


Introduction
Seasonal influenza is a major contributor to respiratory infections in children. The disease causes high morbidity among children, and annual vaccination is the most effective infection prevention strategy1). In particular, children aged less than 6 years are reportedly more vulnerable to influenza infection than children from other age groups, and the infected children pose a significant burden to their families2). Considering the high risk of infection with seasonal influenza among children and the development of complications associated with the disease, the vaccinating of children younger than 6 years is crucial. The Korean Pediatric Society recommends that all children aged 6 to 59 months should receive the influenza vaccine annually. However, the nationwide influenza vaccination coverage for children younger than 6 years in 2014 was estimated at 79.2%3). Although vaccination has reached the ideal coverage rate for infection control, we believe that a higher vaccination rate is better considering the direct and indirect disease burden to the families and society4,5). As caretakers are the primary decision-makers about childhood vaccination, the analysis of parents' opinions about vaccination against influenza and the identification of the underlying drivers and barriers to influenza vaccination is essential.
In this study, we hypothesized that educational intervention could modify parents' opinions and influence their attitudes toward childhood vaccination. We adopted the Health Belief Model, which proposes that individuals make health decisions based on their perception of factors such as disease susceptibility and severity, decision-associated benefits, and barriers to vaccination6). Using the framework of this model, we explored the factors that affected the parents' decisions to vaccinate children against influenza and quantified the relative importance of each associated factor.
Materials and methods
This study included 639 parents whose children were aged <6 years by October 2014. We provided specific education and collected information from the parents who visited the Pediatric Departments of the Korea Cancer Center Hospital and Seoul Eulji Hospital, the Jungnang Borough Office Healthcare Center, and 3 day-care centers in Seoul. This study was approved by the Institutional Review Board of Korea Cancer Center Hospital (approval number: K-1503-001-005).
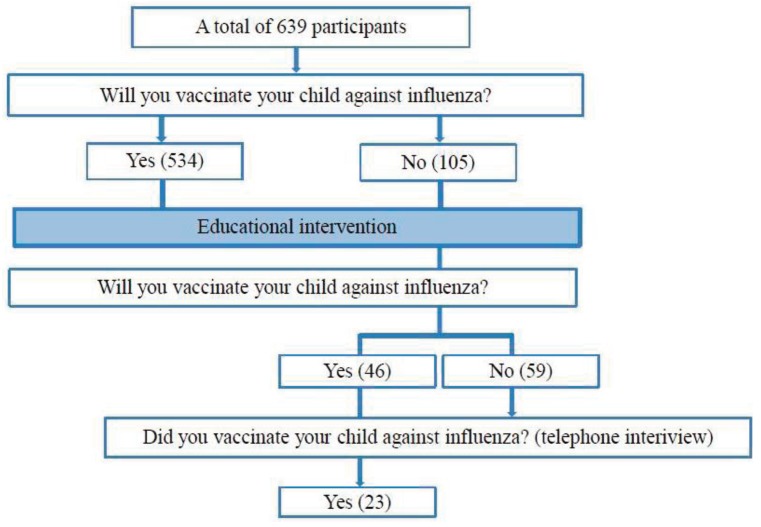
The parents were first asked to complete a survey questionnaire consisting of 15 statements and were then asked to attend a brief written educational session (Table 1). After the session, the parents were asked to reply to 13 of the 15 statements to determine changes in opinion (Fig. 1). Two statements were not included in the postintervention survey and consequently were not included in the analysis. The educational sessions included general easy-to-understand information about influenza and vaccination. The sessions emphasized the severity of the disease in children and the importance of vaccination and included information on possible side effects of vaccination, prevention of side effects, and management of side effects if they occur. Utilizing the Health Belief Model, the survey questionnaire assessed the parents' knowledge about influenza infection and vaccination, child's susceptibility to influenza, disease severity, and barriers to childhood vaccination.
