




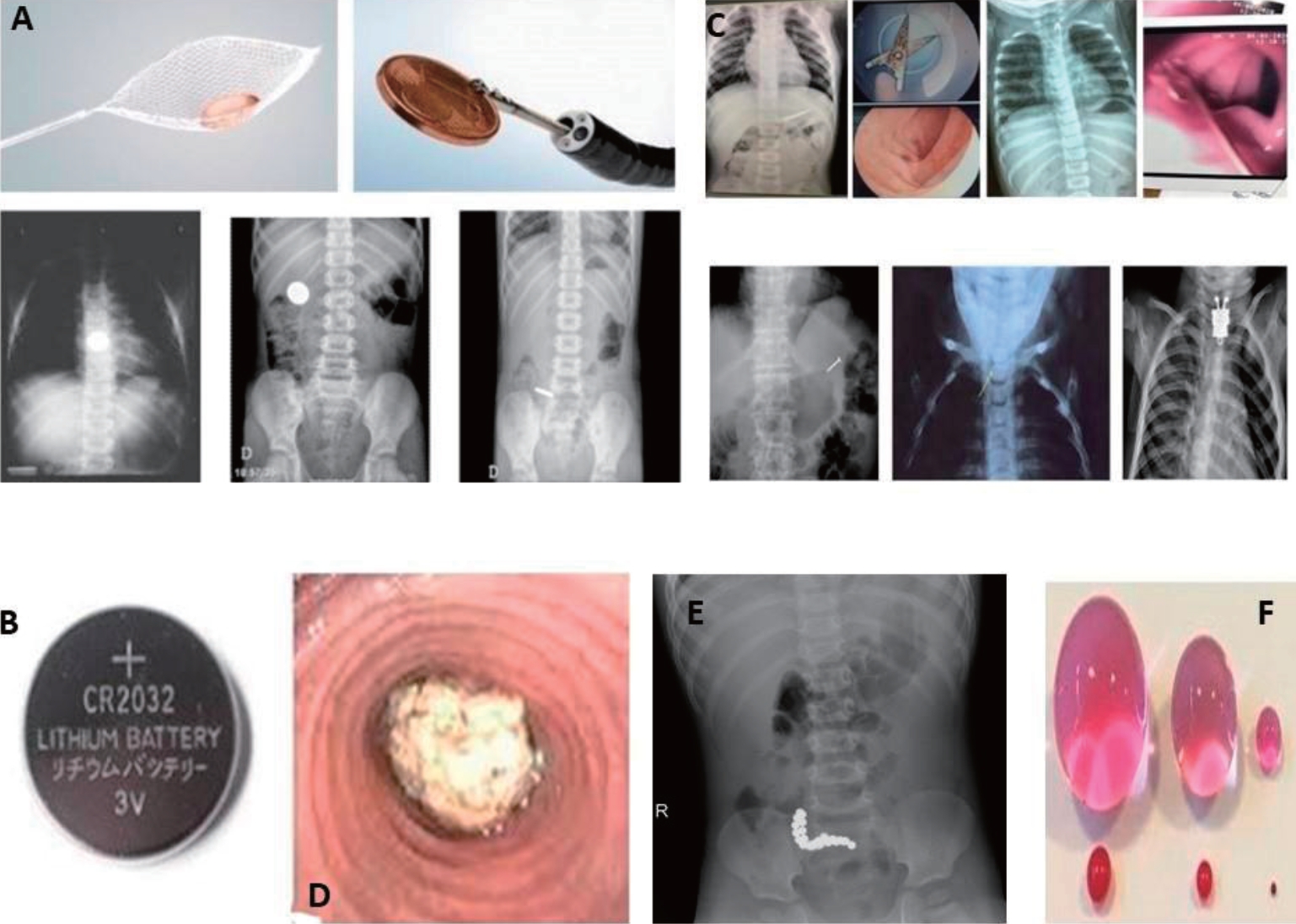
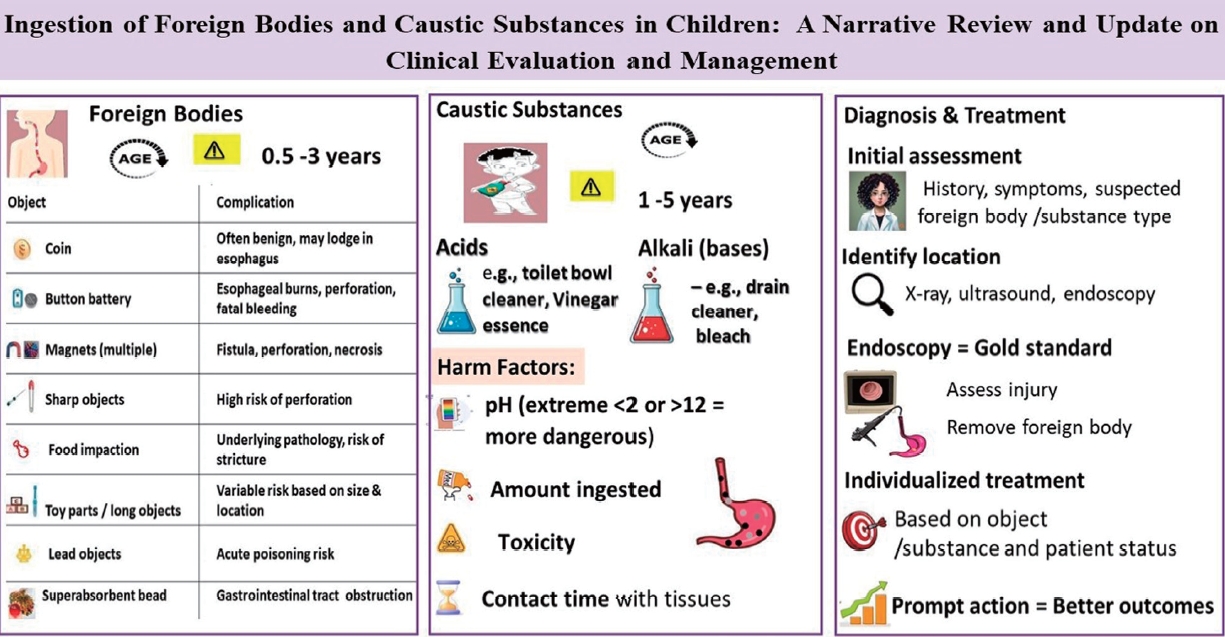
Graphical abstract
Introduction
The majority of cases of foreign body ingestions in children occur between the ages of 6 months and 3 years [1-3]. In most cases, the ingestion is reported by the child's caregivers or other family members as witnesses or suspects of the event. Its clinical management focuses on confirming and treating cases at risk of complications, depending on the foreign body's type and location. The ingestion of caustic substances is a frequent concern in emergency departments, occurs most often in children aged 1–3 years and can cause serious acute and long-term complications, such as the development of esophageal strictures [4,5].
Foreign body ingestion
1. Epidemiology
More than 100,000 cases of foreign body ingestion are reported annually in the United States (US) and of them, >75% occur during childhood [1,6,7]. Most foreign body ingestions occur between the ages of 6 months and 3 years [1-3]. Multiple body ingestions and repeated episodes are uncommon and mainly observed in children with neurodevelopmental and behavioral disorders [8,9]. Although the mortality rate from foreign body ingestion is extremely low, deaths have been reported [2,10]. Common foreign bodies swallowed by children include coins, button batteries, toys, toy parts, magnets, safety pins, screws, jewelry, bones, and food [2,7,11].
2) Flat batteries
