


Introduction
Prader-Willi syndrome (PWS) is a complex genetic disorder that results from the lack of paternally expressed genes in the chromosome 15q11-q13 region caused by a deletion of the paternal copy (70%), maternal uniparental disomy (UPD) (25%), an imprinting center defect, or balanced translocation1,2,3). The estimated prevalence of PWS is difficult to ascertain, but several studies suggest that it is one in 10,000-30,000 live births4,5). PWS is characterized by atypical facial features, hypotonia, feeding problems, developmental delays, hypogonadism, short stature, obesity, and behavioral and learning disturbances3,6).
PWS patients are troubled with growth hormone (GH) insufficiency3). Therefore, GH treatment is used to improve body composition and growth during childhood. Reports have demonstrated that GH treatment in older PWS children has resulted not only in a remarkable growth response but also in a dramatic improvement in body composition, with a decline in fat percentage and an increment in lean body mass (LBM), resulting in increased muscle strength and agility3,7,8). Several studies on psychomotor development in PWS infants have demonstrated the improvement in body composition, motor development, and cognitive development during GH treatment8,9). Although there have been several reports on the clinical characteristics and the effects of GH treatment on PWS patients10,11), few reports have compared GH treatment effects according to gender and age at the start of GH treatment in Korean PWS patients. Therefore, the primary object of this study was to delineate the clinical manifestations of Korean PWS infants and toddlers and examine the effects of GH treatment according to gender and age at the start of GH treatment at a single center.
Materials and methods
1. Patients
We retrospectively analyzed the medical records of 30 patients with PWS (16 boys, 14 girls) who were diagnosed using molecular genetic testing, including methylation specific polymerase chain reaction and fluorescence in situ hybridization, as well as their clinical features at the Endocrinology Department of Pusan National University Children's Hospital between March 2009 and August 2013. In addition, microsatellite analysis was performed to confirm the UPD in nondeletion individuals. Among 30 patients with PWS, 22 patients were treated with recombinant human GH (Genotropin, Pfizer, New York, NY, USA). Among individuals under two years of age, GH treatment was started at a low dose, such as 0.25-0.30 mg/m2/day or 0.009-0.012 mg/kg/day and increased during the first weeks and months to reach the standard replacement GH dose of approximately1.0 mg/m2/day or 0.035 mg/kg/day, administered in daily subcutaneous injections, and only 14 patients (eight boys, six girls) received GH treatment for more than two years.
2. Methods
The patients visited the outpatient clinic for follow-up every three months and their height, weight, complete blood cell counts, routine chemistry, and thyroid function were checked. Height was measured using a Harpenden stadiometer marked to the nearest 0.1 cm and weight was recorded to the nearest 0.1 kg with an electric scale. Supine length was measured in infants younger than three years of age. Growth was analyzed by calculating the height standard deviation scores (SDS), body weight SDS, and body mass index (BMI) SDS according to the 2007 growth reference of Korean children and adolescents by the Korean Pediatric Society and Korea Centers for Disease Control and Prevention. Dual x-ray absorptiometry was used to calculate the body component ratio including LBM, fat percentage, bone mineral content (BMC), and bone mineral density (BMD). Height, body weight, head circumference, and BMI measurements were recorded before GH treatment and at intervals of 12 months thereafter. Psychomotor development was evaluated using the Denver developmental screening test (DDST) in GH treated patients with PWS by age at the start of GH treatment. Test results of psychomotor development were expressed as developmental age divided by chronological age and multiplied by 100, reflecting the percentage of the expected development (%ed) for that age. Changes in motor and mental development are expressed as percentage of change over 24 months (development at 24 months minus development at start, divided by development at start, multiplied by 100). Written consent was obtained from all participants who provided identifiable samples.
3. Statistical analysis
The Wilcoxon signed rank test was used to compare data before and after GH treatment. Mann-Whitney analysis was used to assess the effects of GH treatment according to gender and age in 14 patients with PWS. Differences were considered statistically significant when P<0.05. All statistical analyses were performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA).
