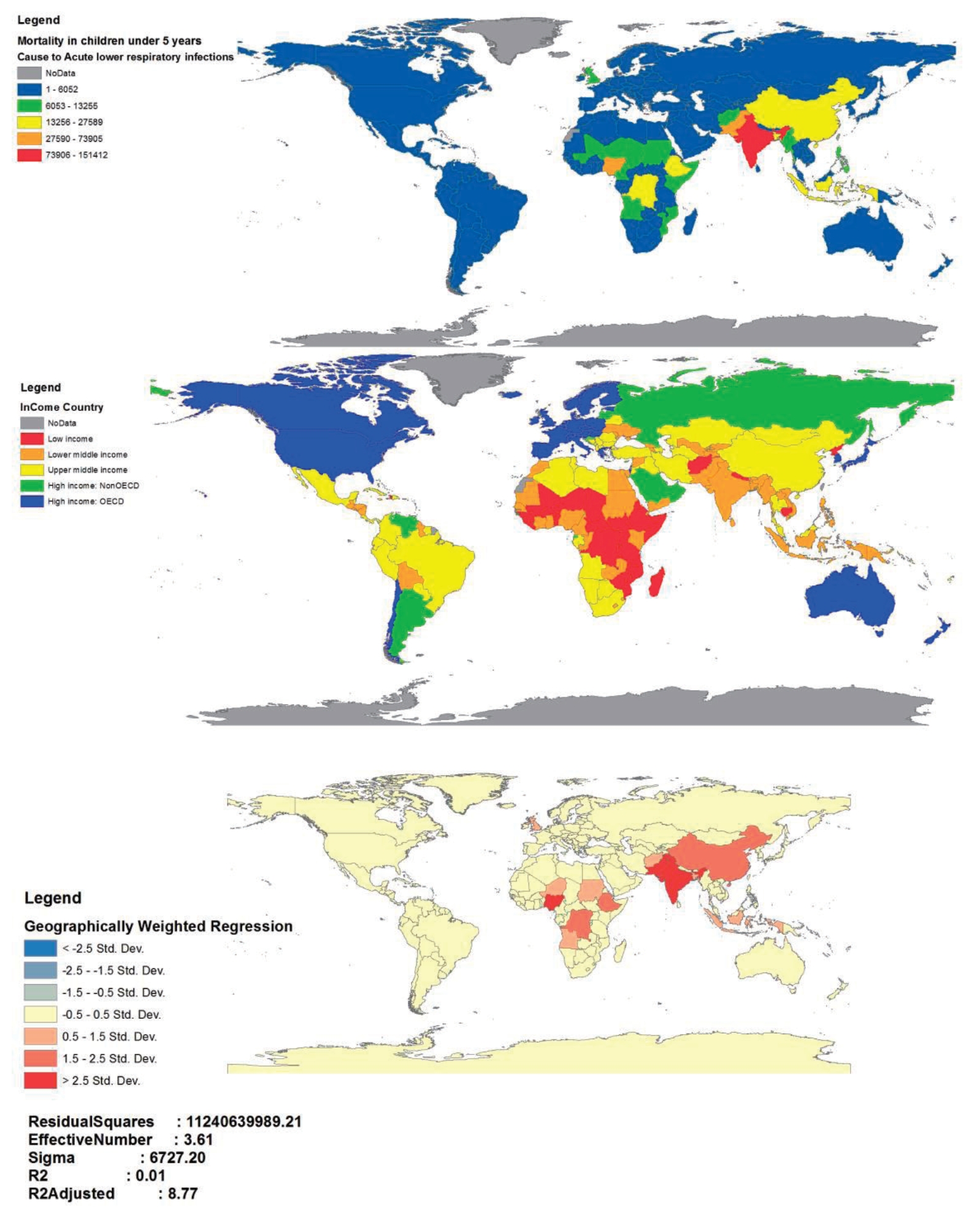
Fig. 2 shows the trend of mortality from ALRI in children under 5 years among countries. The countries with the highest and lowest numbers of mortality are in red and blue colors, respectively. Further, in 2000, the highest numbers of child mortality from the ALRI were in India, China, Afghanistan, Pakistan, Nigeria, and Ethiopia. However, India, Chad, Central Africa, and Nigeria had the highest numbers of child mortality from this disease in 2017. Based on Fig. 2, China experienced a decline from the orange level in 2000ŌĆō2004 to yellow in 2005ŌĆō2013, and then in 2014ŌĆō2017, it changed to light blue which indicates a significant reduction in deaths due to ALRI.
