


Introduction
Sinusitis is a well-recognized cause of both acute and chronic childhood headache, but isolated sphenoid sinusitis is a rare disease and its symptoms are often nonspecific and confusing. Thus a delay in diagnosis occurs frequently1,2). Although chronic severe complications are possible, sinus-induced chronic headache has a good prognosis if diagnosed and treated early2).
New daily persistent headache (NDPH) is form of chronic daily headache (CDH) that may have features of both migraines and tension-type headaches. NDPH is difficult to diagnose and requires a multifaceted approach3). NDPH is more frequent in children and adolescents than adults, and accounts for 1.7%-10.8% of patients with CDH cases in children and adolescents4). Infections are associated with NDPH and may provoke symptom5).
In this article we present two cases of children with isolated sphenoid sinusitis that caused symptoms of NDPH.
Case reports
1. Case 1
A 10-year-old boy was referred to headache clinic in Soonchunhyang University Seoul Hospital for evaluation of CDH. He had no family history of migraine. His first headache with diplopia had occurred 6 months previously, and he remembered the exact date. The patient described his headache as a dull, pressing sensation located in both parietal areas that was accompanied by photophobia and lasted about 4 hours. These events occurred nearly every day, and were occasionally not relieved by sleep. His CDH type was consistent with NDPH. The patient had trials of nonsteroidal anti-inflammatory drugs (NSAIDs) and topiramate, but these had no effects on his headaches.
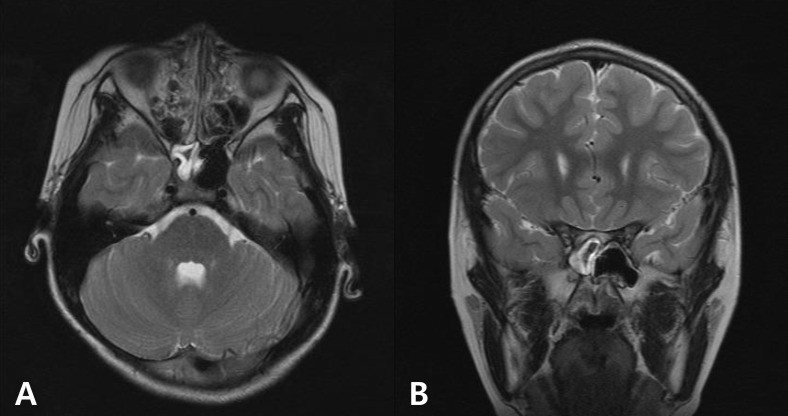
He denied any nasal symptoms or fever. Sinus percussion and examination of his cardiorespiratory and abdominal systems were normal. His vital signs were within normal limits. His neurological and ophthalmological examinations were normal. Routine blood work included thyroid function, inflammatory markers, complete blood count, virus study, and metabolic profile, and the results were normal. We did not check the cerebral spinal fluid (CSF) study. A brain magnetic resonance imaging (MRI) scan showed isolated right sphenoid sinusitis (Fig. 1). After oral antibiotic treatment for about 4 weeks, his symptoms resolved completely.
2. Case 2
An 11-year-old girl presented with severe headache with dizziness and nausea over a 6-month period. Her mother has a typical migraine history. The patient and her mother could recall the exact date that the girl's headaches began and that these had caused changes in her daily routine. The headaches affected both the periorbital and temporal areas, were constant and throbbing, and were exacerbated by head movement. The symptoms lasted about 4-5 hours and occurred every other day. Her chronic headache type was regarded as NDPH. She was given NSAIDs and amitriptyline, but the response was not good.