Results
1. Clinical characteristics in PWS patients
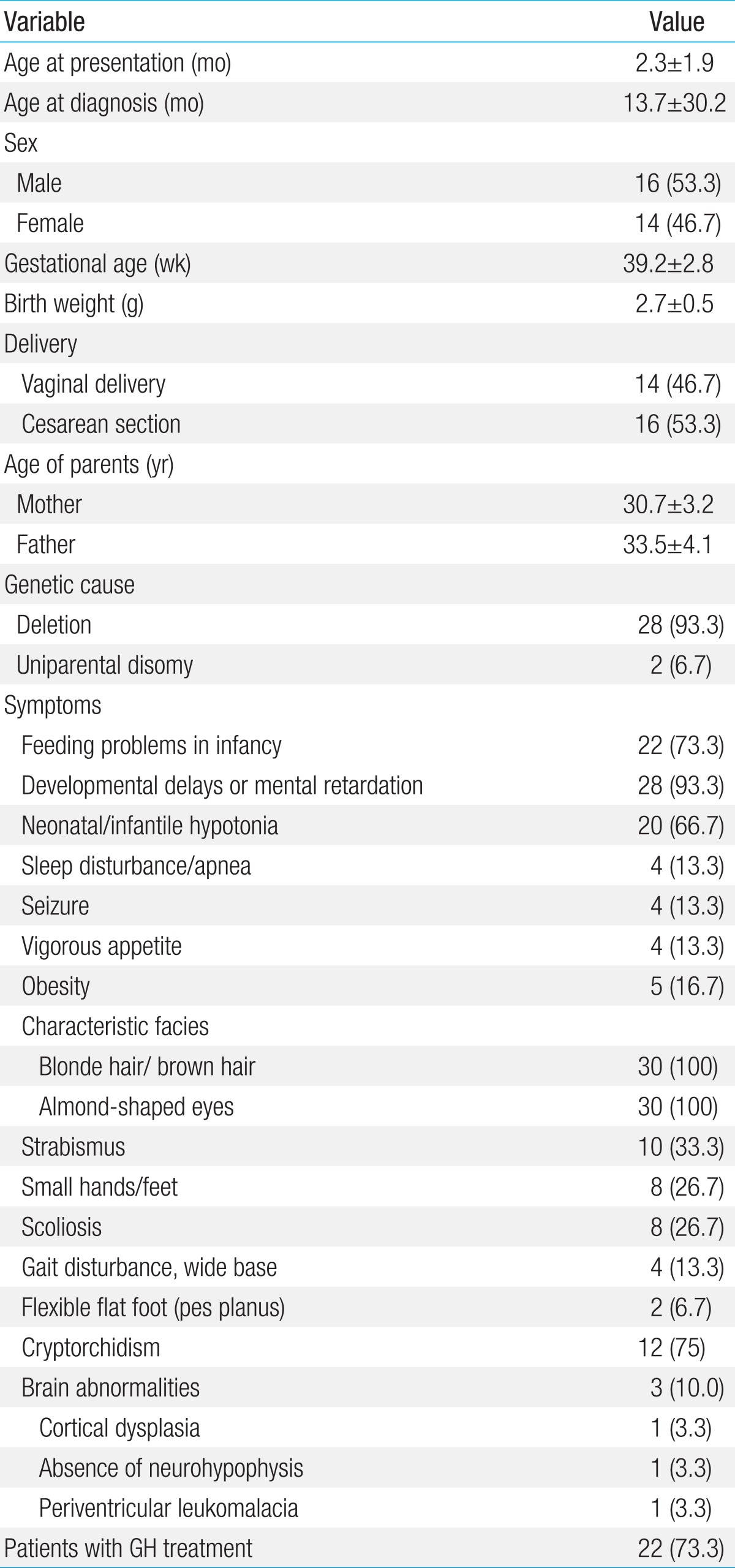
Thirty patients were diagnosed with PWS during a period of four years and six months. The sex ratio had a similar proportion of females and males: sixteen patients (53.3%) were male and fourteen (46.7%) were female. The mean age at presentation was 2.3 months (0-4.2 months of age). The mean age at the diagnosis was 13.7 months (2-47 months of age). The mean follow-up period was 3.5 years (2.3-4.4 years). Twenty eight patients (93.3%) had a paternal deletion, and the other two (6.7%) had a UPD. Phenotypic characterization of all patients was performed and is summarized in Table 1. All patients showed the characteristics of facial dysmorphism, including blond or brown hair, almond-shaped eyes, and a thin upper lip. Most patients showed developmental delays/mental retardation (93.3%), cryptorchidism (75%), feeding problems in infancy (73.3%), and neonatal or infantile hypotonia (66.7%).