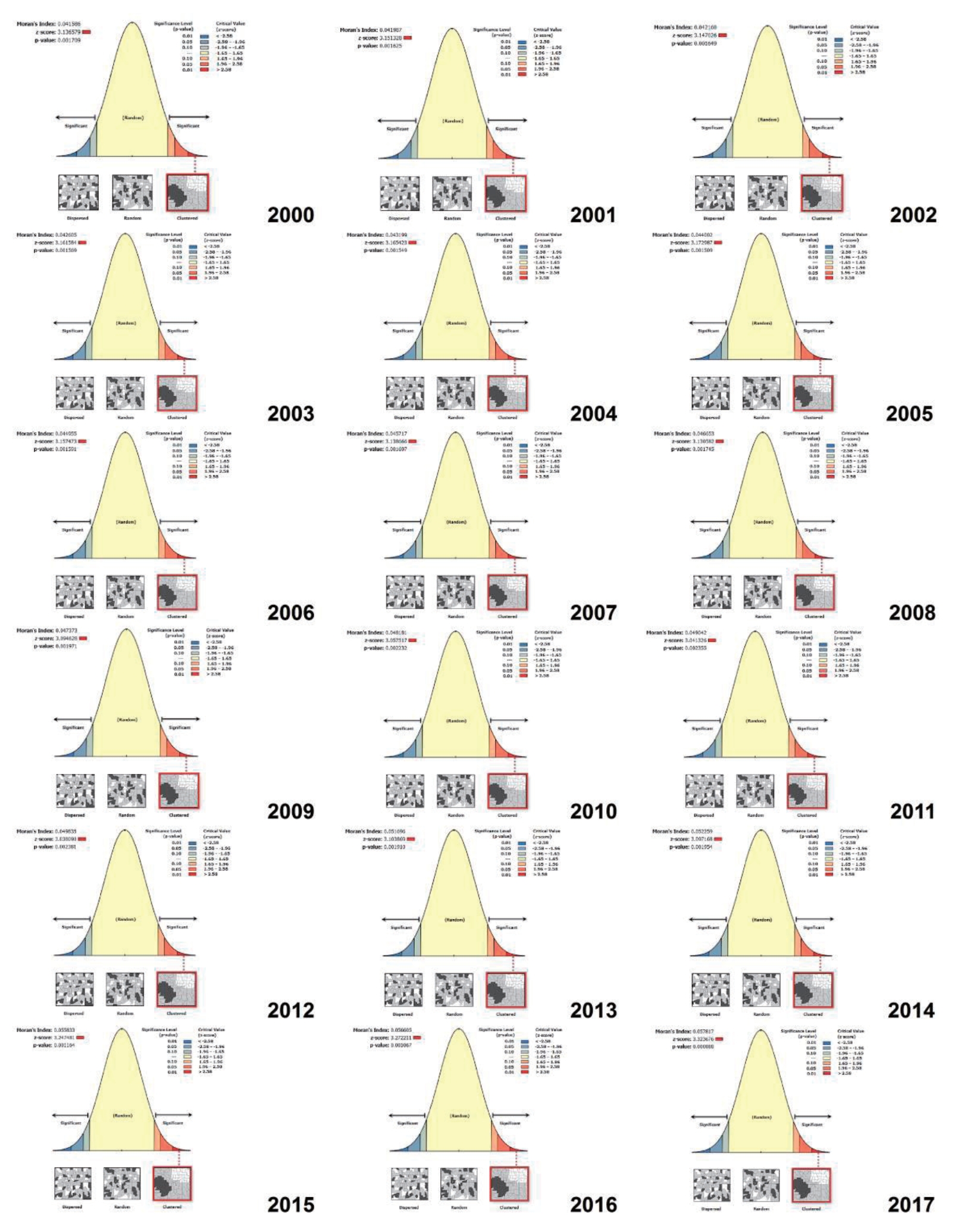
As shown in Fig. 3, the mortality of children under 5 years caused by ALRI has followed a clustered pattern over 2000ŌĆō2017 (MoranŌĆÖs I>0 and z score>2.58).
