

Introduction
Adolescent "illness" is largely classified with either children or adult "illness". The notion of adolescent illness implies distinctive common psychosocial characteristics, rather than symptoms of physical disease or signs of illness1). The recent economic growth in Korea and the adoption of westernized dietary habits have affected the lifestyle of Korean adolescents accordingly. As the eating habits of adolescents have become increasingly westernized, average weight and height has increased, while a drastic downward trend in pubertal timing has been observed.
Diversified sources of information and constant technological advancements has been providing uncontrolled access of information for everyone. In particular, increasingly available adult content that exposes adolescents to smoking, drinking alcohol, and sexual experiences is progressively more becoming problematic as it creates psychosocial problems. It is important for doctors who specialize in this particular age group to consider and understand the significance of psychosocial factors that are related to risk-taking behaviors for the betterment of patient care and public health.
Demographics
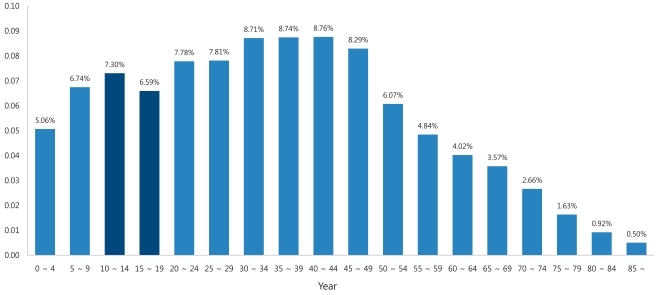
The average proportion of the adolescent population in developed countries ranges between 13 to 15%2). According to the 2005 Korean population census, the percentage of the population between the ages of 10 and 19 is 13.9% across the entire nation's population, which is consistent with numbers from other developed countries (Fig. 1). The definition of adolescent population used by the National Statistical Office in 2010 has differed at different times; however, overall, the population of people between the ages of 9 and 24 consists of 21.1% of the nation's population and the rate has consistently decreased since 1978.
As Fig. 1 illustrates, the notable difference between the Korean population and those of other developed nations is that the pediatric population (age, 0 to 9 years) comprises 11.8% of the total population, which is less than the total population of adolescents, while the pediatric population (age, 0 to 4 years) has decreased to 5.1%. This figure indicates that the adolescent population comprises the majority of the general patient populations of pediatricians, an important factor to consider for future implementation of adolescent health solutions.
Mortality
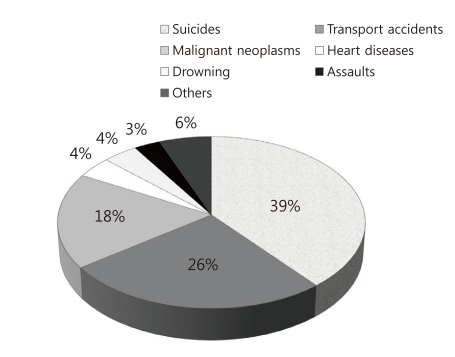
According to the National Statistical Office of Korea, the mortality rate of the adolescent population between the ages 10 to 19 decreased to 22.2 per 100,000 in 2009 from 38.2 in 1999. However, it showed an increment of 5.5% from the previous year. The major cause of death in the adolescent population is suicide, followed successively by transport accidents, and malignant neoplasm (Fig. 2)3).
From 1999 to 2008, the major causes of death in the adolescent (age, 10 to 19 years) population were, in order, transport accidents, suicides, and malignant neoplasm. The change in the major cause of death from transport accidents to suicide appears to be due to an increased rate of suicides. In 2008, the suicidal rate per 100,000 was 4.6, but increased to 6.5 people per 100,000 in 2009.
The primary causes of adolescent suicides are school-related problems such as stress from overwhelming academic responsibilities, mental health problems, lack of social support, and other socioeconomic issues.
Physical changes in Korean adolescents
The average height of a 12-year old Korean boy in 2008 was 158.1 cm, a 4.5 cm increase from 10 years ago (153.6 cm in 1998). The average weight has also increased by 4.9 kg, from 45.0 kg in 1998 to 50.8 kg in 2008.
There have been changes not only in physical indices but also in sexual maturation based on the Sexual Maturity Rating (SMR). In 1994, the average Korean female adolescent's first pubertal change, breast budding (SM2), occurred at the age of 11 years. Development of pubic hair (SMR2) took place at an average age of 12.9 years. For male adolescents, the first growth of testes (SMR2) occurred at an average age of 12.7 years, 1.7 years later than female adolescents, and development of pubic hair (SMR2) occurred at an average age of 13.2 years4). These figures were similar to British adolescents, where breast budding occurs at an average age of 11.2 years, and the first growth of the testes is at the age of 11.6 years5). These numbers illustrate the similarities between Korean statistics and those from developed western countries, with exception that Korean male adolescents begin pubertal development 1.1 to 1.5 years later than western male adolescents.