The consumption of flat batteries (Fig. 1B) has recently increased because of their widespread use in household appliances and other devices. Serious complications (esophageal burns, perforation, and/or fistula development) and/or death occur in 3% of battery ingestion cases [2,3,13]. Although disc-shaped batteries have been used for almost 30 years, their initial clinical experience with ingestion quite benign. Data collected and published by the National Capital Poison Centre in 1992 on >2,300 patients showed that over a 7-year period no deaths occurred and only 0.1% of affected individuals developed a serious complication consisting of 2 esophageal strictures [14]. However, over the next 20 years, clinical experience has changed dramatically with a new follow-up study from the same center. In this study of >8,600 cases, major complications occurred in 73 patients (0.8%), versus death in 13 patients (0.15%) [15]. The cause of this dramatic increase in morbidity and mortality appears to be linked to 2 specific changes in the market during this period: increased battery diameter and the change to lithium cells which cause an increased likelihood of esophageal impaction and increased pressure respectively. Lithium batteries >20 mm are responsible for 94% of battery ingestion-related deaths. The tissue damage is caused by the generation of hydroxide radicals; therefore, caustic mucosal damage is induced by from a high pH rather than electrothermal injury. Changes including, an increase in pH from 7 to 13 at the negative pole in 30 minutes and mucosal necrosis in 15 minutes [16] were observed in animal experiments.