In our study, the elements of the Health Belief Model were divided into 2 groups: drivers and barriers. Factors such as perceived susceptibility to the disease, perceived severity of the disease, benefits of vaccination, and cues to action were regarded as drivers to vaccination, whereas factors such as cost, side effects, and inconvenience of vaccination were regarded as barriers to vaccination (Table 1). The level of agreement or disagreement to the statements was assessed by asking the participants to rank their agreement with each statement of the questionnaire on a scale from 1 (strongly disagree) to 5 (strongly agree). For the 5 statements that assessed the negative perception (‘I have unfavorable opinions about influenza vaccination,’ ‘The probability of side effects of influenza vaccination is high,’ ‘Influenza vaccination weakens the immune system,’ ‘Receiving the influenza vaccine is not convenient,’ and ‘Influenza vaccine is expensive’), the lower scores indicated a favorable opinion about influenza and vaccination. The questionnaire also contained demographic information, including the parents' sex, age, employment status, household income, and education level. Before and after the educational intervention, parents were asked whether they would have their children vaccinated against influenza that year. In addition, telephone interviews were conducted from December 2014 to January 2015 to identify parents who had vaccinated their children against influenza in that season (Fig. 1).
We used descriptive statistics to compare the selected sociodemographic variables. All group comparisons between the pre- and posteducational intervention were analyzed using analysis of covariance (ANCOVA), and the level of education and household income were evaluated using ANCOVA. The agreement scores between the preand posteducational intervention were compared using Student t test. P values smaller than 0.05 indicated significant differences between subgroups. The IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA) was used for data analysis.
Results
1. Modifying factors – characteristics of the participants
A total of 639 parents participated in the survey. The mean age of the participants was 34.4 years (range, 18–66 years), and 88.9% were women. Of the total, 72.9% had a college-level or higher education, and 38.1% reported to be employed. Furthermore, 41% of the participants had a household income of US $2,500–4,500 (Table 2).
Table 3 shows the correlation between the participants' sociodemographic information and the likelihood of parents to agree with childhood vaccination. The parents' sex and employment status were not significantly correlated with their decisions about influenza vaccination (P=0.055 and P=0.541, respectively). However, the level of education and household income were strongly correlated with the likelihood of parents to agree with childhood vaccination (P=0.047 and P=0.043, respectively).
2. Pre- and posteducational intervention
Among the 639 participants, regardless of their opinions about vaccination before attending the educational sessions, there were significant differences in the agreement scores between pre- and postintervention. After adjusting for the educational level and household income, the agreement scores were increased for most of the statements but were decreased for the negative perception statements following the educational intervention (Table 4). The number of parents who agreed to vaccinate their children after attending the educational sessions was increased from 83.57% before the sessions to 90.77% after the intervention. However, the intervention did not significantly change the unfavorable opinions about influenza vaccination and the agreement scores for the convenience of receiving the vaccination.
Before the intervention, 105 parents reported not to agree to vaccinate their children against influenza (Fig. 1), but 46 parents (43.8%) changed their opinions after the intervention. Table 5 shows the changes in the agreement scores of these 46 participants between pre- and postintervention. Compared to the total participants, this group strongly agreed with most of the statements and presented higher agreement scores. In particular, the unfavorable opinions about vaccination improved significantly after the intervention in this group. However, the intervention did not change the opinion of 59 out 105 parents about childhood vaccination (Table 6).
Telephone interviews were conducted with 459 parents after 2 to 3 months of the completion of the intervention and the survey. Among these, 404 participants reported having vaccinated their children. In addition, of the 105 parents with unfavorable opinions about influenza vaccination, 46 participants changed their opinions after the intervention (Fig. 1); among these, 33 were reached by telephone and 23 reported to have vaccinated their children against influenza.
3. Drivers and barriers to vaccination
Table 4 shows the change in the agreement scores of the questionnaire after the educational intervention. We divided the statements into 2 categories—drivers and barriers—to identify the factors that encouraged and discouraged parents from vaccinating. Parents significantly changed their opinions after the intervention in these 2 categories, except for 4 statements. The recommendation from the physician achieved the highest score as a driver whereas the cost of the vaccine had the highest score as a barrier to vaccination.