The current median age of menarche in Korean adolescents is 12.8 years, 1 year earlier in 19826). Comparisons with other studies show that, in the last 10 year period, menarche has occurred earlier each year. In 2009, the mean age of menarche was 12.47) this trend of menarche occurring at an early age was evident from results presented by Kim et al.8) in 2010.
The increase in the rates of sexual experience, and decrease in the average age of first sexual experience, is causally associated with earlier pubertal changes.
Exercise, diet and obesity
Due to the recent economic growth in Korea and improvement in diet, the problems of excessive caloric intake, nutritional unbalance, and lack of exercise have intensified throughout the population, there has been a consistent increase in the number of overweight or obese individuals in the population.
Korean adolescents often face excessive competition for school entrance exams, leading to an increase in the frequency of sedentary activities that prevents physical activity and causes significant adolescent health risks. In addition, their busy daily schedule causes irregular dietary habits and increased consumption of fast foods, and carbonated drinks, resulting in inadequate nutrition and lack of a healthy diet for adolescents. Mental instability from excessive academic stress is another factor that may cause adolescent weight gain leading to obesity, which negatively affects the quality of life and is a cause of early death when obesity continues through adult life.
1. Exercise and diet
In 1999, 57% of adolescents in Australia reported a lack of physical activity including 23% who never exercised9). In Korea, 19% of adolescents have never exercised, and notably, 29% of adolescents who participated in regular exercise did so for less than 1 hour10).
In 2009, 31.6% middle school and high school students in Korea reported performing vigorous physical activity for 20+ minutes 3 or more days per week7). Of high school students, who have a significantly higher academic workload, 9.1% reported that they do 60+ minutes of moderate physical activity 5 or more days a week, while 37.0% of U.S high school students reported that they performed considerably more physical activity than Korean high school students11).
Twenty-seven percent of Korean adolescents did not have breakfast for 5 days in a row and 66.5% consumed carbonated drinks more than once during the week. This figure is lower than the previous year's statistics since the implementation of the new policy against "the sale of carbonated drinks at schools" in 2006.
Additionally, statistics reveal that 60.6% of adolescents consume fast foods such as junk food at least once a week; this statistic was low, until 2008 but has increased by 4.5% subsequently. The percentage of the adolescent population that received education about nutrition and dietary habits was only 28.1% in 2009, significantly lower than 45.6% in 20067).
2. Obesity
The rate of prevalence of obesity in Korean adults was 26.3% in 1998, increasing to 31.5% in 2005. The rate of obesity in Korean adolescents also increased from 8.7 to 16.0%12). In 2009, 8.2% of the adolescent population was considered obese; this figure has stayed consistent since 2007. Male adolescent obesity was 11.5% and female adolescent obesity was 4.4%. The percentage of the overweight population (based on a body mass index [BMI] above 85 percentile and below 95 percentile) was 3.5%7).
In the case of Korean high school students, 9.7% were considered obese whereas 12.0% of U.S high school students were considered obese11). Moreover, 32.6% of those identified as obese attempted to lose weight within 1 month.
A research survey in 2010, high school students indicates that 12.0% of male and 4.0% of female students were considered overweight (BMI, 23 to 25). The survey further found that 10.7% of male adolescents and 3.0% female adolescents were classified as obese (BMI >25)13).
Mental health
The increasing number of adolescents faced with mental health problems is a growing problem worldwide. In the state of Minnesota in the U.S., 57% of the adolescent population faced intervention based on mental health issues at least once in 200614). Further, 10 to 20% of adolescents are faced with mental health problems or disorders and their mental disorders might lead to the onset of adult depression15).
In case of Korean adolescents, an excessively competition-oriented education environment, sudden changes in socio-cultural values, and the introduction of foreign cultures are constantly preventing them from building firm personal values and independent thinking. Depression, drug addiction, smoking, wrongdoing, bullying, social isolation, addiction to the internet or computer games and maladjustment behaviors are becoming obvious social problems among Korean adolescents. According to the Seoul Child and Adolescent Mental Health Center, 35.8% of 2,664 participating adolescents have exhibited mental health problems16).