These findings are compatible with reports of esophageal strictures at 2 hours after ingestion and highlighting the importance of immediate endoscopic interventions in these children.
3) Sharp objects
Sharp objects (Fig. 1C) constitute 10%–15% of the foreign bodies swallowed by children [7]. The most common sharp objects are safety pins, needles, paper clips, pins, and fish bones. Sharp objects carry a high risk of perforation of approximately ~15%–35% [1,17]. If such objects lodged within the hypopharynx, they can cause a retropharyngeal abscess [18]. Toothpicks and bones also frequently cause perforations [7,19].
4) Impacted food
Impacted food (Fig. 1D) is the most common foreign body in the esophagus of adults but not in children. Children with bolus impaction usually have underlying esophageal pathologies such as: eosinophilic esophagitis, esophagitis caused by reflux, strictures, achalasia, diaphragm or ring, or esophageal motility disorders [7,20,21]. Therefore, biopsy is recommended, during endoscopy for bolus removal, biopsies in these also recommended [7].
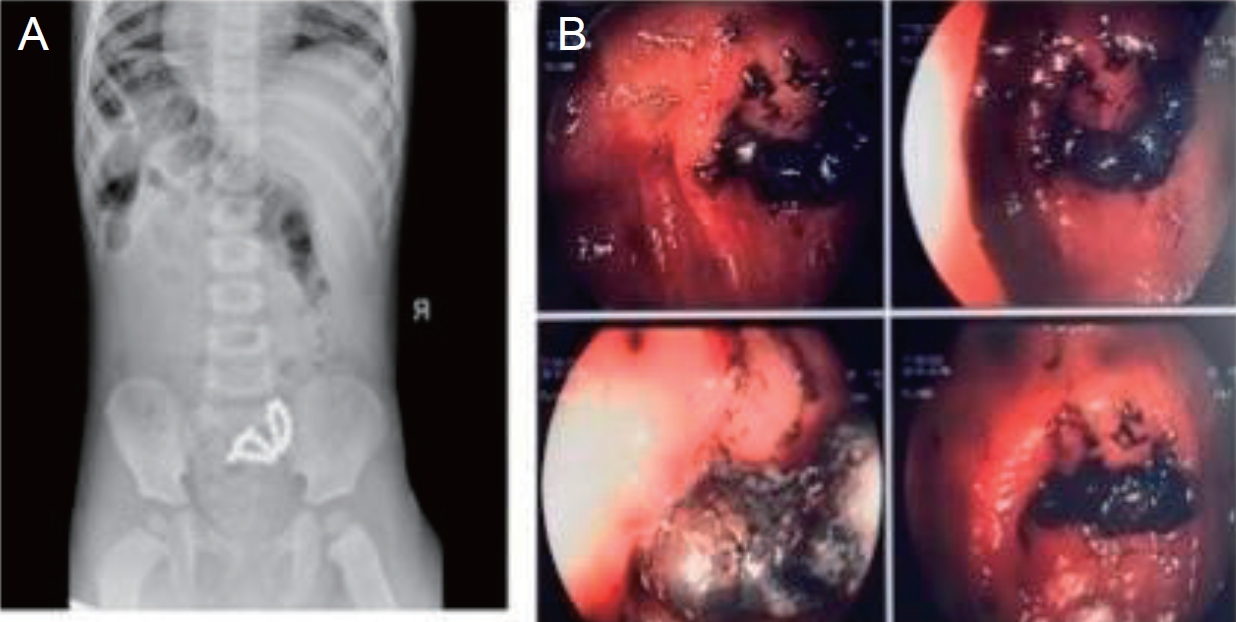
5) Magnets (Figs. 1E and 2)
In recent years, use of magnets has increased in toys consisting of small hundreds of balls, cylinders or cubes, “stress relievers” and household utensils, resulting in serious consequences from swallowing them [22,23]. These magnets are high-powered, are made of neodymium and exert 5 times the pulling force of traditional magnets. This risk arises because the as the mucous membrane can become trapped between the magnets or between the magnet and another metal body, causing perforation and fistula.
6) Objects/toys comprising of many parts
Objects/toys comprising of many parts require special attention because they may include radio-opaque or nonradioactive parts or even batteries with known risks, such as the fidget spinner toy [24].
7) Long objects
Long objects such as toothbrushes, batteries, and spoons are more commonly swallowed by older children, adolescents, and adults. The risk of serious complications depends on the object's length or other characteristics as well as the child's age [25].
