


Introduction
Accurate measurement of organ size is important in estimating adequate growth in children. Renal size is an important indicator not only to evaluate the children with renal disease, but also to determine adequate organ growth1-4). Renal size can be estimated by measuring renal length, renal volume, cortical volume or thickness. Despite the measurement of renal volume is the most accurate method to estimate renal size, the measurement of renal length is widely accepted because of its simplicity and reproducibility5,6).
There are several published reports about the renal length measurement by renal ultrasonography (US), but little is known about the renal length measurement using Technesium-99m dimercaptosuccinic acid (DMSA) scan7). Although renal US has been widely used to measure renal length in children, inter- and intra-observer variability exist6,8,9). DMSA scan is known more reproducible than renal US, and can also detect cortical abnormalities and assess renal function10).
In this study, we measured renal length with DMSA scan and established a simple equation for predicting renal length in Korean children.
Materials and methods
1. Patients and methods
This study included 700 hospitalized children who were clinically suspected with urinary tract infection and underwent DMSA scan at Konkuk University Medical Center from May 2005 to August 2011. DMSA scan were performed to the patients who had pyuria in urinalysis collected by urine bag, urine catheterization, midstream urine sample or took antibiotics prior to admission, after the fever subsided. The children with clinical pyelonephritis and presented renal scarring or culture-proven urinary tract infection were excluded. The patients were excluded if they had renal abnormalities on US or DMSA scan such as altered echogenicity, solitary kidney, multicystic kidney disease, hydronephrosis, vesicourethral reflux, acute nephritis, photon defect of kidney or renal scar. Patients with organ transplantation, renal surgery, failure to thrieves were also excluded. Medical records of 346 children who met inclusion criteria were reviewed retrospectively.
There were 148 boys and 198 girls. All those examined were divided into two age groups: less than 1 year old and 1 year of age or older. Because kidney growth were highest and most variable during the first year of life, but leveled off afterward.
Renal lengths were measured in both kidneys by assessing the maximum pixel length on DMSA scan. And the mean renal lengths was defined as half of the sum of the standard deviation scores in the right and left kidney. The mean renal length was used for further analysis, being referred to as 'Renal length' unless stated otherwise.
2. Statistical analysis
Data were analyzed by PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA). Differences in variables between the groups were compared using independent t-test, and the correlations between age and renal length were obtained using regression analysis and Pearson correlation analysis. The relationship between whole age group and renal length was assessed by power regression model. Using R2 as the criterion for comparing and choosing linear and nonlinear fashion, renal length less than 1 year old were statistically analyzed using a nonlinear model described; The group of 1 year of age or older was analyzed using a linear regression model of the general form y=ax+b. Values with P<0.05 were considered statistically significant.
