




Graphical abstract. GA, gestational age; PND, postnatal day; PMA, postmenstrual age; SNUH, Seoul National University Children’s Hospital; aOR, adjusted odds ratio; CI, confidence interval; NDI, neurodevelopmental impairment.
Introduction
Bronchopulmonary dysplasia (BPD) is a chronic lung disease primarily caused by inflammation and lung injury resulting from mechanical ventilation and supplemental oxygen therapy, which can disrupt alveolar and vascular development [1,2]. Although interventions such as antenatal glucocorticoids, surfactant replacement therapy, and lung-protective ventilation strategies have improved survival rates, they have no significantly reduced BPD among survivors, particularly in extremely preterm (EP) infants [3-5]. In Korea, the overall incidence of moderate-to-severe BPD in very low birth weight infants was approximately 30% [6], with no significant change from 2013 to 2020 [7]. The incidence increases as gestational age (GA) decreases, reaching 50%, 72%, and 87% in infants born at 26−27 weeks, 24−25 weeks, and 22−23 weeks of gestation, respectively [7]. BPD is associated with significant long-term morbidities, including persistent respiratory impairments, increased susceptibility to pulmonary infections, a higher rate of re-hospitalization for respiratory issues, and adverse neurodevelopmental outcomes such as cerebral palsy (CP) and cognitive delays [8-11]. A recent study highlighted the significant effect of BPD on pulmonary function and structure, which has important implications for the treatment and management of preterm infants [12]. As a result, numerous strategies have been studied to prevent and treat BPD, aiming to minimize lung injury, promote lung development, and improve long-term outcomes.
Postnatal systemic corticosteroids, which help reduce lung inflammation, have been widely studied for their potential to prevent and treat BPD. A recent meta-analysis showed that early systemic corticosteroids treatment (initiated within the first 6 days of life) reduced the risk of BPD and combined outcome of mortality or BPD at 36 weeks’ postmenstrual age (PMA) [13]. However, it increased the risks of CP, and the combined outcome of mortality or CP, which these risks being more pronounced with dexamethasone [13]. Due to these adverse effects, multiple national and international organizations recommend against using dexamethasone within the first week after birth to prevent BPD in EP infants [14-16]. Regarding late treatment (delayed until after the first week of life) with systemic corticosteroids, a 2021 Cochrane systematic review demonstrated that only dexamethasone, not hydrocortisone, reduced the risk of BPD and the composite outcome of death or BPD at 36 weeks’ PMA [17]. This meta-analysis reported that dexamethasone did not increase the risk of CP or neurodevelopmental impairment; however, it was noted that the individual studies were underpowered to assess long-term effects [17]. Recent studies have shown that the effect of postnatal systemic corticosteroids, particularly dexamethasone, on survival free of CP varied depending on the risk of BPD [18,19]. Specifically, while dexamethasone had harmful effects in infants at a low risk of BPD, it improved survival free of CP in those at a high risk of BPD [19]. As a result, there is growing consensus that the targeted administration of postnatal corticosteroids should be considered for infants at high risk of severe BPD. However, uncertainty remains regarding the optimal criteria for initiating postnatal corticosteroid treatment.
The respiratory severity score (RSS) is a simple, noninvasive tool for assessing respiratory failure. It can be used continuously without the need for blood sampling and is calculated as the product of mean airway pressure (MAP) and the fraction of inspired oxygen (FiO2). RSS has been shown to closely correlate with oxygenation index in newborns receiving mechanical ventilation [20]. Furthermore, it has become a valuable tool for predicting BPD severity by quantifying the extent of respiratory support required. A retrospective study conducted by our unit from 2010 to 2014 found strong correlations between RSS on postnatal day (PND) 14, 21, and 28 and the risk of death or severe BPD in EP infants [21]. Recent studies have reported consistent findings [22,23]. Given its potential to stratify risk for BPD, our unit developed and implemented a postnatal systemic corticosteroid protocol in 2015, using RSS as a key criterion for initiating treatment.
