




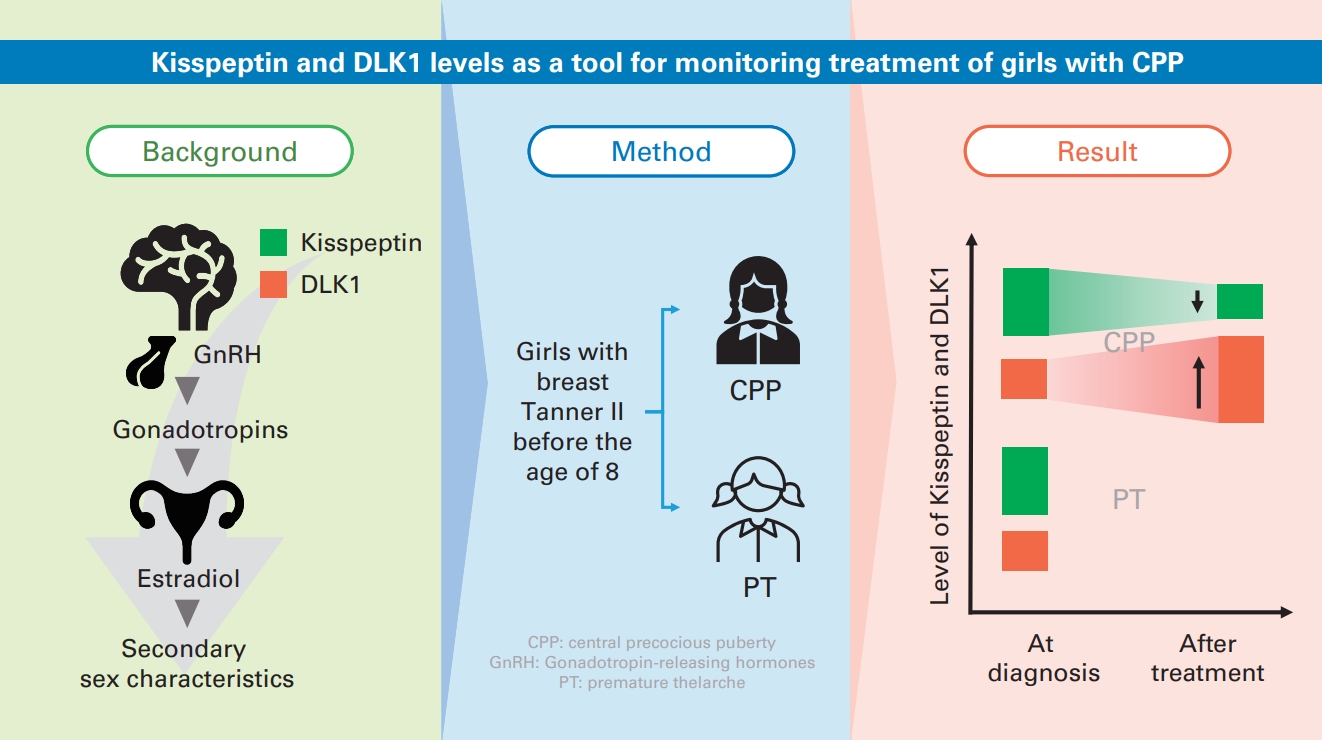
Graphical abstract. DLK1, delta-like 1 homolog; CPP, central precocious puberty; GnRH, gonadotrophin-releasing hormone; PT, premature thelarche.
Introduction
Central precocious puberty (CPP) refers to the expression of puberty-related symptoms in girls prior to the age of 8, which is caused by the activation of the hypothalamic-pituitary-gonadal (HPG) axis [1]. Premature thelarche (PT) is the development of breast in the absence of other signs of puberty. PT is regarded as a normal variant of development. In contrast to in CPP, the HPG axis is not active in PT [1].
The pathophysiology of idiopathic CPP is complex, involving environmental, nutritional, and genetic factors. Numerous genes, such as KISS1, KISS1R, MKRN3, and DLK1, have been identified as a cause of familial form of CPP [2-5]. Early increases in HPG axis activators, such as kisspeptin, and decreases in axis inhibitors, such as DLK1, were discovered to have a crucial role in the development of CPP [1-6].