Ophthalmologic problems were common, particularly strabismus (33.3%). The following brain abnormalities were present in three patients (10.0%): cortical dysplasia (3.3%), an absence of neurohypophysis (3.3%), and periventricular leukomalacia (3.3%). Skeletal abnormalities, including scoliosis (26.7%) and flexible flat foot (6.7%), were also observed. Obesity and seizures were also observed in five patients (16.7%) and four patients (13.3%), respectively.
2. Anthropometric data and IGF-1/IGFBP3 levels in GH-treated PWS subjects
The mean age at the start of GH treatment in the 14 PWS patients was 2.6 years (6.4-73.5 months). The mean treatment duration was 3.5 years (2.4-4.5 years). After two years of GH treatment, height -SDS (Ht-SDS) increased from -1.20±1.34 to -0.72±1.01 (P=0.056). Head circumference-SDS (HC-SDS) also increased from -1.81±1.30 to -0.77±0.83 (P=0.004). Body weight-SDS (Bwt-SDS) increased from -0.82±1.60 to -0.07±1.17 (P=0.048). LBM (g) increased from 10,156.55±6,330.24 to 12,272.52±4,379.82 (P=0.001). BMC (g) increased from 484.51±222.06 to 656.14±229.60 (P=0.001). BMD (z score) seems to increase from 0.39±1.22 to 1.00±1.12 (P=0.067). The body fat percentage tended to decrease from 34.72±8.00 