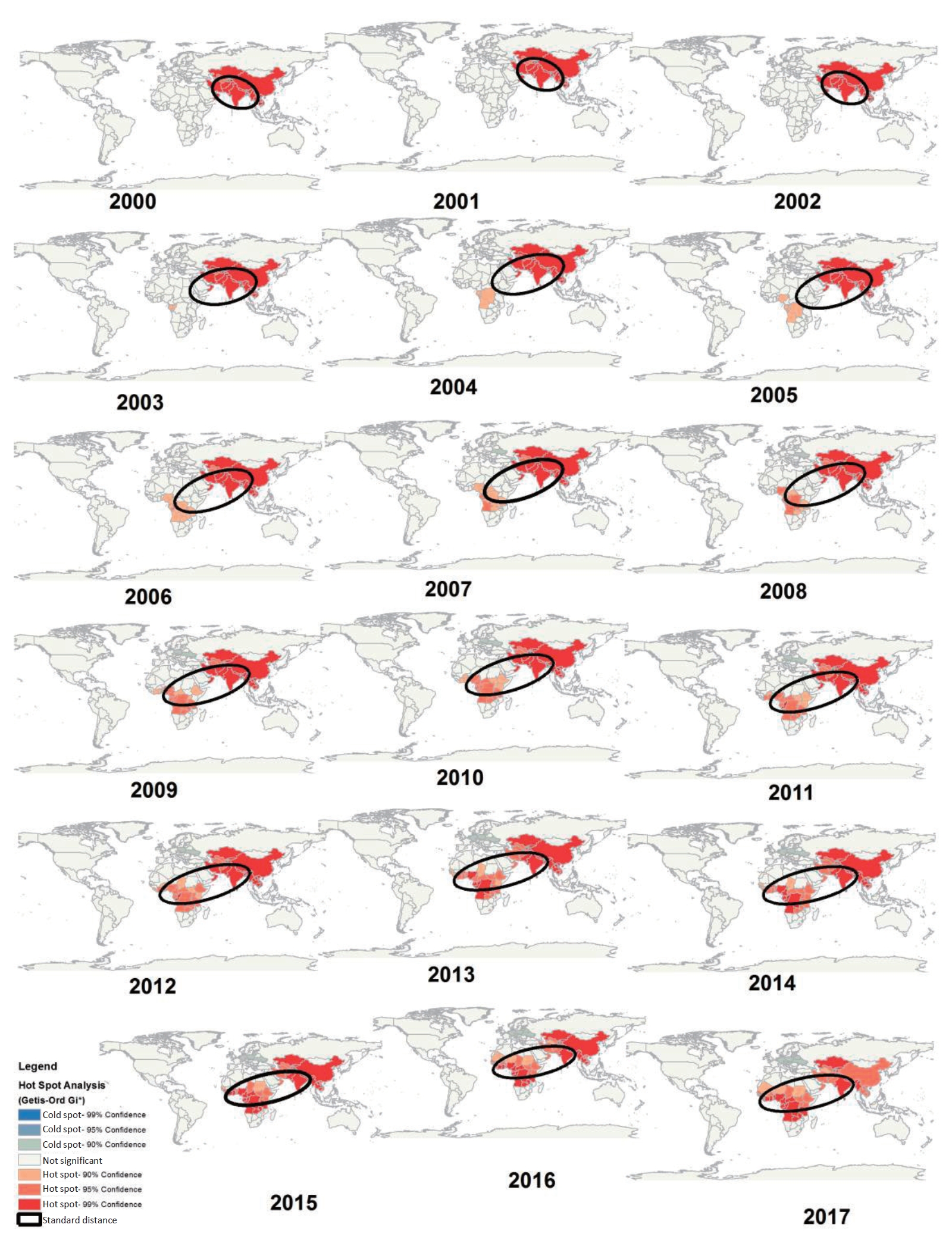
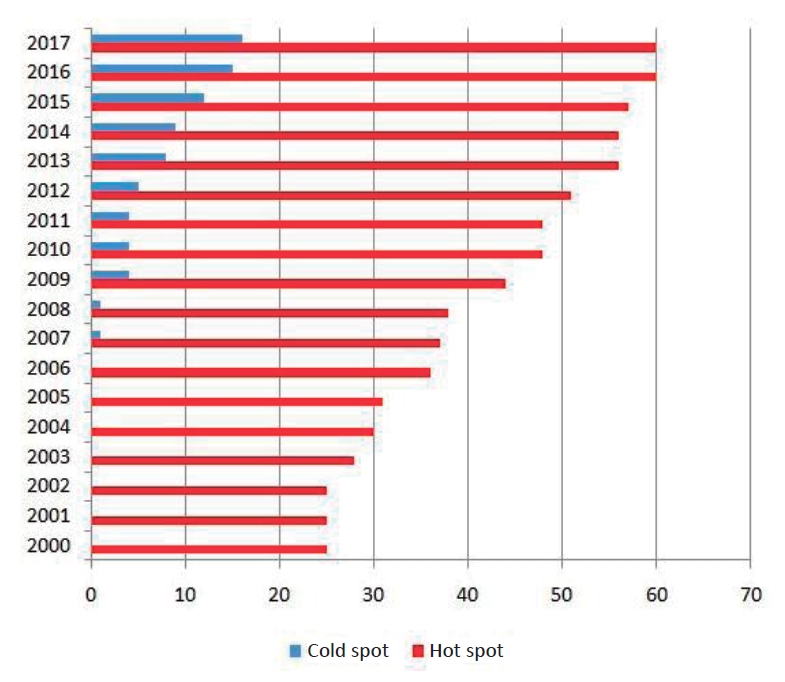
Fig. 4 shows the results of the GOG statistic for the identification of hot and cold spots of mortality of children under 5 years caused by ALRI at 90%, 95%, and 99% confidence levels. The results demonstrated that the hot spots were concentrated in Asia in 2000 (China, Thailand, Myanmar, India, Pakistan, Afghanistan, Kyrgyzstan, Uzbekistan, Turkmenistan, Kazakhstan, Iran, and Oman), while within 18 years, it drew towards the African countries (Angola, Tanzania, Zaire, Kenya, Ethiopia, Sudan, Chad, Nigeria, Cameroon, Congo, Central Africa, Mali, Ghana, Ivory Coast, Guinea, Senegal, Mauritania). It should be noted that a cold spot was formed in Europe from 2007 onward and followed an ascending trend by 2017. Based on the GIS maps, the direction of focal points has undergone changes, so that the direction has been northwest-southeast in the years 2000, 2001, and 2002, whereas changing in a northeast - southwest direction from 2003 onward. Other findings showed that in 2000, 25 countries were identified as hot spots, which increased to 60 countries in 2017 (Fig. 5).
As shown in Fig. 6, based on the results of GWR test, the regions identified as the hot spots of mortality from ALRI in children under 5 years were among the middle-income countries (R2=0.01, adjusted R2=8.77).
Discussion
