


Introduction
Wernicke's encephalopathy, first described in 1881 by Carl Wernicke, is an acute neuropsychiatric syndrome that requires emergency treatment to prevent death and neurologic morbidity caused by thiamine (vitamin B1) deficiency1,2,3). The classical triad of Wernicke's encephalopathy includes encephalopathy, oculomotor dysfunction and gait ataxia4). It is generally associated with alcoholism, anorexia nervosa and hyperemesis gravidarum which in turn induces thiamine deficiency5). In addition, it is also known to be related to prolonged parenteral nutrition without vitamin supplementation in systemic malignancy5).
Here we report a case of a 13-year-old boy who was diagnosed with Wernicke's encephalopathy derived from prolonged malnutrition during treatment for a neuroblastoma. He was treated with thiamine of 100 mg daily, and then of higher dosage (i.e., 500 mg three times a day) after 5 days. He was completely recovered after intravenous injection of high-dose thiamine.
Case report
A 13-year-old boy was diagnosed with neuroblastoma stage IV two years previously with no evidence of brain metastasis on initial cerebrospinal fluid study, and he received treatment 6 times with chemotherapy, as well as auto peripheral blood stem cell transplantation (auto PBSCT), therapeutic metaiodobenzylguanidine for residual tumor, and unrelated PBSCT for tumor relapse. When he was discharged from the hospital after successful unrelated PBSCT, he experienced increased nausea and vomiting, and poor oral intake. He was subsequently admitted to receive intravenous amino acid resuscitation (Trophamine) and total parenteral nutrition (TPN). When he was admitted, jitteriness on bilateral upper extremities was observed for a brief time while he was receiving intravenous amino acid resuscitation and TPN therapy. Under the impression of Wernicke's encephalopathy, intravenous thiamine replacement was done. Although his thiamine level came out to be normal (6.9 µg/dL; reference range: 2-7.2 µg/dL), we kept thiamine replacement therapy for one week since his oral intake was very poor. Then we changed intravenous thiamine replacement into oral replacement for one more month to prevent Wernicke's encephalopathy. Brain magnetic resonance imaging (MRI) was not performed since his thiamine level was within normal range then. Since he had no apparent neurological symptoms and his oral intake improved, we discontinued thiamine prophylaxis at discharge. The patient visited the outpatient clinic for reappearing nausea, vomiting and poor oral intake, and received TPN and intravenous amino acid resuscitation on a regular basis. Nonetheless, his symptoms did not improve and his general weakness increased. He was readmitted 3 months later.
One review of system, the patient had poor oral intake with nausea and vomiting, and he had lost 13 kg over 2 months. His initial vital signs were stable and his mental status was alert. Our initial physical examination did not reveal any abnormal neurological signs. Laboratory tests showed pancytopenia and elevated liver enzymes (The white blood cell count, hemoglobin level, and platelet count were 2,960/µL, 8.4 g/dL, and 139,000/µL respectively. His level for aspartate aminotransferase and alanine aminotransferase was 62 IU/L and 69 IU/L correspondingly).
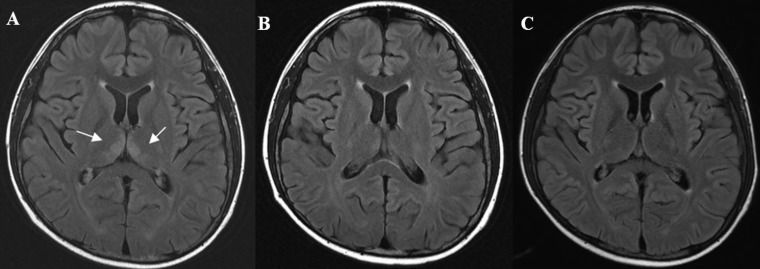
There were no specific findings from a brain MRI that was carried out on the day of admission in order to exclude brain metastasis. The patient received TPN replacement therapy while trying to develop his oral intake. On hospital day 7, he started to complain about dizziness, ataxic gait, and bilateral jerky type multidirectional nystagmus, but his mental status was alert and he did not show sensory changes in his extremities. On the evaluation of dizziness, neurological evaluation and consultation to Otolaryngology Department was done. His dizziness was not associated with spinning sensation, and it was nontrue vertigo type. He had no ear fullness or tinnitus, and his ear drums and hearing function were all intact. On neurological examination, his cranial nerve function test or deep tendon reflex test showed no remarkable findings, and rapid alternating test and finger-to-nose test also showed normal findings. On standing, he was slightly swaying to right side, but he had no unilateral motor power impairment. Consultation to the Ophthalmology Department was done, and there was no papilledema or diplopia on physical examination. His brain computed tomography was unremarkable. However, brain MRI showed hyperintense lesions in the bilateral medial thalami and periaqueductal gray matter was visible in T2-weighted and fluid-attenuated inversion recovery images, characteristic of Wernicke's encephalopathy (Fig. 1A). An electroencephalogram showed somewhat slow and disorganized background rhythms, which were compatible with mild degree of diffuse brain dysfunction.