to 32.42±7.86, but it was not statistically significant. IGF-I SDS and IGF binding protein-3 (IGFBP-3) SDS increased from -0.08±0.65 to 0.77±0.81 and -0.18±0.24 to 0.36±0.51 (P=0.002) (Table 2).
3. Comparison of GH treatment by age at the start of GH treatment
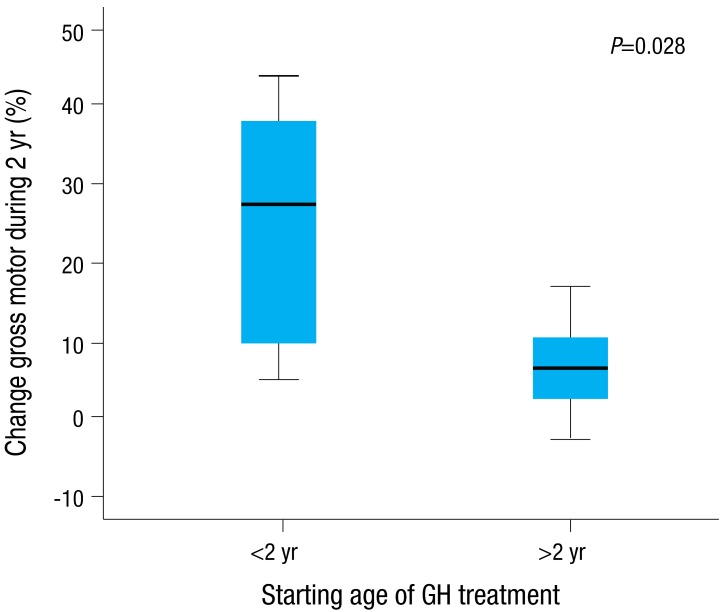
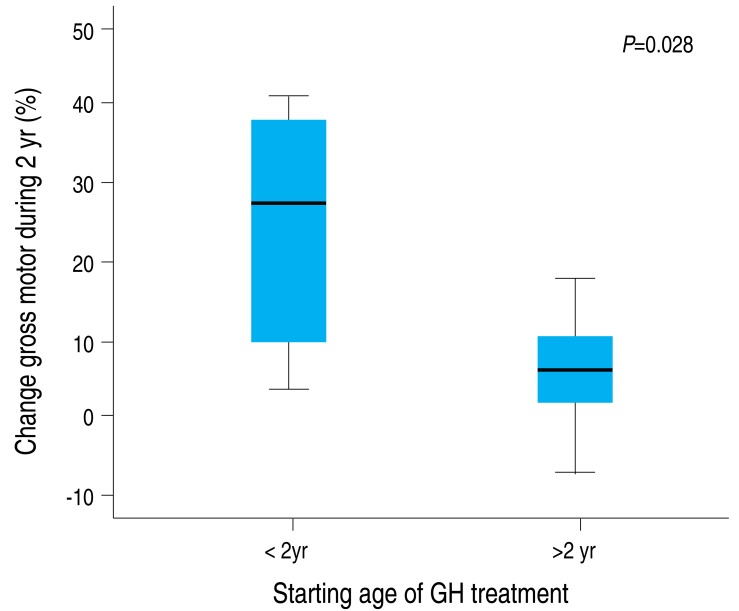
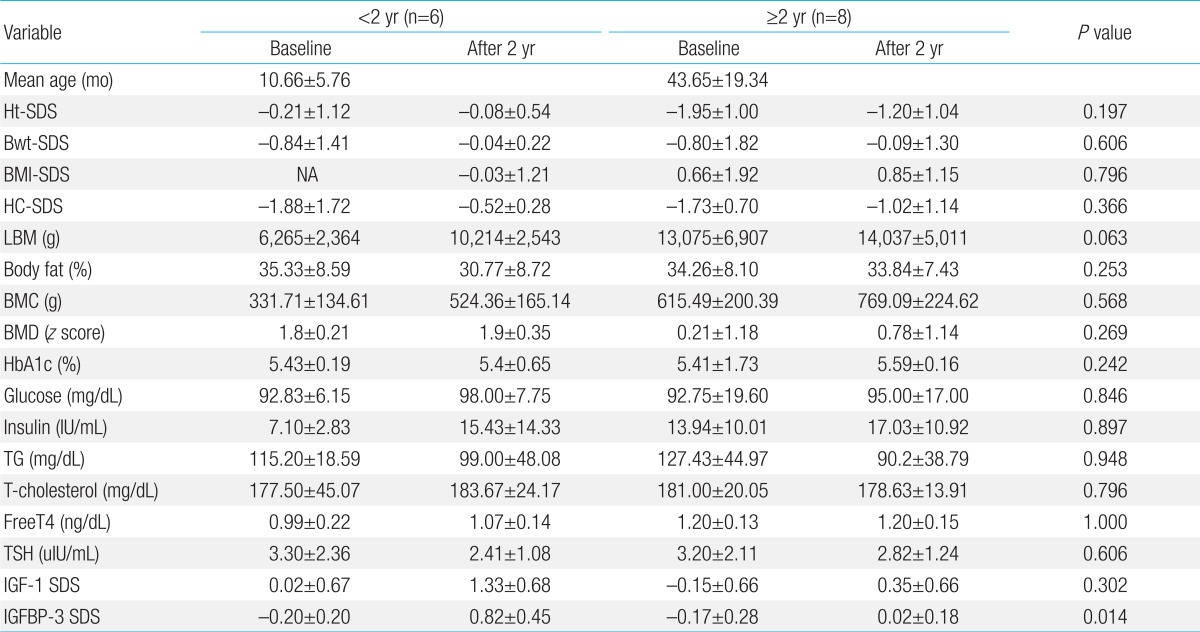
We compared the results of GH treatment for children under two years (n=6) (10.66±5.76 months) and older than two years of age (n=8) (43.65±19.34 months) at the start of treatment. There were significant increases in IGFBP-3 SDS among individuals under two years of age compared with individuals older than two years of age after GH treatment (P=0.014) (Table 3). Psychomotor data were obtained using the DDST in GH-treated patients with PWS according to the age of GH start (Table 4). The changes in both gross and fine motor development were observed during the second year of study among individuals younger than two years of age who obtained GH therapy: Change was from 62.37%±13.68% to 77.02%±14.97% (P=0.028) in gross motor development and from 63.00%±10.96% to 77.11%±11.63% (P=0.028) in fine motor development, respectively (Figs.1, 2).