8) Objects with a high lead content
Objects with a high lead content (e.g., lead weights used in fishing, curtain weights, toys, medals) can cause acute lead poisoning, or even death [26].
2. Clinical manifestations and symptoms
Children are often asymptomatic after foreign body ingestion, in which case the investigations are performed because of a positive or suspected history. In a study of 325 pediatric patients, only 50% with a foreign body in the esophagus reported symptoms, such as retrosternal pain, dysphagia, and cyanosis at the time of swallowing, in many of these children, these symptoms were transient [18]. When symptoms are present, the clinical presentation varies according to foreign body and location.
When a foreign body is present in the esophagus, a child may experience food intake refusal, dysphagia, drooling, chest pain, restlessness or respiratory symptoms such as wheezing, hoarseness and fever. Sharp foreign bodies, may cause symptoms such as subcutaneous emphysema or even pneumomediastinum due to esophageal perforation [2,12]. In cases in which the foreign body has been lodged within the esophagus for an extended long time, weight loss, recurrent aspiration pneumonia, or tracheoesophageal fistula development may occur. Aortic erosion and life-threatening bleeding after the ingestion of foreign bodies have also been described [20].
Patients with a foreign body in the stomach are usually asymptomatic, unless that foreign body is large and capable of causing an obstruction, which would result in vomiting or even a refusal to eat [27]. Patients with a gastric outlet obstruction may present with emesis containing undigested gastric contents as well as, non-bilious, gastric distension. Depending on the type of foreign body (e.g., sharps, batteries, magnets), its removal is considered advisable even in asymptomatic patients to avoid further complications.
Foreign bodies that pass through the pylorus and progress into the intestine usually do not cause symptoms and are expelled during defecation. In some cases, they can become trapped in the lower digestive tract, causeinge delayed complications. Cases of coin entrapment in the cecum with symptoms compatible with appendicitis, pyogenic liver abscess after the displacement of a sharp object from the digestive tract, chronic appendicitis after the insertion of a long object, and ileal perforation after swallowing a stone have been described.
3. Assessment
A detailed history and meticulous physical examination are crucial in the case of a suspected foreign body and ensure an appropriate investigation. Increased clinical suspicion is also very important when the corresponding symptomatology is present, even with a negative history in patients within high-risk age groups (children up to 3–5 years of age), for whom foreign body ingestion should be included in the differential diagnosis.
Conventional anteroposterior and lateral radiographs of the neck, chest, and abdomen can be used to establish at diagnosis and provide information regarding foreign body type and location [2,15]. A metal detector can reveal materials that are metals but not radiopaque, for example. aluminum; however, it has limited diagnostic value as it does not detect all metallic bodies [28] and cannot specify its type (e.g., battery versus/coin, or exact location.
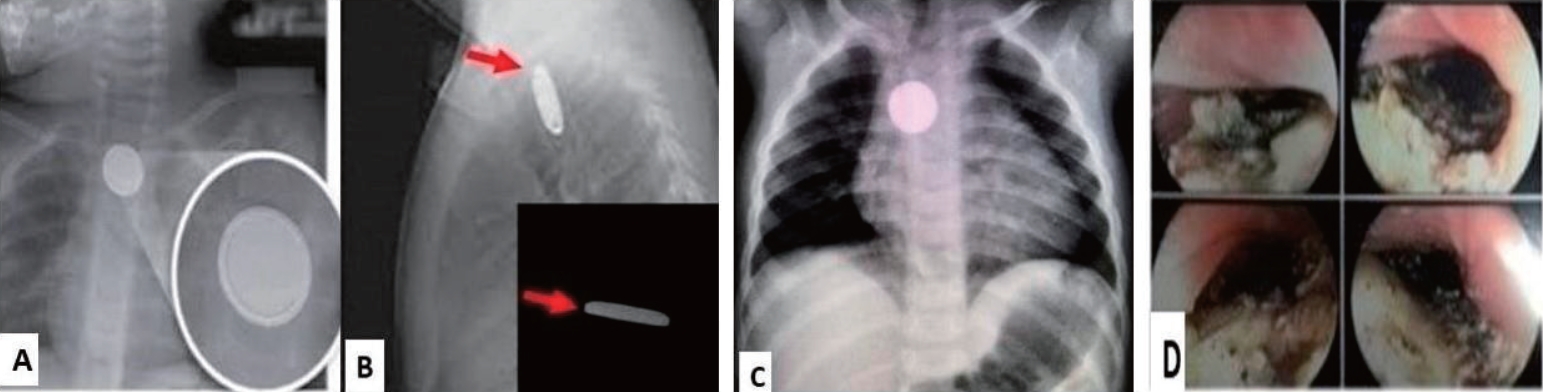
When the presence of a foreign body is revealed on radiography, the following should be evaluated. First, the location of the foreign body should be determined to inform its appropriate management. Foreign bodies located within the esophagus should be differentiated according to tracheal or esophageal placement. Flat foreign bodies located in the trachea tend to assume a sagittal position and are best observed on lateral radiographs, whereas those located in the esophagus are usually oriented coronally and appear circular on anteroposterior radiographs [29].