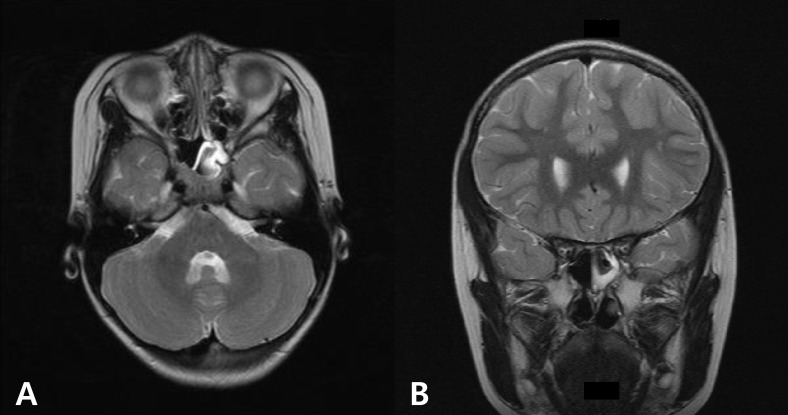
The patient had no nasal symptoms or signs of infection. Sinus percussion and neurological examinations were normal. Results of basic laboratory tests including a complete blood count, thyroid function, and infection markers were normal. A virus study that included Epstein-Barr virus was also normal. Her vital signs were within normal limits. CSF study was not performed. A brain MRI was requested to rule out intracranial pathology, and it revealed isolated sphenoid sinusitis (Fig. 2). After about 1 month of oral antibiotics for sinusitis, the patient's symptoms resolved completely.
Discussion
CDH is defined as a headache lasting more than 4 hr/day on more than 15 day/month for more than 3 months. According to the International Classification of Headache Disorders, 2nd edition6), NDPH is one of four types of CDH and comprises daily headaches within 3 days of onset that are unremitting for >3 months. Because most patients with NDPH complain of a headache that begins abruptly, they often remember the exact date the event started. Their headache subtype resembles tension-type overlapping typical migraine3). In general population studies, CDH is estimated to affect about 5% of adults and 1% of children and adolescents, and the prevalence of NDPH has been reported at 0.03%-0.1%7). NDPH has been reported in children and adolescents than adults3,7).
Patients with NDPH should have no symptoms of increased intracranial pressure or other neurological symptoms and no papilledema3). Any secondary headache may come on suddenly, as in NPDH, and it is important to distinguish between primary and secondary causes. Well-known secondary causes of NPDH are cerebral venous sinus thrombosis, carotid or vertebral dissection, vascular disorder, exposure to a toxin, temporomandibular joint disease, endocrine disorders such as Hashimoto's thyroiditis, sphenoid sinusitis, some virus infection and posttraumatic headache3). The clinician should apply tests such as routine blood work, thyroid studies, and assessment of erythrocyte sedimentation rate and the complete metabolic profile.
As a cause of secondary NPDH, isolated sphenoid sinusitis is rare in children and is difficult to diagnosis3,8). Most cases of isolated sinusitis have no nasal symptoms and signs of infection. The sphenoid sinus is often referred to as the "neglected" sinus because it is invisible to superficial examination and cannot be seen on standard endoscopy or plain radiographys9). Therefore, unless the physician has a high degree of suspicion of a sphenoid problem, the diagnosis can be missed for long time9).
The two patients presented with typical NPDH features such as frequent and prolonged headaches that began abruptly and that occurred on both sides in the periorbital area. They did not complain of nasal symptoms. The headaches had adversely affected their lifestyle, and their parents were concerned about the effects. The effects of NSAIDs and/or migraine drugs were poor. The patients' responses to the treatment of sinusitis with antibiotics were dramatic, and their symptoms resolved without complications.
Headaches are present in 85%-98% of patients with isolated sphenoid sinusitis10). The symptoms of headache are periorbital and temporal, worsen on bending forward, and characteristically involve the frontal and parietal regions3). According to the American Academy of Neurology practice parameters, neuro-imaging studies should not be done routinely in children with recurrent headaches and normal neurological examination results10). Despite these recommendations, neuroimaging is sometimes necessary in children. First NDPH or other CDH causes parental anxiety and impairs the patient's quality of life. Second, rare conditions such as isolated sphenoid sinusitis are difficult to diagnosis without brain computerized tomography scanning or MRI.
NDPH can cause sleep disturbances, dizziness, generalized weakness, visual disturbances, abdominal pain, and fatigue. Mood disorders, such as anxiety and depression, are also associated with CDH10). Some cases involve medication overuse and can contribute to frequent school absences. Thus, patients with NDPH should undergo multimodal evaluations, most of which will be clearly negative or positive3). There are still many unanswered questions about NDPH, and further study is needed to understand it better.
 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