This study evaluates the impact of our RSS-guided postnatal systemic corticosteroid protocol on severe BPD and neurodevelopmental impairments over 2 periods: before and after its implementation, in EP infants receiving mechanical ventilation.
Methods
1. Study design and population
This historical comparison study was conducted in the neonatal intensive care unit of Seoul National University Children’s Hospital, comparing the preprotocol period (2010–2014, phase I) with the postprotocol period (2016–2022, phase II). We included preterm infants born at <28 weeks’ gestation who required mechanical ventilation at 14 days postnatally. Exclusion criteria were: (1) major congenital anomalies; (2) death within the first 14 days; and (3) incomplete data.
2. RSS-guided postnatal systemic corticosteroid protocol
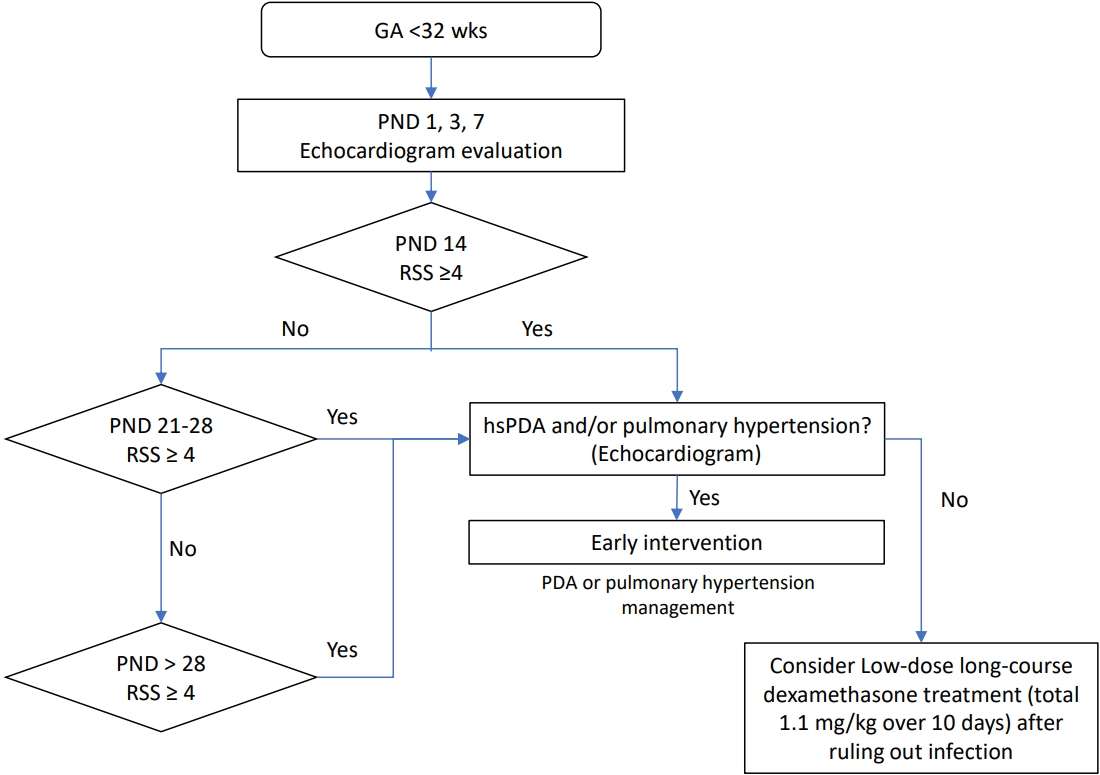
Our institution developed a postnatal systemic corticosteroid protocol for infants at high risk for severe BPD in 2015, guided by the RSS (Fig. 1). Before 2015, systemic steroid administration was considered for preterm infants struggling with ventilator weaning, starting around PMA 30−31 weeks. The developed protocol is as follows: preterm infants born at <28 weeks’ gestation who are still on mechanical ventilation after the second week of life are considered candidates for corticosteroid treatment. If the RSS is less than 4 or if the ventilator settings are showing a decreasing trend, treatment is withheld, and continuous RSS monitoring is performed weekly. If the RSS is 4 or higher, or if there is a sustained increase in ventilator settings, an echocardiogram is performed to assess for hemodynamically significant patent ductus arteriosus (PDA) or pulmonary hypertension. Pulmonary hypertension is suspected based on symptoms of recurrent hypoxemia, leading to echocardiography. Echocardiographic diagnosis was based on one or more of the following findings: (1) tricuspid regurgitation peak velocity (estimated right ventricular systolic pressure) >2.8 m/sec, (2) any cardiac shunt with bidirectional or right-to-left shunt flow, or (3) any degree of interventricular septal flattening [24]. If relevant findings are present, treatment for PDA or pulmonary hypertension is prioritized. Additionally, blood sampling is conducted to check for signs of infection. If no such findings are present, intravenous dexamethasone treatment is considered. The same low-dose, long-course dexamethasone regimen, with a total total of 1.1 mg/kg over 10 days, was used both before 2015 and after the implementation of the RSS-guided protocol. Dexamethasone is administered as a low-dose, long-course regimen, with a total of 1.1 mg/kg given over 10 days. The dosage schedule is as follows: D1, D2: 0.1 mg/kg every 12 hours; D3, D4: 0.075 mg/kg every 12 hours; D5–7: 0.05 mg/kg every 12 hours; D8: stop; D9: 0.05 mg/kg every 12 hours; D10: end.
3. Data collection