The present study provides the spatial modeling of mortality from ALRI in children under 5 years residing in 194 countries over 2000ŌĆō2017. Based on the results, the total number of children mortality from ALRI followed a downward trend during the 18-year period of the study. This finding was consistent with the results of studies conducted by Roth et al. [8], B┼éa┼╝ejczyk et al. [14]. Although the results of the present study indicated a decrease in the number of child mortality, respiratory infections are still the third leading cause of childhood mortality [15], which should be addressed by health interventions. Therefore, there should be health plans and policies consistent with the aim of SDGs to reducing child mortality up to 25 per 1,000 live births by 2030 [16].
The results also showed that the mortality from ALRI in children under 5 years was clustered and had some foci in the world (Fig. 3). These results were consistent with those reported by Golding et al. [17] in Africa. Differences between countries can be due to climate [18], health infrastructure [19], urban traffic [20], latitude and longitude [21], low education of mothers [22]. In addition to the above-mentioned factors, indoor and outdoor air pollution [23] should be also considered which affects around 600,000 children around the world annually [3]. In a study conducted by Yu et al. [24], the effects of dust storms on Asian students' respiration were highlighted. In addition, Analitis et al. [25] studied the relationship between temperature and mortality from respiratory infections, in which 1┬░C rise in the temperature led to a 3.3% increase in respiratory mortality.