According to statistics from the Ministry of Health & Welfare, 43.2% of Korean adolescents are faced with severe stress while the corresponding number for adults is 28.9%. It was discovered that female adolescents faced more stress than male adolescents. This study also revealed that 37.5% of participants had experienced severe depression for at least 2 weeks during the previous 12-month period. Compared to 26.1% of U.S. high school students experiencing depression, more Korean students exhibited symptoms of depression7,11).
Suicide: Previous research findings suggest that hopelessness, daily stress, alienation, depression, lack of self-esteem, lack of self-identity, inadequate social support, and psychological construct are all causative factors for suicide17). In 2006, 32.6% of Korean adolescents had thoughts of suicide and 3% (135 individuals) admitted to attempting suicide18). Another study revealed that 19.1% (15.2% of males and 23.5% of females19) of Korean adolescents had thoughts of suicide in the past 12 months and 4.6% had actually attempted suicide.
Substance use
The recent increase in adolescent use of alcohol, tobacco and other illicit substances poses a health threat for adolescents. A survey in 2009 revealed that, Korean adolescents admitted to using drugs and other illicit substances for personal reasons other than for the treatment of illness. The list of abused substances includes analgesics (49.3%), cough and cold remedies (43.3%), alcohol (37.7%), tobacco (17.6%), tranquillizers and sleeping pills (4.8%), stimulants (2.6%), medicine for Attention-deficit hyperactivity disorder (2.5%), diuretics and diet pills (1.7%), and hallucinogenic inhalants (1.3%)19).
As the Korean drinking culture is generous and hospitable, early adolescent drinking habits pose a serious health treat, cultivate unhealthy drinking habits, and increase the risk of inhalation of super-adhesive agents, leading to deviant behavior. The rate of cigarette smoking among Korean adults is among the highest of the nations in the Organization for Economic Co-operation and Development. As the adolescent rate of cigarette smoking is closely related to the adult rate of cigarette smoking, it is important to note the relationship between the two figures.
Smoking during the adolescent period causes delayed physical growth and respiratory disease, and is harmful for the development of mental health. Smokers are more likely to experience depression or harbor thoughts of suicide than nonsmokers. They are also often faced with higher stress levels, causing and increased occurrence of depression and, anxiety disorders20). Past smoking experiences increase the likelihood of future smoking in adolescents, depending on the smoking status of parents or friends21).
1. Drug
According to a study in 2006, 2% of adolescents have used an illicit substance including inhalation of super-adhesive agents and smoking cannabis18). The rate of substance abuse in Korean secondary school students is 0.7%, with the rate in male and female students being 0.9% and 0.4%7). Compared to the figure of 36.8% of high school students in other developed nations who use marijuana and cocaine, the rate of substance abuse among Korean adolescents (6.4%)11) is considerably lower.
2. Alcohol
A study carried out in 2001 shows that 62% of adolescents consume alcohol10). Further, a study by Bae18) in 2006 indicated that 73.7% of Korean adolescents had consumed alcohol.
Twenty-one percent of Korean adolescents indicated that they have consumed alcohol use in the past month, and the breakdown of the respondents was 23.7% male and 18.2% female. In the case of high school students, 29.1% admitted to alcohol use in the past month, lower than the corresponding statistic of 41.8% from U.S. high school students7,11).
The average age of initial alcoholic consumption was 13.2 years; the average ages for male and female were 13.1 years and 23.7%, respectively. Approximately 33% of adolescents were exposed to high-risk drinking, with male adolescents at higher risk. Approximately 40% of adolescents who use alcoholic beverages exhibited more than 2 behavioral problems after drinking7).
3. Smoking
In 2006, a study in Korea indicated that 71.6% of adolescents had never experienced tobacco smoking, but 5.7% indicated that they smoke frequently18). The adolescent smoking population is increasing consistently every year and the average age of the first smoking experience is decreasing.
According to statistics from the Ministry of Health & Welfare in Korea, 12.8% of secondary school students have smoked cigarettes in the past month the occurrence is higher among male adolescents (17.4%) than among female adolescents (7.6%). 17.5% of high school students indicated that they smoked, about 2% lower that the corresponding statistic from the U.S.11). About 6.7% admitted to daily smoking; this figure has consistently increased since 2005 and currently 10.8% of high school students have admitted to daily smoking. The average age at the first experience of cigarette smoking was 13.1 years in 2006, which is considerably earlier than the figure from 19987).
Reproductive health
Adolescent sexuality issue is a growing problem as the number of adolescents who are sexually experienced before marriage is increasing. Their limited knowledge of contraception and of sexual matters, and attitudes, cause unintended pregnancy and sexually transmitted diseases (STD). These unintended pregnancies and STDs can cause physical as well as psychological and social damage in adolescents.