The medical records of the study population were reviewed retrospectively. Prenatal factors included oligohydramnios, gestational diabetes mellitus (DM), premature rupture of membranes (PROM), histologic chorioamnionitis and antenatal steroid use. Neonatal and demographic factors included GA, birth weight, small for GA (SGA), multiple birth, sex, neonatal resuscitation at birth, respiratory distress syndrome (RDS), respiratory support at PND 14, treated pulmonary hypertension, treated PDA, necrotizing enterocolitis (NEC, stage≥2) [25], congenital infection, culture-proven sepsis, and term-equivalent brain magnetic resonance imaging findings including intraventricular hemorrhage (IVH, grade≥3) [26] or hemorrhagic infarction and periventricular leukomalacia (PVL). The RSS was calculated using continuous vital sign data from electronic medical records, determined by multiplying the MAP by the FiO2 on an hourly basis. Clinical data on systemic corticosteroid use were collected, including PMA and PND at the initiation of first corticosteroid administration, as well as the total cumulative dose of steroids. Respiratory and neurodevelopmental outcomes were also analyzed. Short-term respiratory outcomes were defined as BPD severity at PMA of 36 weeks based on the Jensen 2019 criteria [27], while long-term respiratory outcome was assessed by respiratory support at discharge and hospital readmission within 12 months due to respiratory causes. Neurodevelopmental outcomes were assessed at a corrected age of 18–24 months based on severe neurodevelopmental impairment (NDI), defined as the presence of one or more of the following: CP, visual impairment (VI, no functional vision in one or both eyes), or hearing loss (HL) requiring a permanent hearing aid.
4. Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics ver. 24.0 (IBM Co., USA). Continuous variables are reported as mean±standard deviation or median with interquartile range, while categorical variables are presented as frequencies with percentages. Group differences were analyzed using Student t test or Wilcoxon rank-sum tests for continuous variables and chi-square or Fisher exact tests for categorical variables. Binary logistic regression was used to compare the 2 period groups, adjusting for GA and antenatal steroid administration, and ventilator mode at PND 14. A P value <0.05 was considered statistically significant.
5. Ethics statement
This study was approved by the Seoul National University Hospital’s Institutional Ethics Committee (IRB approval number: H-2408-032-1558). The study adhered to the principles of the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective nature of this study.
Results
During the 2 distinct study periods, a total of 567 neonates born at <GA 28 weeks were admitted. After excluding infants who died within first 7 days (n=36), were not intubated at PND 14 (n=314), had incomplete data (n=7), or had major congenital anomalies (n=2), a total of 208 patients were enrolled. Of these, 108 infants (51.9%) were in phase I, while 100 infants (48.7%) were in phase II.
