

Introduction
Necrotizing enterocolitis (NEC) is an emergency gastrointestinal disease in neonates due to mucosal or transmural necrosis of the bowel. About 7% to 13% of all very low birth weight (VLBW) infants admitted to the neonatal intensive care unit (NICU) develop NEC, with a mortality range of 10% to 44%1-3), and both the incidence and mortality rate increase with decreasing birth weight and gestational age (GA). Intestine immaturity, birth asphyxia, low appearance, pulse, grimace, activity, and respiration (Apgar) score, intestinal ischemic change due to umbilical artery catheterization, viruses (rotavirus, coronavirus, and enterovirus), infection from coagulase-negative Staphylococcus or Clostridium difficile, and early rapid feeding are cause of NEC4-6). Some reports have indicated an association between red blood cell (RBC) transfusion (RBC(t)) and NEC, but this is controversial7-10). In this study, we analyzed the association between NEC and RBC(t) in VLBW preterm infants.
Materials and methods
We reviewed the charts of 180 VLBW preterm infant patients retrospectively who were admitted to the NICU of CHA Gangnam Hospital from January 2006 to December of 2009, excluding patients with hematologic disease, intraabdominal anomalies, and other congenital anomalies. Patients who received transfusions for causes other than NEC were also excluded.
The NEC diagnosis was made according to the modified Bell's staging criteria by a neonatologist when infants had both systemic and radiographic signs of NEC. Infants with stage II or greater were defined as the NEC group and those less than stage II and without NEC patients were defined as the control group. We defined that RBC(t) before NEC diagnosis as the frequency of transfusion until the NEC diagnosis (mean day at NEC diagnosis, day 18) in NEC group. Therefore, the frequency of transfusion was counted until 18 days after birth in control group. We evaluated patient history, including GA, birth weight (B.wt), Apgar score at 1 and 5 minutes, hemoglobin (Hgb) and hematocrit (Hct) at birth, the time from premature rupture of membrane (PROM), the use of prenatal antibiotics, intraventicular hemorrhage (IVHŌēźgrade 2: identified and classified by sonographic features), disseminated intravascular coagulopathy (DIC), hemorrhage history at other sites (pulmonary hemorrhage, gastrointestinal hemorrhage, and petechia), the presence of respiratory distress syndrome (RDS), and the number of times surfactant was used, presence of patent ductus arteriosus (PDA), dose of indomethacin administration, time on ventilator and O2 and the presence of bronchopulmonary dysplasia. We investigated the NEC stage and the frequency of packed RBC(t) during the hospital course and transfusions before the NEC diagnosis for the patients with a NEC diagnosis. The decision for RBC(t) was made by the neonatologist caring for the infant and transfusion guidelines11) were followed. All transfusions were done with packed RBCs. Packed RBCs were transfused in a volume of 10 to 20 mL/kg over 2 to 4 hours.