Equally important is the distinction between circular foreign bodies in the esophagus, as batteries require immediate removal, whereas coins may not. For batteries, the double-halo or step-off sign Fig. 3 is characteristic. If simple radiographs cannot identify the foreign body, further investigation using computed tomography (CT) or noncontrast-enhanced magnetic resonance imaging (MRI) may be required especially if the patient is symptomatic or the foreign body has some dangerous characangiograteristics such as being sharp, long >5 cm. or large, (diameter >2 cm). If the patient is asymptomatic, the environment is reliable and safe for the ingested foreign body, and the object has benign characteristics, further imaging may not be necessary. The use of ultrasound to highlight a foreign body in the esophagus or stomach requires appropriate special operator experience [30]. Upper gastrointestinal transit with water-soluble contrast has been used to highlight mainly nonradioactive foreign bodies, whereas barium transit should be avoided since it may complicate localization of the foreign body during any upcoming gastroscopy.
4. Patient management after foreign body ingestion
Patient management in such cases varies depending on the patient’s clinical picture, age, as well as the, foreign body's location, properties, size, length, sharpness. Foreign body type dictates the specific instructions for the timing of its removal.
5. Coins
A small percentage of swallowed coins are found in the esophagus, whereas approximately two-thirds of them are found in the stomach during initial radiography. If in the esophagus, they should be removed immediately if the patient is symptomatic or within 24 h if the patient is asymptomatic. Typically, in 20%– 30% of cases, the coin advances into the stomach during follow-up; this, this occurs more often in older children and when initially located in the lower third of the esophagus [31].
When coins are found in the stomach, treatment can be conservative because they have smooth borders, are not made of toxic metals, and in the majority of cases, they are expelled naturally without complications within 1–2 weeks. If the coin remains in the stomach for >4 weeks, its surgical removal is recommended [1,7,15]. If the patient presents with symptoms, such as vomiting, fever, and abdominal pain, the coin's condition and location are reassessed and endoscopic removal is performed.
6. Batteries
A battery in the esophagus is a medical emergency that should be treated immediately. Esophageal necrosis can be caused by battery liquefaction through an electrical current, resulting in ulceration within a few hours and perforation of the esophagus up to 8 h after ingestion [24]. Therefore, if a battery is lodged in the esophagus, immediate removal within 2 hours is recommended. If immediate access to an endoscopic room is lacking, it is recommended that children >1 year of age, who are not allergic, be administered a single dose (of 5–10 mL) of honey by the parents as soon as possible after the battery is swallowed (especially if the child is being transported from the countryside), followed by a single dose of sucralfate 500 mg once the hospital is reached. Animal studies have shown that honey has a protective effect against the appearance of burn damage [32]. Patients with a battery embedded in the esophagus requires hospitalization, immediate endoscopic removal, and special imaging when deemed necessary to detect possible complications, such as esophageal perforation, tracheoesophageal fistula, and aortic erosion [15]. In cases of severe esophageal burns, must be re-evaluated for esophageal strictures. The usual practice is to perform a barium swallow at 4–6 weeks after battery ingestion.
According to recent ESPGHAN guideline the protocol for treating battery ingestion in children [33] when the battery is postesophageal, the distinction is made according to the time that has passed since the battery was swallowed. If it is <12 hours have passed and the child is symptomatic or swallowed a magnet, immediate endoscopy within 2 hours is recommended. If the battery passed through the stomach, then a pediatric surgery consult is recommended. If the child is asymptomatic, then radiograph should be repeated at in 7–14 (earlier if symptoms occur). Management is individualized for each case and center. If >12 hours have passed since the episode, endoscopy is recommended to remove the battery and to assess possible damage to the esophageal mucosa. If transmural esophageal damage is suspected, CT angiography is recommended to exclude the possibility of vascular damage.