1. Baseline characteristics and morbidities between the 2 phases
Baseline characteristics and clinical data are summarized in (Table 1). GA (25.8±1.4 weeks vs. 25.6±1.4 weeks, P=0.330) and birth weight (765.5±211.3 g vs. 755.9±166.7 g, P=0.719) were similar between phases I and II. The proportion of antenatal steroid administration increased in phase II (74.1% vs. 86.9%, P=0.024). Other perinatal factors, including SGA, multiple births, sex, oligohydramnios, gestational DM, preeclampsia, PROM, histological chorioamnionitis, and neonatal resuscitation at birth were comparable between the 2 phases.
RSS above 4 at PND 14 was similar between the phases (17.6% vs. 21.0%, P=0.599). However, significant differences in ventilator modes at PND 14 were observed between phases I and II (P<0.001). High-frequency oscillatory ventilation and neurally adjusted ventilatory assist were used more frequently in phase II, whereas the use of conventional ventilation was less common compared to phase I. Other morbidities that could impact respiratory status, including RDS, surfactant administration method and protocol, treated PDA, treated pulmonary hypertension, NEC, congenital infection, and culture-proven sepsis, also showed no significant differences between the phases. The proportion of PVL was lower in phase II, but the difference was not statistically significant (9.1% vs 3.1%, P=0.373), and there was no significant difference in IVH ≥grade 3 or hemorrhagic infarction.
2. Comparison of corticosteroid administration characteristics between the 2 phases
The characteristics of corticosteroid administration are summarized in Table 2. The proportion of dexamethasone use was higher in phase II compared to phase I (17.6% vs. 33.0%, P=0.017). In phase II, dexamethasone was initiated earlier than in phase I (PMA: 31.1 weeks vs. 29.0 weeks, P=0.027; PND: 34.5 days vs. 29.0 days, P=0.037). The total cumulative dose of dexamethasone had a median of 1.1 mg/kg in both groups, with no significant difference.
3. Respiratory and neurodevelopmental outcomes between the 2 phases
Respiratory and neurodevelopmental outcomes were compared between phases I and II (Table 3). Among respiratory outcomes, the proportion of infants with Jensen grade 0 (i.e., without BPD) was significantly higher in phase II (15.2% vs. 30.2%, adjusted odds ratio [aOR] [95% confidence interval, CI], 2.31 [1.10–4.83], P=0.024). While not statistically significant, there was a trend toward a lower proportion of Jensen grade 3 in phase II (17.2% vs. 9.4%; aOR [95% CI], 0.42 [0.17–1.08]; P=0.064). The proportion of other Jensen grades, respiratory support at discharge, and readmission within 12 months showed no significant differences between the 2 phases. For neurodevelopmental outcomes, the proportion of death or any NDI was lower in phase II (22.4% vs. 17.0%; aOR [95% CI], 0.70 [0.34–1.45]; P=0.337), although the difference was not significant. The proportions of any NDI including CP, HL, and VI, and mortality was not significantly different between the 2 phases.
4. Subgroup analysis according to the administration of corticosteroid
Table 4 presents clinical outcomes among infants receiving steroids. A reduction in Jensen grade 3 BPD was observed in phase II compared to phase I, with borderline statistical significance (47.4% vs. 21.2%; aOR [95% CI], 0.26 [0.07–1.00]; P=0.050). In contrast, the proportion of Jensen grade 1 BPD increased significantly in phase II (5.3% vs. 33.3%; aOR [95% CI], 12.22 [1.19–125.90]; P=0.035). Respiratory support at discharge and readmission within 12 months were similar between the 2 phases. For neurodevelopmental outcomes, the proportion of death or any NDI tended to decrease in phase II compared to phase I, although the difference did not reach statistical significance (22.2% vs. 6.1%; aOR [95% CI], 0.28 [0.04–1.91]; P=0.195). The proportion of any NDI alone also decreased in phase II compared to phase I, showing borderline statistical significance (23.5% vs. 3.1%; aOR [95% CI], 0.11 [0.01–1.19]; P=0.069). There were no significant differences in the proportions of CP, HL, VI, and mortality between the 2 phases.