Results
A total of 346 Korean children, 148 boys (42.8%) and 198 girls (57.2%), were included in this study. Their median age was 1.35 years with age distribution between 1 month and 17 years.
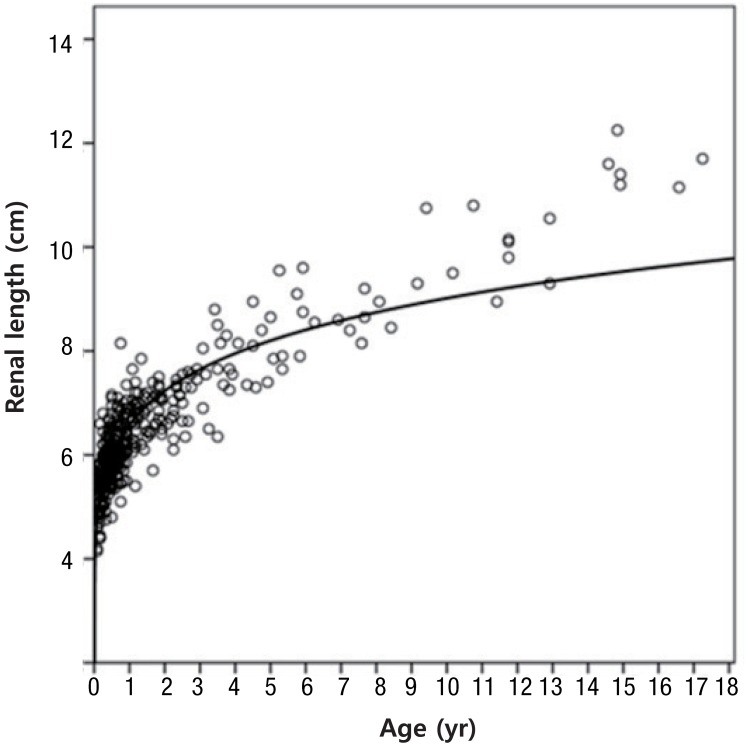
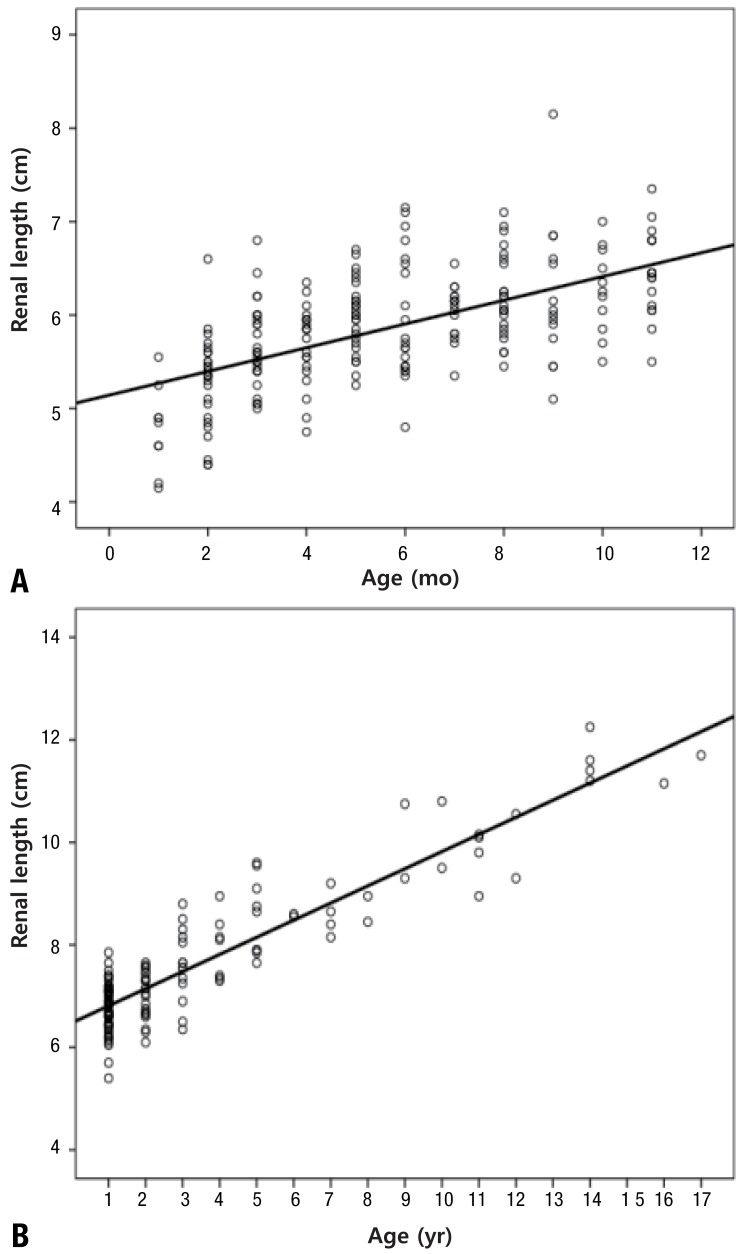
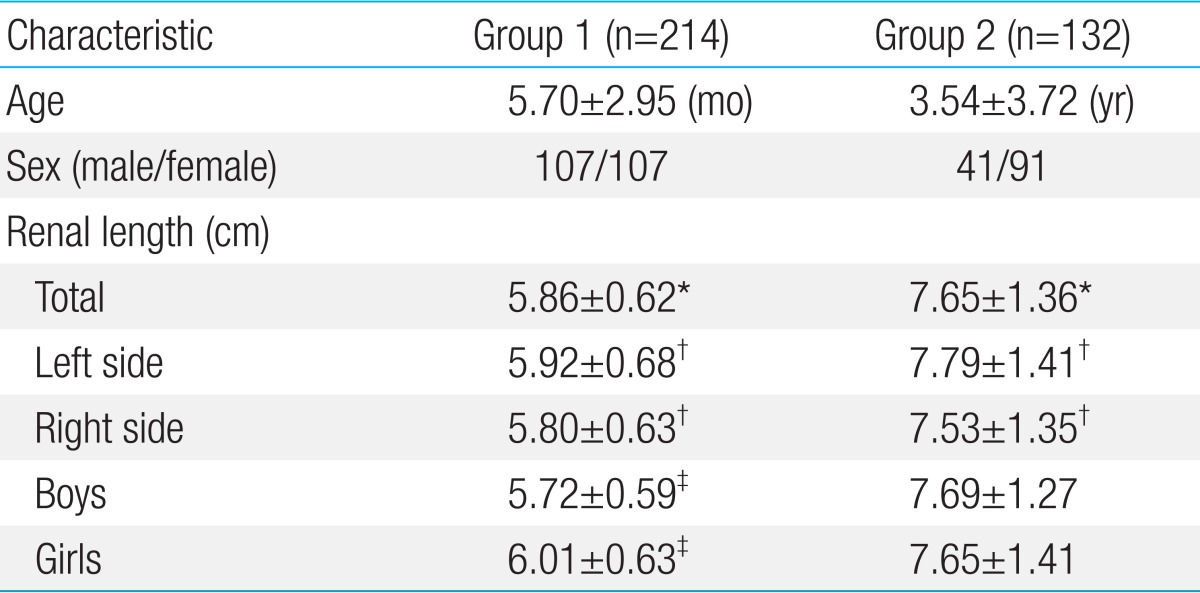
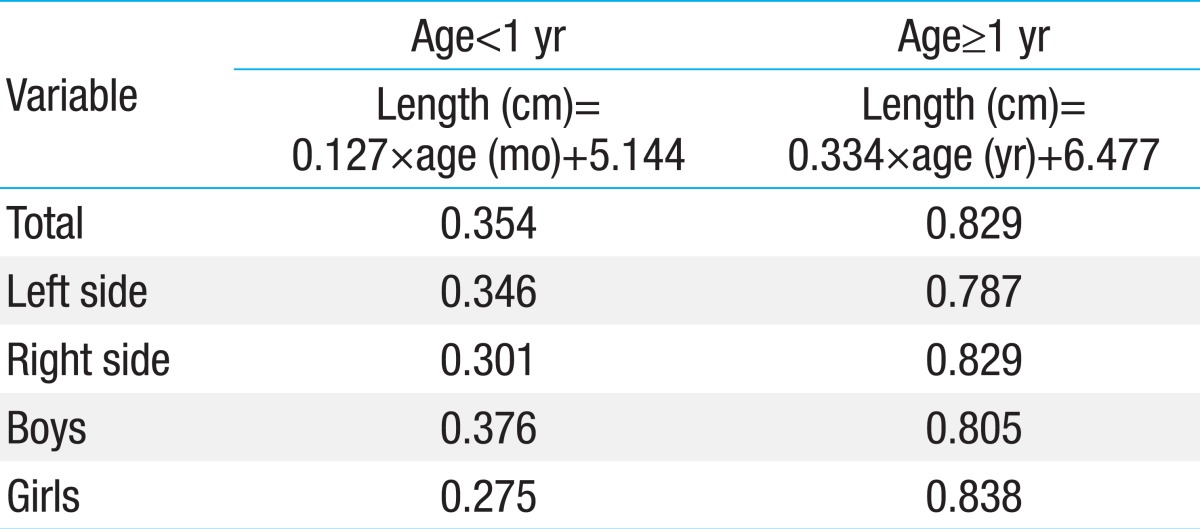
Children were divided into two age groups: 214 children (61.8%) were less than 1 year old (group1) and 132 (38.2%) were 1 year of age or older (group 2). Mean renal length was 5.86±0.62 cm in group 1, and 7.65±1.36 cm in group 2 (P<0.001) (Table 1). Renal length was larger in left side than right side (6.63±1.36 cm vs. 6.46±1.28 cm, P<0.001), and no statistically significant difference in size between the gender in group 2. Renal length increased with age (Fig. 1). Growth rates of renal length were highest during the first year of life, and then stabilized in a linear fashion after 1 year of age. From the data of the 346 children, the regression equation for renal length was produced as follows: 4.682×age (month)0.137, R2=0.780. In group 1, the formula was renal length (cm)=0.127×age (month)+5.144, R2=0.354 (Fig. 2A), and 0.334×age (year)+6.477, R2=0.829 in group 2 (Fig. 2B). Coefficients of determination (R2) were calculated overall group and separately for left kidneys alone, right kidneys alone, boys alone and girls alone. R2 values of subsets were presented in Table 2.