PDA was diagnosed based on echocardiographic findings. The number of transfused patients, the frequency of transfusions per patient, Hgb level at the time of transfusion, and cases in which the NEC diagnosis was made within 48 hours of transfusion were also analyzed. The Statistical analysis was performed with SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA) using the t-test, and logistic regression. P value under 0.05 was considered significant.
Results
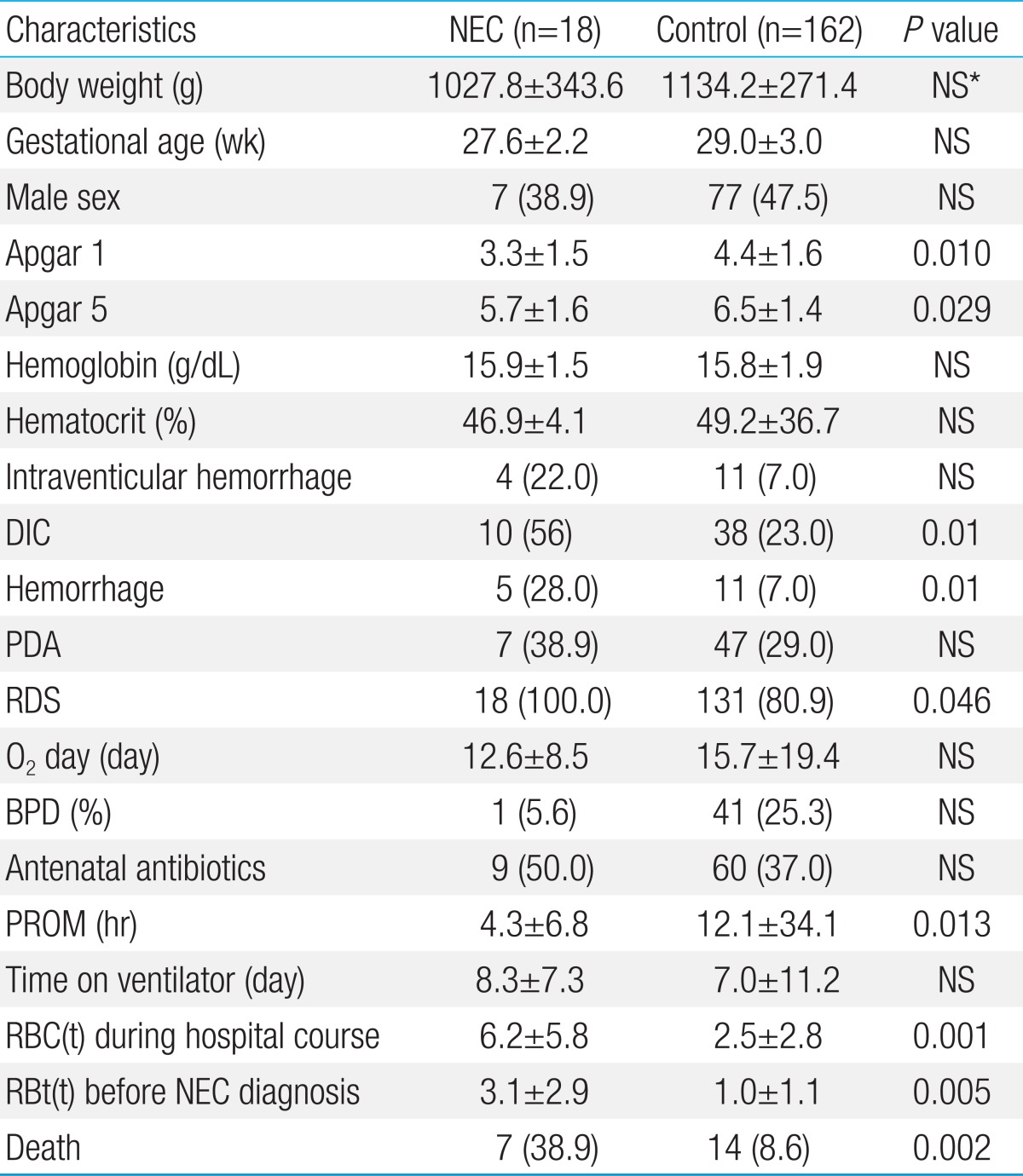
Among the 180 VLBW preterm infants, 18 (10%) were included in the NEC group. GA, B.wt, Hgb and Hct were not different between the two groups at birth. But, the Apgar scores at 1 and at 5 minutes were significantly lower in the NEC group, and the incidence of RDS, DIC, hemorrhage and mortality were also significantly higher than those in control group. The incidence of IVH and PDA tended to be more frequent in the NEC group than that in the control group. But there were no significant statistical difference. A total of 3.1┬▒2.9 transfusions were administered in the NEC group before the NEC diagnosis with 6.2┬▒5.8 transfusions administered in the NEC group during the entire hospital course. This number of transfusions before NEC diagnosis was significantly larger than that in the control group (1.0┬▒1.1 times) (Table 1).
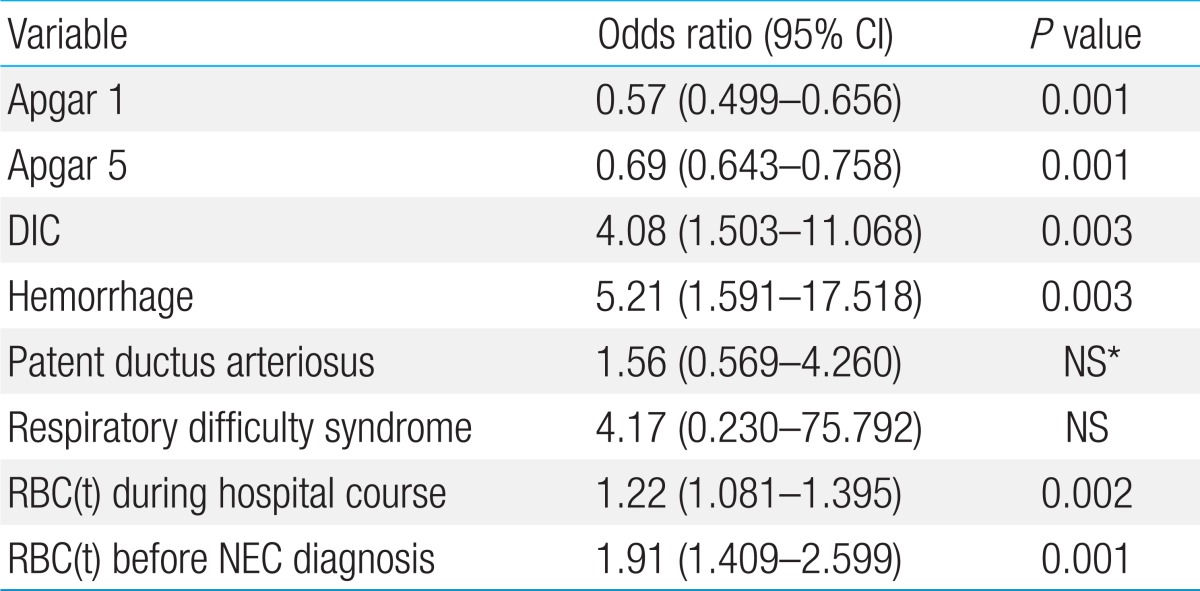
Table 2 shows the univariate logistic regression to verify generally known NEC risk factors, including Apgar score, PDA, RDS, DIC, and hemorrhage. PDA was not a significant factor and RDS had a nonsignificant confidence interval. The risk of NEC decreased significantly with higher 1 and 5 minutes Apgar scores (Table 2). The risk for NEC increased 1.22 times (95% confidence interval [CI], 1.081 to 1.395; P=0.002) for those with a higher frequency of RBC transfusion during hospital course. The risk for NEC increased 1.91 times (95% CI, 1.409 to 2.599, P=0.001) with higher the frequency of RBC(t) before NEC diagnosis (Table 2). We conducted a multivariate logistic regression after adjusting for GA, Apgar score, PDA, RDS, PROM, DIC and death. As a result, the risk for NEC increased 1.19 times (95% CI, 1.022 to 1.387; P=0.026) with increasing frequency of RBC(t) during the hospital course. The frequency of RBC(t) before NEC diagnosis increased the risk for NEC 1.63 times (95% CI, 1.145 to 2.305; P=0.007) (Table 3).
Discussion
Late complications of the gastrointestinal system in preterm babies are increasing along with early pulmonary and cardiologic early complications. NEC remains a disease with high mortality even with aggressive treatment12). Additionally, NEC requiring surgical treatment lead to growth and developmental disorders in VLBW infants13,14). The incidence of NEC varies with reporters. According to Walsh and Kliegman15), Gregory et al.16), Egan et al.17), and Polin et al.18), NEC occurs in 0.83% to 7.5% of all infants, but according to Kliegman et al.19) the incidence of VLBW infants admitted to the NICU is 12%. In this study, the incidence of NEC among the VLBW preterm infants was 10%, which was similar to other reports.