Gonadotrophin-releasing hormone (GnRH) stimulation test is the gold standard for diagnosis of CPP, but there are some limitations including the unavailability in certain parts of community, time-consuming, costly, and uncomfortable [7-9]. In terms of treatment, it is challenging to ascertain the efficacy of GnRH analogs in CPP patients after diagnosis. Kisspeptin directly controls pulsatile GnRH release which leads to luteinizing hormone (LH) and follicle-stimulating hormone (FSH) release from anterior pituitary gland and a subsequent activation of the production of sex steroid from the ovaries [6]. Delta-like 1 homolog (DLK1) is a negative regulator of Notch signaling, and it has been hypothesized that DLK1 may inhibit the formation, maturation, and secretion of kisspeptin neurons [6,10-12].
The aim of the study was to compare serum kisspeptin and DLK1 levels in girls with CPP at diagnosis and follow-up to an age-matched PT group, and to explore if kisspeptin and DLK1 might be utilized as a marker for CPP diagnosis and follow-up.
Methods
1. Participants
This prospective longitudinal study included 48 girls with premature breast development before 8 years of age, who visited the pediatric endocrinology outpatient clinic of King Chulalongkorn Memorial Hospital from November 2019 to July 2022. The demographic data collected included chronological age, age of breast onset, bone age, breast Tanner stage, pubic hair Tanner stage, height (standard deviation score, SDS), weight (SDS), and body mass index (BMI) (SDS). The Tanner stage was utilized to assess the maturation of breasts and the development of pubic hair through visual inspection and palpation by pediatric endocrinologist. National Standard Growth Curve of Thailand's Ministry of Public Health was used to determine SDS for height, weight, and BMI (Department of Health, Ministry of Public Health, Thailand; reference for weight and height in Thais aged 1 day to 19 years; Bangkok, Thailand 2020). The Greulich and Pyle technique was utilized to determine the patient's bone age.
2. Blood sampling and GnRH stimulation test
All subjects were performed a GnRH stimulation test in the morning. At the beginning of the test, an intravenous cannula was inserted and serum levels of LH,FSH,estradiol, kisspeptin, and DLK1 were obtained. Triptorelin Acetate (Dipherelin, Ipsen Pharma Biotech, Boulogne-Billancourt, France) 100 μg was administered as subcutaneous injection at upper external side of forearm. Blood samples (serum LH and FSH) were obtained at 30, 60, 90, 120 minutes after Triptorelin injection. The girls were divided into 2 groups according to the GnRH stimulation test results. CPP was defined by peak LH from GnRH stimulation test ≥6 IU/L. The girls who demonstrated lower values were classified as the PT group.
Intramuscular Triptorelin pamoate was administered to all patients diagnosed with CPP at a dosage of 11.25 mg every 12 weeks. Serum LH, FSH, estradiol, kisspeptin, and DLK1 levels were collected 1 hour after intramuscular Triptorelin pamoate treatment to monitor pubertal suppression at the 6 months of the therapy. Blood samples were centrifuged and subsequently stored at a temperature of -80°C until further analysis.
3. Hormonal assays
Serum LH, FSH, and estradiol levels were measured using electrochemiluminescent immunoassay (ECLIA) by Elecsys Assay commercial kits (Roche Diagnostics GmbH, Mannheim, Germany) and analyzed in a Cobas 6000 and 601 automated system. The detection limits for LH and FSH were 0.1 U/L. LH has approximately 2% intra-assay and interassay variability. FSH has 2.8% intra-assay variability and 4.5% interassay variability. Estradiol was measured using the Elecsys Estradiol III Assay (Roche Diagnostics GmbH) through ECLIA. The method's lower limit value was 5 pg/mL, and its intra-assay and interassay variability values were up to 6.7% and 10.6%, respectively.
Analysis of serum kisspeptin levels were done using ELISA (MyBioSource, San Diego, CA, USA) with the detection limit of 31.2–2,000 pg/mL and intra-assay and interassay coefficients of variation <12%. DLK1 levels were analyzed by ELISA (IBL America, Minneapolis, MN, USA) with the lower detection limit of <0.4 ng/mL, and mean intra-assay variability 5%, mean interassay variability 8.1%.