Table 5 presents clinical outcomes among infants who did not receive steroids. The proportion of infants with Jensen grade 0 significantly increased in phase II (18.8% vs. 42.9%; aOR [95% CI], 3.46 [1.53–7.83]; P=0.003). The proportions of Jensen grade 1, 2, and 3, respiratory support at discharge, and readmission within 12 months were not significantly different between the 2 phases. Neurodevelopmental outcomes and mortality rates showed no significant differences between the 2 phases.
Discussion
After the implementation of the RSS-guided postnatal systemic corticosteroid protocol, a greater proportion of infants received steroids at an earlier time point. Among all infants, the proportion with Jensen grade 0 lung status increased in phase II, a trend particularly pronounced among those who did not receive steroids. Among infants receiving steroids, the severity of BPD appeared to improve in phase II compared to phase I. Specifically, the proportion of infants with Jensen grade 3 BPD decreased with borderline statistical significance, whereas the proportion of infants with Jensen grade 1 BPD increased significantly in phase II. There was no significant difference in the proportion of death or any NDI between the 2 phases.
This protocol considered several factors when determining the timing of steroid administration, the target population, as well as the type and dosage of the steroid. First, based on existing studies reporting that early dexamethasone administration within 7 days of life is associated with poor neurological outcomes [13], steroid administration within the postnatal 7 days was avoided in this protocol. Second, before deciding on steroid administration, echocardiography was performed on infants with an RSS score of 4 or higher, or those with increasing ventilator settings, to check for hemodynamically significant PDA or pulmonary hypertension. Existing studies have shown that the presence of a moderate/large PDA with a left-to-right shunt persisting for 7–14 days increased the risk of BPD [28,29], and prolonged exposure to PDA raised the risk of BPD-associated pulmonary hypertension [30]. Therefore, in cases with hemodynamically significant PDA, the treatment of PDA was prioritized before initiating steroid therapy. Early pulmonary hypertension, detected between 7 and 14 days of life, is also known to be associated with an increased risk of moderate/severe BPD at PMA 36 week [24,31]. Severe BPD encompasses various clinical phenotypes, including parenchymal disease and abnormal pulmonary vascular development. Early disruption of pulmonary angiogenesis impairs alveolarization and causes sustained abnormalities in lung structure, leading to BPD and pulmonary hypertension [32]. Given that steroids reduce lung parenchymal inflammation, their effectiveness may be diminished in cases of BPD accompanied by early signs of pulmonary vascular disease. Third, the decision to use dexamethasone as the sole postnatal steroid in this protocol was based on evidence demonstrating its superior efficacy in improving respiratory outcomes, particularly in facilitating extubation and reducing BPD, compared to hydrocortisone [17,33]. The dosage was minimized, considering its potential impact on neurological developmental outcomes. Fourth, this protocol determined steroid use based on RSS levels. RSS is a simple, noninvasive tool for assessing lung disease severity in preterm infants. Multiple studies have demonstrated its efficacy in predicting severe BPD or death in EP infants [21,22,34]. According to the study published by Jung et al. [21], conducted on patients from this unit, the RSS cutoff values for predicting severe BPD or death were 3.0 on PND 14, 3.6 on PND 21, and 3.24 on PND 28. Based on these results, this protocol set the RSS cutoff for initiating steroid administration at 4.