The etiology and pathogenesis of NEC is not clearly understood20), but it is known to be a complex, multifactorial disease21,22). According to a recent reports transfusion increase the risk for NEC7), and the NEC mechanism is related to a recent exposure to transfusions. The latest hypotheses as to why packed RBC(t) increases the risk of NEC suggest that stored RBCs decrease nitric oxide23) and a packed RBC(t) increases the intestinal immune response24). In this study, GA and B.wt were not different between the NEC and control groups, but in the univariate logistic regression, the risk for NEC decreased significantly the higher the GA, B.wt, and Apgar scores at 1 and 5 minutes. Higher PDA incidences also tended to increase NEC risk, but the difference was not significant. The number of patients in the NEC group who were diagnosed within 48 hours of a transfusion was 14 and after 48 hours the number was two. Only two patients with NEC did not receive a transfusion their GA were 31 and 30 weeks and their Apgar scores at 1 minute were 1 point and 0 points. Cardiopulmonary resuscitation was carried out on these infants. The Apgar score at 5 minutes recovered to 5 points for both and the infants recovered with conservative therapy after the NEC diagnosis.
In the multivariate logistic regression, a higher frequency of RBC(t) before the NEC diagnosis increased the risk for NEC 1.63 times (95% CI, 1.145 to 2.305; P=0.007) after adjusted for GA, Apgar score at 1 minute, RDS, PROM, DIC, and death. The number of transfusions was significantly different between our two groups and the adjusted multivariate logistic regression revealed that the NEC risk increased 1.297 times (95% CI, 1.097 to 1.533; P=0.002) with an increase in the number of transfusions. There are several biologically plausible reasons why packed RBC(t) may lead to NEC, including a decrease in nitric oxide in stored RBCs and an exaggerated intestinal immune response to packed RBC(t)9). In contrast to our study, Josephson et al10). reported that RBC(t) had no temporal relationship to NEC and stated that is only meaningful as it indicates the infant's general condition.
Because many reports are contradictory on the relationship between transfusions and NEC, additional studies are necessary involving larger patient groups. In addition, the patient's general condition and the risk of NEC based on the transfusion must be considered when treating preterm infants <1,500 g.
In conclusion, we analyzed the risk factors for developing of NEC in VLBW preterm infants. The results showed that the risk for NEC increased with an increased frequency of transfusions before the NEC diagnosis (relative risk, 1.63; 95% CI, 1.145 to 2.305; P=0.007).

 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