Under the impression of Wernicke's encephalopathy, we started intravenous replacement of thiamine 100 mg daily. On treatment day 5, his symptoms improved slightly, but nystagmus and dizziness remained. We then increased the amount of thiamine replacement to 500 mg three times a day. Brain MRI at 9 days of thiamine replacement showed a slight improvement but the lesions remained (Fig. 1B). The patient's dizziness and nystagmus improved and disappeared upon treatment days 10 and 14, respectively. He was discharged with an oral thiamine supplement on treatment day 18. The patient's thiamine level was 1.5 µg/dL when he was first diagnosed with Wernicke's encephalopathy, but his thiamine level was over 9 µg/dL before he was discharged from the hospital.
His oral intake did not improve significantly after he was discharged, and he was readmitted to our hospital two more times for intravenous thiamine replacement although he did not complain of any symptoms related to Wernicke's encephalopathy. On that time, follow-up of brain MRI was performed, and the image was improving compared to the MRI when he was first diagnosed with Wernicke's encephalopathy. His brain MRI after two months of thiamine replacement was normal (Fig. 1C).
Discussion
Wernicke's encephalopathy is caused by thiamine deficiency primarily in alcoholics, and it can also occur in impaired nutritional
states including gastrointestinal disorders, hyperemesis gravidarum and malignant diseases5,6). Thiamine pyrophosphate is a cofactor of the pyruvate dehydrogenase complex, alpha-ketoglutarate
dehydrogenase, and transketolase. These enzymes play a key role in the regulation of glucose and energy metabolism in the brain. Therefore, when there is a shortage of thiamine, cells fail to meet their metabolic demands, and eventually it leads to metabolic acidosis, cell death, and external imbalance2,3,7). Brain tissue from patients with Wernicke's encephalopathy shows selective damage to subcortical areas of the brain that include the thalamus and mammillary bodies8). Oxidative stress, glutamate-mediated excitotoxicity and inflammation are major contributors to regional neurodegeneration in Wernicke's encephalopathy2).
A previous study detected the clinical triad of ocular symptoms, ataxia, and mental confusion in only 16% of Wernicke's encephalopathy
patients4,5). Another study reported that the classic clinical triad was present in only 0.4% cases at onset8). In our case, the patient showed dizziness, nystagmus and ataxia, but his mental status was alert until recovery. The relatively nonspecific nature of the clinical presentation may have delayed the diagnosis in many cases. Early signs and symptoms include loss of appetite, nausea, weakness, giddiness, diplopia, memory loss and difficulty in concentration. It is not until the later stage when the patient shows signs and symptoms of the classic triad, hallucination, and coma, yet early intervention with thiamine replacement is essential to reverse the symptoms of Wernicke's encephalopathy5,9,10,11). Brain MRI is the most sensitive technique and is required for all patients in whom Wernicke's encephalopathy is suspected. Medial thalami, mammillary bodies, tegmentum, periaqueductal region, and tectal plate are typical sites of abnormal MRI signals. The dorsal medulla, red nuclei, cranial nerve nuclei, cerebellum, corpus callosum, frontal and parietal cerebral cortex are less common sites of involvement although they are more frequently affected in nonalcoholic cases5,12). In our case, brain MRI revealed the involvement of bilateral medial thalami and periaqueductal gray matter.
Empiric thiamine replacement should be initiated as soon as Wernicke's encephalopathy is suspected. Delayed treatment may increase the likelihood of morbidity or mortality7). Patients require IV administration of at least 100 mg of thiamine daily for several days in Wernicke's encephalopathy10,13). However, in order to prevent permanent damage (i.e., Korsakoff syndrome), the British National Formulary and the Royal College of Physicians, London (Royal College of Physicians 2001) recommend the immediate treatment guideline for Wernicke's encephalopathy in alcoholics14). Thiamine 500 mg IV three times daily for 2 to 3 days and 250 mg IV daily for the next 3 to 5 days are recommended as immediate treatment14). However, there is no fixed guideline for pediatric patient who was diagnosed with Wernicke's encephalopathy. Dosage of 50-100 mg daily or 1.8-mg thiamine per 1,000 kcal has been suggested in pediatric patients, and 100 mg of daily thiamine replacement is routinely recommended in pediatric patients11,13). Furthermore, although high dose of thiamine replacement has not been documented in pediatric patients, high dose of thiamine therapy has been reported in nonalcoholic adult patient15). In our case, symptoms remained after use of 100 mg of thiamine when our patient was diagnosed with Wernicke's encephloapathy, so we increased the dose to 500 mg three times daily although Wernicke's encephalopathy was not alcohol induced. The patient was symptom-free after 1 week of high-dose thiamine replacement therapy. We prescribed him with oral thiamine on his discharge for supplementation. Furthermore, we have readmitted our patient for thiamine treatment therapy two more times after his discharge. Although he did not manifest a classical triad other than poor oral intake and general weakness, immediate replacement of thiamine helped him to recover his general condition.
In this report, we presented a case report of Wernicke's encephalopathy associated with prolonged malnutrition due to malignancy in a child. Since early diagnosis and optimal dosing is needed for complete recovery, it is important to suspect Wernicke's encephalopathy and replace thiamine actively although the initial symptoms may not be typical. Moreover, a high dose of thiamine (500 mg three times daily) should also be considered immediately in the pediatric patient with incomplete recovery from Wernicke's encephalopathy.
 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