Discussion
In this study, we measured renal length with age using DMSA scan and produced a simple formula for predicting renal length in children (R2=0.780).The formula for the renal length were presented separately according to the age (1 year) based on the growth velocity of the kidney.
Accurate measurement of organ size is important in children to estimate the adequate growth. Renal size measurement is one of the important indicator to determine adequate growth and renal function1,2,11). Renal length can be measured by several modalities such as renal US, computed tomography (CT) scan, and DMSA scan5,12). CT scan has several disadvantages for children such as radiation exposure and potentially nephrotoxic contrast agent administration, therefore it is recommended as secondary diagnostic tools for further evaluation of renal lesions that are detected with other imaging modalities5,13). Renal US is one of the most common imaging method for assessment of visceral organ without any risk of radiation. There are many previous studies about measurement of renal length by US5,14-17). Although renal US has been widely used in children, inter- and intra-observer variability exists in measuring kidney size6,8,9,18,19). DMSA scan is known more reproducible and accurate modality than US in measuring renal length, as the maximum longitudinal renal axis can be more reliably obtained20). It can also detect cortical abnormalities and assess renal function21), and has less radiation exposure compared to CT scan7,10,20,22). Although DMSA scan is a useful tool for estimating renal size in children, a few studies has been published7,10,20,22). Several published studies have been suggested simple equations to estimate the renal size by US in normal Korean children23,24). But there is no reports with DMSA scan.
This study showed that left kidneys are larger than right kidney which was consistent with prior studies23,25).
Akhavan et al.25) proposed age-based formula for estimating renal length by US in children over 1 year old; renal length (cm)=0.278×age (year)+6.103 (R2=0.812). It is similar to our age-based formula that examined by DMSA scan. Lobo Sotomayor et al.7) proposed similar formula using DMSA scan; renal length (cm)=0.2644×age (year)+6.319 for children over 1 year old and 6.1727×age (year)0.1535 in whole age group. They are similar to our age-based formula in Korean children examined by DMSA scan. Further studies are required to establish age-based formula for estimating renal length and reference values using various modalities.
Our study showed that renal length increased with age, and the relationship between renal length and age was biphasic which consisted with previous report25). It is well known that most rapid renal growth occurs during the first year of life and then the renal growth rate finally stabilizes in linear fashion16,25,26). So the children were divided into two age groups: children less than 1 year old and children 1 year or older.
In this study, the renal length could be predicted with this linear equation in children older than 1 year of age (R2=0.829). Meanwhile, the ability of explanation of formula for renal length in infants was much lower (R2=0.354).Renal length is also influenced by intrauterine factors and gestational size during the first year of life16,25,27-29). Therefore, it is difficult to establish simple formula in infants. Further studies including large population and associated factors are needed in this age group.
This study had some limitations. The data was obtained retrospectively from the patients who were clinically suspected with urinary tract infection and performed DMSA scan. However, for minimizing the factors that affect this study, we excluded the patients with a fever, a positive urine culture result, acute pyelonephritis and with genitourinary anomalies. A prospective study will be necessary in normal Korean children.
In addition, we did not consider relevant variables such as height, weight, nutritional status and genetic factors3,16,30). Following studies would be required considering these relevant variables.
In conclusion, we established the simple age-based equation predicting renal length by DMSA scan in children over 1 year of age. It is suggested that this formula would be a useful tool to estimate adequate renal size and growth in Korean children in clinical practice.
 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