The most significant result of implementing this protocol was the increase in Jensen grade 0 in Phase II. This result was primarily driven by a significant increase in Jensen grade 0 among the infants who did not receive steroids. These findings suggest that the protocol may have effectively identified infants at lower risk of BPD who did not require steroid treatment. According to a recent meta-analysis on the effect of systemic dexamethasone on survival free of CP, as the risk of BPD increased, the risk difference in survival free of CP between the dexamethasone and control groups also increased [19]. Notably, in groups with a BPD risk of less than 30%, dexamethasone had a detrimental effect. Therefore, it is crucial to identify infants at low risk of BPD and avoid unnecessary steroid use. From this perspective, this protocol may have clinical utility in reducing unnecessary steroid use.
Among the infants who received steroids, the increase in Jensen grade 3 BPD and the decrease in grade 1 BPD suggest a shift toward lower overall BPD severity in phase II. This may be associated with the timing of steroid administration. In phase II, steroids were initiated earlier compared to phase I (median PMA: 31.3 weeks vs. 29.0 weeks, median PND: 34.5 days vs, 29.0 days). Additionally, the timing of administration was more consistent in phase II, with a narrower interquartile range of PMA (29.3–35.3 weeks vs. 27.9–30.7 weeks) and PND (22.8–66.0 days vs. 22.5–36.0 days) compared to phase I. Moreover, approximately 75% of infants received steroids within the first 5 weeks of life in phase II. This finding that earlier administration of steroids may have a positive impact on BPD outcomes, is consistent with other existing studies [35,36]. Kwok et al. [36] found that when dexamethasone was administered at 2–3 weeks of chronological age, it was associated with lower rates of severe BPD and/or death, earlier extubation, and decreased respiratory support at discharge compared to administration after 5 weeks. Cuna et al. [35] concluded that moderately late treatment (postnatal 14–28 days) was associated with fewer days on mechanical ventilation and supplemental oxygen compared to delayed treatment (postnatal 29–42 days). Prolonged mechanical ventilation can lead to ventilation-induced lung injury through proinflammatory signaling pathways, exacerbating lung damage and a generalized systemic inflammatory response [37,38], which may be reduce the effectiveness of the anti-inflammatory effect of postnatal steroids when administered later.
Data derived from current evidence, including meta-analyses, are inconclusive on the long-term neurodevelopmental consequences of the late dexamethasone administration [17,32]. In this study, there were no significant differences in death, any NDI, or the composite outcome of both between phase I and phase II, despite a higher rate of steroid use in phase II. Among the infants receiving steroids, the risk of any NDI tended to decrease with borderline statistical significance in phase II; however, this pattern was not observed among infants who did not receive steroids. This may be related to the possibility that implementing this protocol effectively identified infants at high risk of severe BPD, and applying the treatment reduced the risk of severe BPD. However, as this is a retrospective study with a small sample size, it is limited in drawing definitive conclusions about the long-term effects of dexamethasone. Therefore, further studies are needed to confirm these findings.
This study has several limitations. First, its retrospective design may introduce selection bias, and the relatively small sample size limits the generalizability of the findings. In particular, the subgroup analysis presented in Table 4, which involved infants who received corticosteroid treatment (n=19 and n=33), may limit the reliability and robustness of the observed associations. Nevertheless, the study provides meaningful insights by systematically evaluating the impact of an RSS-guided corticosteroid protocol in a high-risk preterm population over an extended period, using a consistent steroid regimen. Second, loss to follow-up, particularly due to referral to nearby regional hospitals, limited the availability of complete long-term neurodevelopmental outcome data. While the follow-up rate of our unit was relatively high, missing data from transferred patients may have introduced bias, potentially underestimating or overestimating the true neurodevelopmental outcomes. Future large-scale, prospective, multicenter studies are warranted to validate the efficacy and safety of RSS-guided corticosteroid administration, to more accurately assess long-term respiratory and neurodevelopmental outcomes, and to minimize biases associated with small sample sizes and incomplete follow-up.
In conclusion, our RSS-guided postnatal systemic corticosteroid protocol effectively identified high-risk BPD infants, enabling targeted and early steroid use. This approach reduced the risk of severe BPD without negatively affecting neurodevelopmental outcomes. By providing a more precise and individualized strategy for postnatal corticosteroid therapy, this study may help optimize BPD management in EP infants.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