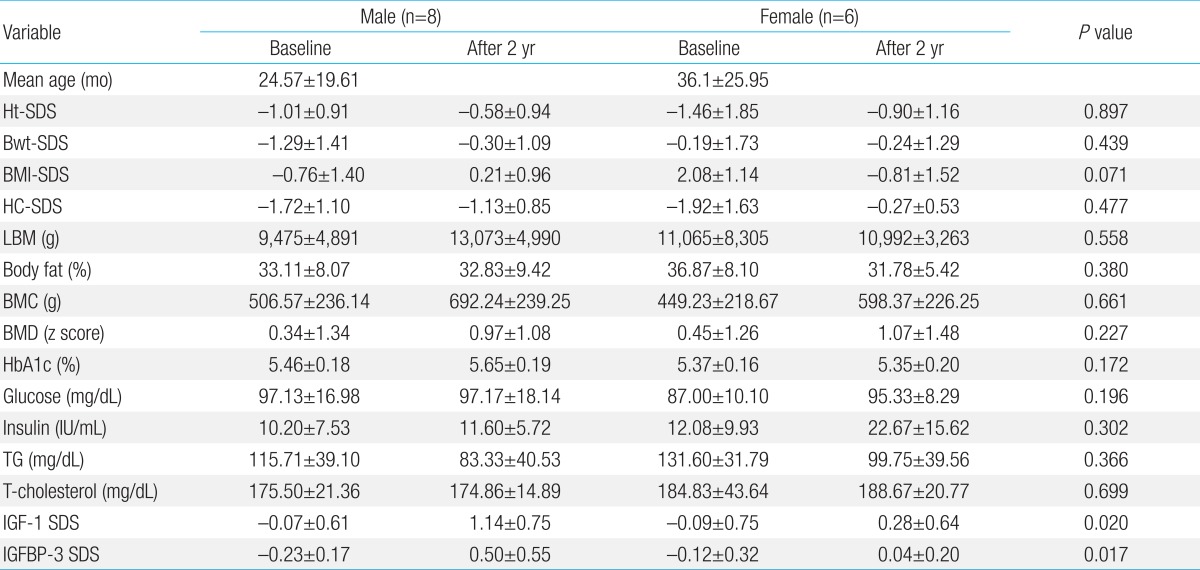
4. Comparison of GH treatment of PWS patients by gender
The efficacies of GH treatment for male and female patients with PWS were compared (Table 5), and there was significant difference in insulin-like growth factor-1 (IGF-1) SDS and IGFBP-3 SDS among male PWS patients.
Discussion
This study was performed to delineate the phenotypic characterization of Korean PWS infants and toddlers and assess their response to two years of GH treatment according to gender and age at the start of treatment, which would allow a comprehensive understanding of the natural course of PWS and the effects of GH treatment. PWS is characterized by a number of signs and symptoms11). In the present study, most patients showed developmental delays or mental retardation, cryptorchidism, feeding problems in infancy, and neonatal or infantile hypotonia. Of interest, strabismus, scoliosis, and obesity were infrequent (33.3%, 26.7%, and 16.7%, respectively). Perhaps this is because most of the patients enrolled in this study were infants and toddlers. In addition, seizures developed in four patients (13.3%) with PWS within one year of age and well controlled by antiepileptic drugs in all patients.