1. Sexual activity
According to a study that was conducted among high school students in Seoul in 2005, 16% of the survey participants were sexually experienced and 50.3% indicated that they did not use contraceptive methods. About 2.3% of female participants indicated that they had experienced pregnancy, and 71% had induced abortions22).
Additionally, a study that was carried out in Korea in 2000 revealed that 47.5% of female students aged 15 to 16 years were sexually active. Approximately 22.8% of students had been involved in a sexual relationship before the age of 13, and 11.5% had sexual relationships after the age of 1723).
In 2009, 5.1% of secondary school students admitted to experiencing sexual intercourse, with 7.1% of male and only 3.0% of female adolescents having experienced sexual intercourse. This figure is has not changed significantly since 2006. About 8.2% of Korean high school students were sexually experienced, whereas the corresponding figure was 46.0% among U.S. high school students11). The sexual experience rate was higher in students who attended a specialty high school than a conventional high school in Korea.
The average age at first sexual intercourse was 14.0 years; this has decreased since 2006. The rate of sexual experience before entrance into middle school is 1.1% in Korea, considerably less than in the U.S.
2. Sexually transmitted diseases
About 30% of the STDs that occur in the U.S. are contracted during adolescence. There are no statistics regarding adolescent STDs in Korea; however, we could assume that severity of the issue is minor, since the rate of sexual activity in Korean adolescents is considerably lower than in western countries.
3. Other sexual risk-taking behaviors
According to the "2010 Adolescent Statistics" by Statistics Korea, 96.7% of teenagers use the internet on a daily basis; 37.3% have watched pornography movies and 35.9% have surfed pornographic sites24). These particular statistics suggest that there has been 4 to 5% increment in the exposure to harmful mass media, which could lead to improper sexual behavior.
Risk-taking refers to the tendency to engage in behaviors that are potentially harmful or dangerous, and often threaten health; risk-taking that begins during adolescent period could lead to more severe health and social issues in adult life25). These behaviors include intentional or unintentional injuries, smoking, drinking alcohol, substance use, sexual behaviors, unhealthy diet, and lack of exercise. These risk-taking behaviors are a major cause of adolescent mortality and morbidity and some studies have shown that some of these risk-taking behaviors are evident in younger age groups than before26,27).
In the past, there has been a lack of resources to implement solutions to such issues, with only information, education, or counseling being offered. However, a recent series of studies regarding risk-taking behaviors has been conducted to analyze the cause and effect of individual, environmental, and situational factors of adolescents. As a result, awareness of the concept of adolescent health status and health promotion is on the rise among health issues10,28). Furthermore, it is important for pediatricians and doctors who treat adolescent patients to note the significance of cause and effect of risk-taking behaviors.
If an adolescent's risk-taking behavior is identified and treated at an early stage, it is modifiable; if treatment is not implemented at an early stage, these behaviors could cause various diseases and could be a cause of chronic morbidity. It is, therefore, important to identify the health status of adolescents for optimal public health. It is also important to increase the awareness of potential problems of risk-taking behaviors among adolescents to implement the promotion of health.
To prevent and reduce such risk, the Center for Disease Control and Prevention has established a Youth Behavior Risk Factor Surveillance System in the U.S. since 1990, while in Europe, Health Behavior in School-aged Children was implemented to identify health problems and its associated factors. The Ministry of Health and Welfare and the Korea Center for Disease Control and Prevention has conducted the Korean Youth Risk Behavior Web-based Survey since 2005; however, the data collected and the extent of analysis has not been sufficient in comparison to similar studies from institutions and organizations from developed countries. Therefore, particular attention on the part of Korean pediatricians and doctors who treat adolescent patients is needed.
Conclusion
During the adolescent period, they undergo rapid physical, emotional and, cognitive development, including the establishment of lifestyle and habitual routines that strongly influence adult health life. Therefore, it is important to build a healthy lifestyle and acquire a proper view of health during this period. If healthy habits and a proper view of health are not established, it could lead to risk-taking behaviors. Since such behaviors are a major cause of adolescent mortality and morbidity, these issues must be addressed with much care.
The recent rapid economic growth, and the earlier onset of physical, sexual, and psychological maturation among adolescents compared to many years ago, influences their health status. The incidence of weight increase, sexual maturation, drinking alcohol, smoking, sexual experiences, and other risk-taking behaviors is increasing, and adolescents experience these factors earlier. Therefore it is important to note that the risk-taking behaviors of adolescents are caused by individual psychosocial factors.
 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