4. Statistical analysis
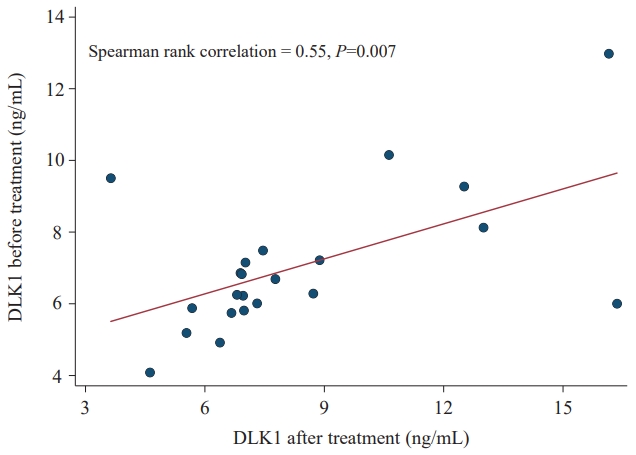
Statistical analyses were performed using the Stata 15.1 (StataCorp LLC, College Station, TX, USA). Nonnormally distributed data were shown as median and interquartile range (IQR), whereas normally distributed data were represented as mean and standard deviation. Difference in continuous and categorial data between the 2 groups was tested using a Wilcoxon rank-sum test and chi-square test, respectively. Wilcoxon sign-rank test was used to compared serum kisspeptin and DLK1 levels between before and after GnRH analog treatment in CPP girls. P value <0.05 was considered statistically significant. Spearman rank correlation was utilized for correlation analysis.
5. Ethical consideration
Informed consent was obtained from all subjects and their parents upon providing the study purpose and processes involved. The study was approved by the Institutional Review Board (IRB) ofthe Faculty of Medicine, Chulalongkorn University (IRB No. 205/64) with the international guidelines for human research protection as Declaration of Helsinki, The Belmont Report, CIOMS Guideline and International Conference on Harmonization in Good Clinical Practice (ICH-GCP).
Results
The study involved a total of 48 girls, who were divided into 2 groups: CPP (n=24; mean age, 7.7±0.7 years) and PT (n=24; mean age, 7.4±0.8 years). There was no significant difference in age, Tanner stage, weight-SDS, height-SDS, and BMI-SDS between CPP and PT groups (Table 1). Significant bone age advancement was observed in the CPP group compared to the PT group (median [IQR]: 1.08 years [0.08–2.03 years] vs. 0.11 years [-0.84 to 0.71 years], P=0.001, respectively). CPP group had significantly greater basal LH, basal FSH, basal LH/FSH ratio, basal estradiol, peak LH, and peak LH/FSH ratio in response to GnRH stimulation test than PT group (P<0.05) (Table 2).
At diagnosis, the CPP group showed similar baseline serum kisspeptin levels (median, 50.5 pg/mL; IQR, 38.2–77 pg/mL) compared to the PT group (median, 49.5 pg/mL; IQR, 39.7–67.6 pg/mL); however, the differences were not statistically significant. Baseline serum DLK1 levels were not significantly different between the CPP and PT groups (median [IQR]: 6.5 ng/mL (5.9–7.5 ng/mL) and 6.0 ng/mL (4.4–14.4 ng/mL), respectively).
After 6 months of GnRH analog treatment in CPP girls, serum kisspeptin levels were lower (median, 46.4 pg/mL; IQR, 37.1–60 pg/mL) than the levels prior to treatment (median, 50.5 pg/mL;IQR, 38.2-77 pg/mL)(P=0.002)(Table 3, Fig. 1).In contrast, serum DLK1 levels after GnRH analog treatment was increased in comparison to those before treatment (median [IQR]: 6.5 ng/mL [5.9–7.5 ng/mL] and 7 ng/mL [6.7–8.9 ng/mL])(P=0.002)(Table 3, Fig. 2). Serum kisspeptin and DLK1 levels at the time of diagnosis and after 6 months of treatment shown a positive correlation (Figs. 3, 4). This study observed a statistically significant link between blood levels of kisspeptin and DLK1 in the same patient at the time of diagnosis and after a 6-month period of therapy.
Discussion
In the early stages of puberty, when breast bud is the only apparent sign, the progression of puberty in girls is not always continuous. It is unclear whether the child has CPP or PT at this time. The prompt management of girls with CPP is crucial for preserving their final height and menstrual cycle. This study aimed to assess the differences in serum kisspeptin and DLK1 levels between patients with CPP and PT. Our results revealed that the initial serum concentrations of kisspeptin and DLK1 in girls with CPP were not significantly different from those with PT. Consequently, baseline serum kisspeptin and DLK1 levels cannot be used as a reliable biomarker for differentiating CPP and PT girls. In addition, changes in kisspeptin and DLK1 levels following pubertal suppression in CPP patients treated with GnRH analog were evaluated. However, the 6-month follow-up after treatment of CPP girls revealed a significant decrease in serum kisspeptin levels and an increase in serum DLK1 levels compared to those before treatment.