GH treatment in PWS has resulted in improved body composition (increase in LBM, lack of increase in fat mass) and cognitive function in those who have been treated11,12,13). In this study, increase of HC-SDS, Bwt-SDS, BMC, LBM, IGF-1 SDS, and IGFBP-3 SDS after two years of GH treatment in PWS infants and toddlers were observed. In particular, a meaningful increase in IGFBP-3 SDS was shown in PWS patients under two years of age when compared to those over two years of age after GH treatment. In addition, BMI-SDS seems to decrease more in PWS female patients than in PWS male patients after GH treatment.
Brain growth during infancy and early childhood seems to be more important than fetal brain growth in determining cognitive function8). After two years of GH therapy, we found a significant increase of HC-SDS in PWS patients. This suggests that cognitive function may improve in PWS patients treated with GH. However, a correlation between the changes in mental development and HC was not assessed. In the present study, PWS patients who received GH treatment when they were under two years of age seemed to have improved the language and personal-social development compared to those who received GH treatment when they were older than two years of age, although there was no significant correlation statistically.
Obata et al.14) showed that PWS males with GH treatment may have greater height increases than PWS females do with the treatment. Lin et al.15) compared the mean final height of male and female patients with GH treatment to those without GH treatment, finding 10.3- and 6.5-cm gains, respectively, after GH treatment. Although there was significant increase in IGF-1 SDS and IGFBP-3 SDS among male PWS patients comparing with female PWS patients in this study, further long-term follow-up research on the mean final height of male and female patients with and without GH treatment is required.
Reus et al.4) hypothesized that GH treatment could improve the effect of specialized physical training on motor development in patients with PWS. Motor problems in PWS patients are presumed to be related to an abnormal high fat muscle ratio. This ratio is important for overcoming gravitational forces and performing the stepping reflex. In PWS patients, however, from birth onwards, fat mass increases and muscle mass decreases16). In the present study, 6 patients under two years of age with PWS who received GH treatment have improved motor development compared to those older than two years of age who received GH treatment. Even if GH treatment has a preserving effect on LBM and BMC, it still has no proven effect on "functional" muscle strength17). Reus et al.18) also reported that noninvasive muscle ultrasound scans and functional magnetic resonance images should be conducted to gain more insight into the relationship between GH treatment and muscle strength. Therefore, additional research on muscle strength measurements using noninvasive methods before and after GH treatment in Korean PWS patients is needed. In addition, although LBM and BMC have increased in the present study, decreases in of body fat percentage and BMI-SDS were not shown in spite of two years of GH treatment. Therefore, it is necessary to control body weight and fat mass with lifestyle changes, diet, and exercise rather than GH treatment.
GH treatment is more often being initiated earlier than in the past. Reported results indicate that GH treatment in PWS has been advantageous when given at the age of 4 to 6 months of age8,19). However, no consensus has been reached on the ideal age of treatment initiation, although researchers have agreed on the benefits of treating before the onset of obesity, which often begins by two years of age5). Considering the increase in IGFBP-3 SDS and an improvement in motor development in PWS patients under two years of age after GH treatment in the present study, it might be beneficial to begin GH treatment as soon as possible.
Although we performed a comprehensive review of the clinical findings of PWS, our study has several limitations. First, the number of patients enrolled in the present study was too small and the period was too short to represent the general clinical spectrum and the effects of GH treatment on Korean PWS patients. Second, a prospective study is required to confirm these benefits due to the limitations of a retrospective study.
A previous study that was conducted in Korea reported increment of Ht-SDS, Bwt-SDS, and decrement of body fat percentage after two years of GH treatment in PWS patients older than two years of age11). Meanwhile, our study was the first to examine the effects of GH treatment according to gender and age at the start of GH treatment, as well as the clinical spectrum in Korean PWS infants and toddlers.
In conclusion, our study showed increases in IGFBP-3 SDS and an improvement in motor development among individuals under two years of age after GH treatment, and difference in IGF-1 SDS and IGFBP-3 SDS by gender. Much longer-term evaluations of a large number of patients are necessary to further investigate the effects of GH treatment in PWS infants and toddlers.


 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