According to our findings, most of the hot spots of ALRI in children under 5 in 2000 were concentrated in Asian countries such as China, Thailand, Myanmar, India, Pakistan, Afghanistan, Iran, and Central Oman. During the18-year period of study, in addition to Asian countries, hot spots have spread to African countries such as Kenya, Ethiopia, Sudan, Nigeria, Chad, Congo, Central Africa, Ghana, and Mauritania (Fig. 4). A similar study by Reiner et al. [26], used Bayesian geostatistical modeling to estimate Lower respiratory infections (LRI) incidence, prevalence, and mortality in African children from 2000 to 2017. The results of that study showed that the distribution of LRI cases and deaths in Central Africa was higher than in other continental countries. Similarly, our study showed that in 2017, the death foci of ALRI were in Central African countries. However, the present study, which examined the trend of deaths in the world, showed the general picture of the morbidity situation caused by ALRI in different continents and suggested that the death foci have shifted from Asia to Africa. It should also be noted that in the study of Reiner et al. [26] both incidence and mortality were studied, but in our study, only mortality was examined. The results of the present study also were consistent with those reported by Golding et al. [17] in terms of the spread of the mortality hot spots towards the central and western parts of the Africa continent. It seems that the movement of children mortality hot spots from Asia to Africa over the past 18 years has resulted from various reasons, including the spread of the disease in developing countries [13], improving the death data registry system in African countries [27], global climate change [28], and environmental pollution and dust [29]. Accordingly, health policy makers should pay particular attention to several countries. One of these countries is India, which has had the highest mortality rates in the last 18 years, thus causing problems [23]. Furthermore, Chad and Central Africa, as the hot spots of mortality from ALRI, receive less funding from the international organizations for health [17].
According to the findings of the present study, new cold spots were formed in Europe 2007, and have expanded by 2017. In a study by Brownell et al. [30], the evidence pointed out the reduction of child mortality in high-income countries, which seems to be influenced by the income conditions and the level of development in the European countries [31].
Based on the results, the spatial direction of hot spots concentrated northwest-southeast in 2000 to 2002, whereas changing in a northeast - southwest direction from 2003 onward (Fig. 4). In the whole period under study, the spatial direction of hot spots overlapped in developing countries, and the common feature of countries with hot spots was their development status. The early diagnosis and treatment of respiratory infections among developing countries have also been emphasized by the WHO. For example, Bangladesh can be referred to as a model among developing countries that has implemented a systematic reporting in the country. The capability of this program is quick monitoring and access to electronic data for further analysis [13].
The results of the present study also indicated the increasing trend in hot spots of children mortality in countries, so that 25 countries were recognized as hot spots in 2000, which increased to 60 countries in 2017 (Fig. 5). However, child mortality rates have declined. Although, health policies seem to have been able to reduce mortality in children under the age of 5, but still in developing countries, the mortality due to acute respiratory infections is on the rise. In other studies, spatial distribution and clustering of respiratory diseases have been addressed such as Netherlands [20] and Iran [32]. Although the geographic area of these studies was not comparable to our research, they were similar in terms of using the same spatial statistics methods.
Based on the results of the GWR test, the countries that were introduced as the hot spots of ALRI in children were among the middle-income countries (Fig. 6). These results were consistent with the results of a study conducted in 17 countries of the Middle East and North Africa over 1980ŌĆō2010 [33] and a study carried out in 59 less-developed countries in 1991 [34]. Furthermore, in studies done by Sonego et al. [35], the relationship between low socioeconomic status and the risk of respiratory infections has been addressed. Given that the mortality of children under 5 years is expected to increase in middle-income countries [10], this will have important implications for services in middle-income countries, in addition to low-income countries. In addition, understanding the effects of the socioeconomic status of countries is complex and needs to be further explored. However, the present study can provide a suitable model for preventive decisions and the possibility of allocating resources.
One of the limitations of the present study was the use of secondary data, which made it impossible to investigate the quality of data for researchers. There were also differences in the methods of collecting information and estimates of the number of deaths in countries, which was beyond the control of researchers. In this study, the researchers failed to measure the effective factors and causes of ALRI on child mortality due to lack of access to specific indicators such as childrenŌĆÖs exposure to unhealthy weather, dust storms, and traffic across countries. Therefore, it is recommended that the data of mortality from respiratory diseases be collected with careful consideration and attention nationally and internationally.
In conclusion, the findings of the present study demonstrated that the total number of child mortality over 2000ŌĆō2017 followed a downward trend, while the number of hot spots increased among countries. It was also found that the mortality of children under 5 years caused by ALRI has followed a clustered pattern, and the situation has taken the form of hot and cold spots in different countries, drawing from the Asian countries (main hot spots in 2000) towards the African countries (over the 18 years under study). In fact, the present study allows the health planners and policy makers to use the GIS visual statistics, information, and rapid identification of the distribution of mortality from acute infections, rather than using the statistical tables that are difficult to understand. Moreover, health policy makers are recommended to pay special attention to countries that have been introduced as hot spots. It is also suggested that the relationship between child mortality from ALRI and climate change, dust storms, traffic and socioeconomic conditions be addressed in future studies.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