If a battery is detected in the stomach, it is removed. If it has progressed to the intestine and the child is symptomatic then, pediatric surgical treatment is recommended; however, if the child is asymptomatic, continued radiographic monitoring for 7–14 days is recommended.
7. Food impaction
Food impaction in the esophagus (Fig. 1D) is rare in children and usually conceals esophageal pathologies. Food removal is performed immediately when children cannot manage their secretions; if the patient feels comfortable and manages their secretions removal can be extended to <24 hours [7], and treatment is individualized depending on food type and impaction location [21]. However, the use of proteolytic enzymes, such as, papain or glucagon, is not recommended for the management of food impaction in children.
8. Magnets
Magnet swallowing (Fig. 2) is a serious and sometimes life-threatening problem requiring that requires special management. Swallowing one or more high-powered magnets, especially if swallowed at different times, can trap the mucosa, through an attractive force between them, resulting in pressure, necrosis, perforation, inflammation, obstruction and further complications such as bowel resection. Magnet ingestion requires immediate evaluation using, cervical, thoracic, abdominal, and lateral radiographs. Mucosal entrapment cannot always be assessed using radiography; however, the consistent presence of slightly separated magnets is indicative of this issue. Even when a single high-power magnet is swallowed, there is a risk of mucosal entrapment may occur due to internal or external contact with another metal object on the individual's clothing, jewelry, or belts. Repeated radiographs are then used to determine whether are multiple magnets which may mistakenly suggest that they are one (fused together). Thus, immediate removal from the esophagus, stomach, or proximal duodenum is recommended if multiple magnets or other metallic objects have been swallowed. I case the magnets have advanced into the intestine, asymptomatic patients should undergo close clinical monitoring and radiographs every 4–6 hours. Alternatively, an attempt should be made to remove them using enteroscopy or colonoscopy if feasible. If patients are symptomatic, immediate surgical resection is recommended.
9. Long objects
The removal of long and blunt objects, such as toothbrushes, batteries, and spoons, should be individualized depending on their length and width as well as child's age. Objects >6 cm usually cannot pass through the stomach [13], and their removal is recommended. However, close monitoring and surgical treatment are required if these objects enter the intestine. In children aged <5 years, removal from the stomach is recommended if the objects are >2.5 cm long.
10. Superabsorbent polymers
Superabsorbent objects (Fig. 1F) have the ability to increase their volume by 30–60 times upon contact with liquids. These objects are not radiopaque and radiographs do not help locate them in the digestive tract. The administration of a water-soluble contrast agent may highlight their location and size. Their immediate removal is recommended due to the increased risk of obstruction, if endoscopic removal is not possible or the patient's symptoms warrant surgical treatment.
11. Lead-containing objects
Acute lead poisoning can occur in children who swallowed lead-containing objects. Elevated levels of lead were found even 90 minutes after ingestion as the acidic environment of the stomach favors the dissolution of the metal. Thus, the immediate removal of these objects from the esophagus or stomach is recommended.
The indications for immediate removal of the foreign bodies are shown in Table 1
12. Foreign body removal techniques
Different methods can be used to remove foreign bodies depending on object size and location; However, in some cases, they are expelled naturally. A rigid endoscope is typically used for foreign bodies located proximal to the upper esophageal sphincter. Magill forceps can also be used to retrieve foreign bodies located in the oropharynx and proximal to the upper esophageal sphincter that are visible during the intubation phase.
