

Introduction
Wiskott-Aldrich syndrome (WAS) is an X-linked recessive syndrome characterized by thrombocytopenia with small defective platelets, atopic dermatitis, recurrent infections with immunodeficiency, and early death of the affected males1,2). Numerous studies have revealed a strong association between genotype and phenotype for the WAS gene3). The various mutations in the WAS gene lead to the presentation of 3 distinct clinical phenotypes: the classic WAS; the milder X-linked thrombocytopenia (XLT) variant; and congenital X-linked neutropenia (XLN)2,4). Whether the clinical phenotype of WAS or XLT is severe or mild is strongly influenced by the effect of the mutation on protein expression1,4,5). Thus, genotype-phenotype correlation in WAS/XLT is not absolute2,4). Only one-third of WAS patients represent the triad, recurrent infection, eczema, and thrombocytopenia particularly during infancy1). In the present case, we report a patient with WAS caused by a novel deletion mutation presenting as familial XLT, for which the clinical course of disease was mild in infant and toddler period, but rapidly worsened afterward.
Case report
A 4-year-old boy had frequently visited the outpatient clinic for the past year with refractory thrombocytopenia since birth and recurrent herpes simplex infections. He had been treated with intravenous immunoglobulin and steroid since birth; however, refractory thrombocytopenia had persisted. Bone marrow aspiration and biopsy showed slightly increased megakaryocyte counts without the presence of any abnormal cells. The atopic skin manifestations did not appear until 3 years of age. Regarding family history, his older brother who was diagnosed as chronic thrombocytopenia died due to intracranial hemorrhage at the age of 10 years, but his 14-year-old sister was healthy.
Until the age of 4, complete blood count showed only thrombocytopenia, hemoglobin (Hb) 11.9 g/dL, white blood cells (WBC) 6,900/┬ĄL with 65.0% segment neutrophils, and platelets 7,000/┬ĄL. After developing recurrent infection and eczema, his laboratory findings revealed neutropenia state such as Hb 8.8 g/dL, WBC 1,690/┬ĄL with 27.0% segment neutrophils, platelets 2,000/┬ĄL, and reticulocyte count 3.13%. Serum immunoglobulin levels were within normal ranges for immunoglobulin IgG, IgA, and IgM although the level of IgE was slightly increased. Lymphocyte subset analysis showed CD4+ at 21.1% and CD8+ at 44.4%, with a CD4+/CD8+ ratio of 2.1. Blood chemistry data was within normal ranges. Single donor platelet and pure red cell transfusion were performed with methylpredisolone pulse therapy for 3 days. However, the platelet counts did not recover. Based on the findings of recurrent infection, refractory thrombocytopenia, and a family history of an elder brother with chronic thrombocytopenia, we decided to perform genetic analysis for WAS after informed consent was obtained. After diagnosis, we evaluated human leukocyte antigen (HLA) typing within the family for hematopoietic stem cell transplantation and performed genetic analysis of the family with genetic counseling. The results showed that his sister was not matched, and we therefore searched for an unrelated HLA-matched donor. While awaiting the HLA-matched donor, his condition rapidly deteriorated with dehydration, petechia, and recurrent epistaxis.
One month later, he was readmitted with fever, subconjuntival hemorrhage, oral mucosal hemorrhage, a pale appearance, and >10 episodes of dark brown-colored vomiting. On the next day, he showed decreased mental status. Because of a strong suspicion of intracranial hemorrhage, emergency brain CT was performed. The CT findings revealed an intracranial hemorrhage in the left frontal lobe and a small intraventricular hemorrhage in the caudate nucleus. Despite aggressive medical and surgical intervention to control the intracranial hemorrhage, he died after three days.
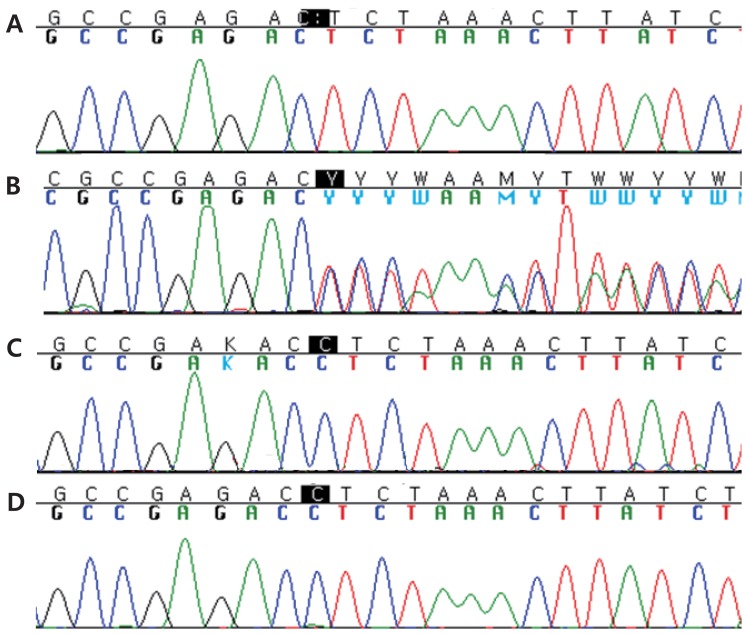
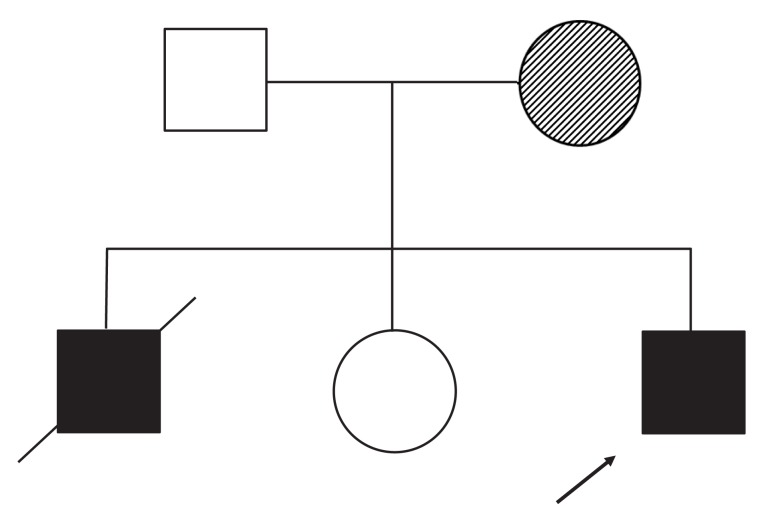
The results of genetic sequence analysis revealed a novel pathogenic deletion mutation in exon 9 of the WAS gene: c.858delC (p.ser287Leufs*21) (Fig. 1). This novel pathogenic variant causes the early termination of protein translation. This mutation in the WAS gene was identified in his mother later while neither his father nor sister. This result suggested that his brother, who earlier died from chronic thrombocytopenia, also had an inherited WAS (Fig. 2).