Kisspeptin is a peptide encoded by the Kiss1 gene that is responsible for GnRH pulsatile release. A defect in kisspeptin signaling might result in precocious or delayed puberty [13-16]. The hypothalamus secretes dynorphin, neurokinin B, and kisspeptin, which interact with the kisspeptin receptor (KISS1R)in GnRH-secreting neurons to enhance the amplitude and frequency of GnRH pulsatility and initiate pubertal development [2]. The correspondence between blood levels of kisspeptin and their levels in the hypothalamus remains unknown. A recent study has provided evidence indicating that the levels of kisspeptin in the blood of female rats are mostly influenced by the expression of Kiss1 mRNA in the ovaries [17]. At diagnosis of CPP or PT, we demonstrated that baseline serum kisspeptin level of girls with CPP was not significantly higher than that of age-matched PT controls. In agreement with the findings of other research, the serum kisspeptin levels of girls with CPP and PT did not differ significantly [18-22]. However, our results are limited by the absence of a prepubertal control group to compared kisspeptin levels. Many studies have been conducted to investigate the relevance of serum kisspeptin levels in the diagnosis of CPP [14,18,20,21,23-27]. In studies exploring serum kisspeptin levels in CPP, girls with CPP have been found to have higher kisspeptin levels than prepubertal control girls [23-27]. Abacı et al. [27] discovered that the serum kisspeptin levels of CPP and PT girls were significantly higher than those of prepubertal controls, but that there was no significant difference between girls with CPP and PT. In addition, a recent systematic review and meta-analysis revealed that kisspeptin levels in girls with CPP were higher than those in controls. Therefore, they concluded that kisspeptin levels alone cannot be used as a reliable diagnostic criterion for CPP when compared to PT [18].
Consistent with the findings of this study, Demirbilek et al. [7] reported that the serum kisspeptin levels of CPP girls prior to treatment were significantly higher than those of age-matched controls. However, these levels decreased significantly after 6 months of effective gonadotropin-releasing hormone analog treatment.Comparable outcomes were seen in this investigation after 6-month period of pubertal suppression, which resulted in considerably lower levels of kisspeptin, FSH, LH, and estradiol in blood drawn an hour after receiving an injection of 11.25 mg of GnRH analog. Consequently, serum kisspeptin levels can be used to evaluate the efficacy of GnRH agonist treatment for CPP [7,24].
The DLK1 gene is identified in a cluster of imprinted genes on the human chromosome 14q32.2. In animal studies, DLK1 functions as a negative regulator of the Notch signaling system, which is essential to the development of kisspeptin neurons. In addition, it has been demonstrated that DLK1 is also expressed in hypothalamic nuclei, including the mediobasal hypothalamus, a crucial region for the regulation of GnRH secretion via kisspeptin neurons [6]. The actual mechanism by which DLK1 influences pubertal time remains poorly understood. In 2017, Dauber et al. [10] reported the first familial case of CPP caused by a DLK1 loss-of-function mutation. They discovered a 14 kb deletion in DLK1 in five female patients with CPP in a Brazilian family, which resulted in undetectable DLK1 levels (<0.4 ng/mL). Montenegro et al. [12] revealed that the genomic deletion in DLK1 in familial CPP patients resulted in undetectable serum DLK1 levels (<0.4 ng/mL), which was consistent with the findings of Gomes et al. [11]. For serum DLK1 levels, we observed that there was no significant difference in baseline serum DLK1 levels between CPP and PT groups, and there was no research on serum DLK levels for distinguishing CPP from PT girls. There is currently no established cut-off value for serum DLK1 levels to diagnose CPP.
We discovered a substantial increase in serum DLK1 in the same CPP patients after pubertal suppression due to GnRH analog treatment, compared to their baseline levels at the time of diagnosis. However, there is few research on serum DLK1 levels. To assess the clinical use of serum DLK1 levels as a monitoring tool for CPP treatment, additional research is required. The limitations of this study are the single-center design, absence of a normal prepubertal control group, and small sample size. To clarify the role of kisspeptin and DLK1 in the adjunctive diagnosis of CPP and monitoring after GnRH analog therapy, additional large-scale research is required.
In conclusion, after 6 months of pubertal suppression with GnRH analog in CPP group, serum kisspeptin and DLK1 levels are lower and higher than at diagnosis, respectively. Serum kisspeptin and DLK1 cannot differentiate between CPP and PT, although they may be used to assess treatment efficacy.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