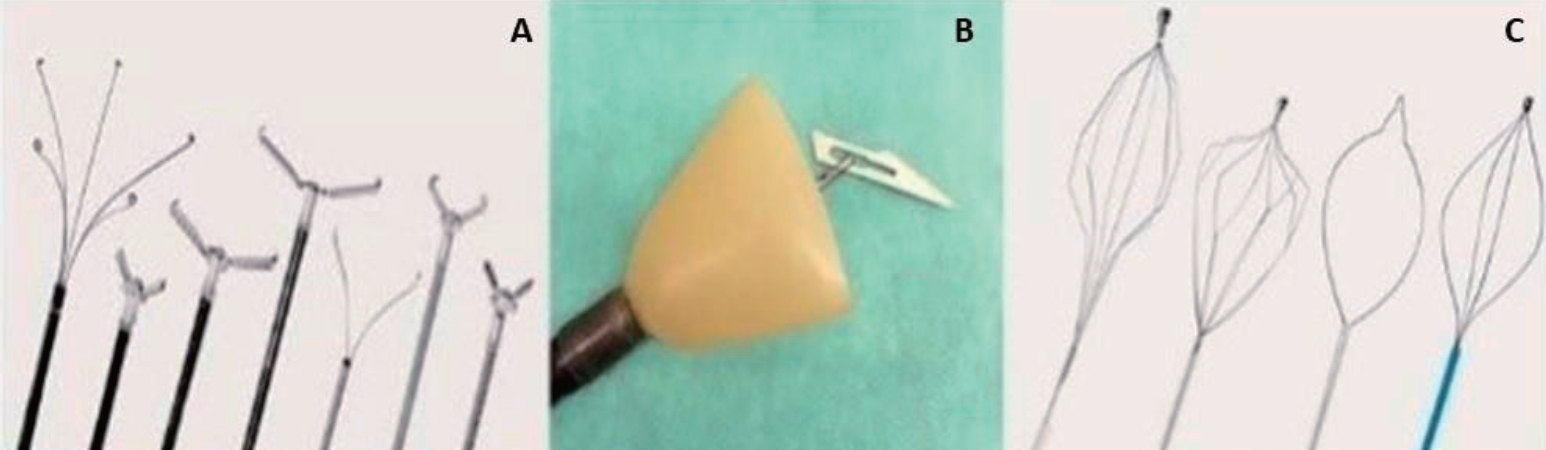
Flexible endoscopes preferred in most cases because they can be used to diagnose complications. Depending on the object's type and location, special grasping forceps, loops, and foreign body grasping nets [1,2,8] can also be used (Fig. 4). Older techniques using Foley catheter and forceps through a nasogastric catheter under radiological guidance have been abandoned. In rare cases, surgical intervention may be required to remove foreign bodies (such as magnets) and treat complications.
13. Complications
Foreign body ingestion by children can be a life-threatening situation thus treatment should be individualized depending on the object's location, type and size to prevent complications.
A detailed algorithm for the management of foreign body ingestion in children is presented in Table 2
Ingestion of caustic substances
The accidental ingestion of caustic substances continues to be a problem that requiring immediate treatment and intervention.
1. Epidemiology
Data from the US indicate 2.1 million cases, half of which were in children aged <5 years [34]. The most common substances ingested by children include household items, cosmetics and personal care products. The ingestion of caustic substances is most common in children aged 1–3 years, with 50%–62% of cases occurring in boys [5]. In children, it usually occurs accidentally; while in adults and adolescents it may occur as a suicide attempt.
2. Types of caustic substances
A substance is classified as caustic when it is capable of causing burns or mucosal erosion owing to its strong acidic or basic properties. Commonly ingested caustic substances include household cleaning products such as bleach, oven cleaners, and drain and toilet cleaners which contain sodium and potassium hydroxide [4]. Other common cleaning products such as laundry and dishwasher detergents, contain sodium phosphate, sodium carbonate, and ammonia [35]. Caustic substances are also components of cosmetic products such as hair care products, and swimming pool products. Alkaline substances are ingested more commonly than acids.
3. Pathophysiology
Alkaline and acidic, substances which are caustic, can cause similar mucosal damage similar to that, caused, however, by different mechanisms.
Alkaline substances tend to cause mucosal damage a pH >11.5–12.5 by creating necrosis through liquefaction. This type of necrosis leads to rapid mucosal degradation, allowing deeper penetration and even perforation. Penetration of the esophageal mucosa by an alkaline substance depends on its concentration and contact duration [36].
Corrosive (acidic) substances tend to damage the esophageal mucosa at a pH <2, thereby causing necrosis through thrombosis. Compared to alkaline substances, acidic substances are less likely to cause perforation because clots forming on the mucosal surface prevent further mucosal erosion. However, 6%–20% of acid ingestions cause esophageal burns [4,5,36].
In the first week post ingestion, in addition to the initial damage, delayed damage to the esophagus (either from alkalis or acids) can occur owing to further inflammation and vascular thrombosis. In the next phase, after 10 days, granulation tissue is formed and the esophageal wall thins. During this period, the esophagus is vulnerable to perforation. Esophageal burns are the most serious injuries as they are accompanied by chronic complications and present in 18%–46% of cases of the ingestion of caustic substances among children [37]. After 3 weeks, fibrous tissue formation begins and stenosis may develop in the esophagus, while perforation is less likely. No clear picture of the incidence and severity of gastric damage in such cases is available; however, in a study of 156 children with caustic substance ingestion, 11% suffered esophageal and gastric damage whereas 9% had gastric damage only [38]. In 80% of patients with alkaline ingestion, gastric injury was observed when a large volume (of 200–300 mL) was ingested. Large volume ingestion has been associated with gastric perforation, while bleeding and death from bronchial vein corrosion have been reported [39]. Gastric damage appears to be more severe with the ingestion of acids such as sulfuric acid, which can cause severe propyloride burns and lead to pyloric obstruction [39]. In a review of 98 patients who ingested acid, 8.2% developed gastric obstruction by 27 days, post ingestion and required a gastrojejunal catheter [40].