Discussion
The WAS gene encodes a 502-amino acid protein expressed exclusively in the cytoplasm of hematopoietic cells. It possesses 5 distinct domains: an N-terminal WAS protein (WASp)-homology domain 1, a guanosinetriphosphatase binding domain, a proline-rich region with SH3 binding motifs, a verprolin and a cofilin homology domain, and a C-terminal acidic region that interferes with Arp2/3 complex-mediated actin polymerization1,2,4-6). WASp is a regulator of actin polymerization in hematopoietic cells and controls the assembly of actin filaments required for microvesicle formation downstream of protein kinase C and tyrosine kinase signaling1,6). WASp plays critical roles in signal transduction and in the regulation of cytoskeletal reorganization7). Approximately 300 different mutations in WASp have been reported thus far, most of which cluster in the first 4 exons and exons 7 and 101,8,9). The different mutations in WASp lead to the presentation of 3 distinct clinical phenotypes: the classic WAS triad of thrombocytopenia / small platelets, recurrent infections, and eczema; the milder XLT variant, characterized predominantly by thrombocytopenia/small platelets; and X-linked congenital neutropenia without the clinical findings characteristic of WAS/XLT intermittent thrombocytopenia1,4,6). Each phenotype is caused by different molecular mechanisms. First, the classic WAS completely averts WASp expression1,4,5). Second, the XLT phenotype is the product of missense mutations that result in expression of defective WASp2,4). Lastly, XLN is caused by gain-of-function mutations that produce constitutively activated WASp2,4). However, the most consistent phenotype-genotype correlation is observed by dividing the patients into 2 categories: WASp-positive (WASp+) if the mutated protein is expressed and of normal size, and WASp-negative (WASp-) if the protein is absent or truncated2,4,6).
The common mutations for XLT are missense mutations in exons 1 and 2 or splice site mutations1). In cohort studies reported in 2004 and 2010, the missense mutation was the most common type followed by splice site mutations and deletions, but only 1 case of a deletion mutation was found in exon 94,6). The type of mutation also showed a correlation with the expression of WASp; WASp+ was correlated more highly with missense and splice mutations, while WASp- was correlated more highly with deletion/insertion and nonsense mutations6). The deletion genotypes prevent the expression of WASp in most cases, due to a premature termination codon that causes the failure of protein translation6). The presence or absence of WASp according to WAS gene mutations had no influence on survival in patients with the XLT phenotype4). These patients showed a rare type of deletion mutation in XLT.
Because of the mild clinical characteristics of XLT, some adult XLT patients can be falsely diagnosed with chronic immune thrombocytopenia, which may result in loss of optimal treatment, such a s hematopoietic stem cell transplantation2,10). In this case, the patient's older brother was mis-diagnosed with chronic thrombocytopenia due to a mild clinical presentation, but later he died due to a life-threatening event of intracranial hemorrhage at the age of 10 years. In this case, the late clinical presentations of eczema and recurrent infection delayed the diagnosis of our patient. The boy only presented with refractory thrombocytopenia until 3 years old. His condition was also considered mild according to the scoring system11). Upon presenting with recurrent herpes simplex infection and controllable atopic dermatitis, his WAS score of 2 was still mild11). Classic WAS patients with a high score were reported to be aged <1 year old, while XLT patients with scores of Ōēż2 were reported as being over toddler period, the age between 1 to 3 years12).
Our novel pathogenic deletion mutation in XLT initially presented with mild clinical symptoms but eventually led to a rapid and severe course of the disease with a high risk of life-threatening intracranial bleeding. Initially, the patient presented only with neonatal refractory thrombocytopenia until 3 years of age, post-infected neutropenia, and late presentation of eczema, but his disease progressed rapidly with a a life-threatening event of intracranial hemorrhage. Due to the phenotypic variability, clinicians should consider the WAS in male patients who present an atypical bleeding tendency, bruising, congenital or early onset of thrombocytopenia13). Especially, XLT should not be assumed to follow a mild clinical progression because phenotypes and genotypes do not always correlate. The clinical features and severity of WAS patients are highly varied. Unfortunately, we did not perform the detection of WAS protein in this boy. For this novel mutation, a scoring system, genotype/phenotype correlation, and laboratory findings provided an ineffective prediction.
In conclusion, we report a Korean boy with XLT with a rapid and severe form of disease after toddler age due to a novel deletion mutation in the WAS gene.
 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