4. Clinical manifestations
Postingestion symptoms vary depending on the degree of damage to the digestive tract. The most common symptoms may last for several weeks and include dysphagia, esophageal motility disorders, and prolonged emptying time. Other symptoms include drooling, retrosternal or abdominal pain, or hematemesis.
5. Assessment
It is important to clarify the timing of the ingestion of caustic substance, as well as its exact chemical composition, pH, and possible volume ingested. Physical examination should include assessment of the central nervous system, vital signs, pupillary reflexes, and level of consciousness. The symptoms of salivation and refusal to eat suggest an esophageal injury. Lesions to the lips or mouth and pharynx have low predictive value for the presence or absence of esophageal injury. Other parameters requiring consideration include the possible toxic effects of these substances, possibility of intentional ingestion-suicide attempts, and simultaneous intake of multiple substances.
6. Imaging
Includes chest and abdominal radiographs are used to assess respiratory function, complications such as gastric or esophageal perforation, and the presence of pneumomediastinum or subcutaneous emphysema. The administration of contrast agents is not recommended; however, if perforation and or emphysema occurs possible erosion of vascular branches are suspected, CT or MRI should be performed.
7. Management
Patient stabilization and close monitoring are initially recommended, with an emphasis on avoiding vomiting and possible aspiration.
The provocation of vomiting, or administration of milk, water or other neutralizing agents, such as, activated charcoal is not recommended. Patients without signs or symptoms should be monitored for food avoidance and fluid intake [5]. The monitoring period is very important for the further management of the patients. An endoscopic examination is recommended for all symptomatic patients, whereas asymptomatic patients should also be evaluated and endoscopically examined depending on caustic substance type. Depending on lesion and burn extent and severity feeding can be interrupted, and broad-spectrum antibiotics, and drugs that suppress HCl acid production proton pump inhibitors can be administered. The placement of a nasogastric/jejunal catheter under endoscopic guidance may be a feeding option. The use of corticosteroids remains controversial; however, in patients with severe esophageal burns classified as grade ≥2B according to the endoscopic esophageal burn assessment scale [41], their administration may be considered. The ESPGHAN guidelines recommend a short course of high-dose corticosteroids—typically for 3 days—in patients with deep circumferential injuries to potentially reduce the risk of stricture formation [42].
The role of sucralfate in preventing caustic agent-induced strictures is controversial, and limited studies have been conducted to date. A recent study showed that sucralfate significantly reduced the incidence of esophageal stricture following the ingestion of caustic agents in children versus control treatment. High doses of sucralfate therapy for grade IIB esophageal injury, can improve prognosis and reduces the risk of stricture formation [43].
In the next phase, after the injury, an upper gastrointestinal series are recommended to identify strictures and appropriate treatment dilations.
8. Complications
The ingestion of caustic substances in children may be accompanied by immediate or long-term complications. Immediate complications are related to the type of substance type, the damage degree and substance location (esophagus or stomach) and potentially life-threatening. Late complications include the occurrence of esophageal strictures, development of esophageal carcinoma in 2% of patients with very severe lesions, and pyloric stenosis.
Conclusion
In conclusion, esophageal burns are the most serious injuries following the ingestion of caustic substances. The most common causes are alkaline and acidic cleaning substances. After the initial necrosis, further mucosal degradation is observed during the first week post ingestion. Additionally, the ingestion of foreign bodies poses several risks depending on object type, shape and size of. Batteries, magnets, sharp objects, and lead-containing objects containing are considered more dangerous; however, even the most “innocent” ones can cause serious complications depending on their location.
Recent management strategies emphasize urgent endoscopic removal of high-risk foreign bodies such as esophageal button batteries and multiple high-power magnets; early endoscopy for symptomatic caustic ingestions; the avoidance of procedures during the high-risk tissue fragility window and the use of standardized clinical pathways to guide risk stratification, imaging, and timely intervention. The pediatrician’s role is very important in educating parents about implementing, strategies to prevent their children from, having easy access to caustic substances and dangerous foreign bodies.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