Discussion
In this study, we evaluated the effect of an educational intervention on parents' opinions about influenza infection and vaccination. Our results demonstrated that the intervention improved the parents' attitudes towards vaccination. Moreover, the results of the telephone interviews confirmed that the changes in opinion led to action, i.e., vaccination.
Influenza can be effectively prevented by vaccination. Owing to the high disease burden in the younger population, especially children aged <60 months, an increase in vaccination coverage is critical. However, the increase in childhood vaccination coverage depends on the caretakers' awareness and positive attitude towards vaccination. Previous studies analyzed the parental decision-making about childhood vaccination and reported that the drivers to childhood vaccination against influenza were a desire to prevent the disease and the physician's recommendation to vaccinate children7,8). Other studies reported that the barriers to vaccination were vaccination safety, convenience and access to vaccination, disease severity, and child susceptibility to influenza9,10,11). Another study demonstrated the importance of intervention to increase the vaccination coverage12). On the basis of these results, we evaluated the changes in the parents' opinions pre- and postintervention and the factors that most strongly influenced their decision to vaccinate their children against influenza. The objective of this study was to assess the parents' general perception of influenza and vaccination and to evaluate the effectiveness of educational interventions in improving their opinions about vaccination.
This study was based on the hypothesis that the increase in influenza vaccination coverage is necessary for public health and that this goal can be achieved by appropriate education about the disease and vaccination.
Previous studies demonstrated that interventions either increase or decrease the perception of a population about vaccination coverage. In the Philippines, a media campaign in 1990 reportedly increased the vaccination coverage. During the period of the media intervention, the proportion of fully vaccinated children was increased significantly from 54% to 65%13). Another study assessed the effect of an Internet-based vaccine education program on influenza vaccination rates and reported that the subjects with access to these resources were 6.7% (95% confidence interval [CI], 1.46–12.30) more likely to be vaccinated than individuals without access to the information. Moreover, the former group was 11.6% (95% CI, 3.6–19.5) more likely to visit health service providers14).
In our study, the postintervention agreement scores for most statements indicated a significant improvement in the knowledge and perception about vaccination and influenza. Furthermore, the likelihood of parents to agree with childhood vaccination depended on their socioeconomic status, household income, and the level of education. Therefore, ANCOVA was conducted to confirm the independent effect of educational sessions on changes in the parents' opinions, and the association remained significant even after adjusting for these modifying factors.
After the agreement scores were compared between the pre- and postintervention, the specific factors that encouraged and discouraged parents from vaccinating their children were identified. Parents significantly changed most of the statements after the educational sessions, except for 4 statements (Table 4). With respect to the drivers to vaccination, the recommendations from the media or physicians were effective in improving the vaccination coverage, considering that the total scores for these 2 statements were comparatively higher in the vaccinated group. This result emphasizes the importance of media and medical professionals in reinforcing the need for influenza vaccination, as demonstrated in previous studies. With regard to the barriers to vaccination, the cost of vaccination discouraged the parents the most. However, the agreement scores for this factor significantly changed after the intervention. In contrast, the agreement scores for the inconvenience of receiving the influenza vaccine did not change significantly after the intervention. These results indicate that the opinion about the convenience of receiving the vaccine cannot be easily changed through education. Therefore, supportive government policies and community assistance are necessary to increase access to vaccination and thus alleviate this barrier. Moreover, it was not possible to significantly change parents' unfavorable opinions about vaccination in general through education. However, as unfavorable opinions about vaccination may be due to various reasons, we think further studies are necessary to specify this statement. This specification may improve the understanding of the factors that discouraged parents from vaccinating their children and how parents' opinions can be changed through education.
Initially, 105 parents had unfavorable opinions about childhood vaccination against influenza. Of this group, 46 parents changed their opinions after attending the educational sessions (Table 5). Compared with the total participants (639 parents), this group strongly agreed with most of the statements and achieved higher total agreement scores. The unfavorable opinions were significantly changed in this group after the intervention. These results suggest that eliminating the unfavorable opinions about vaccination was the primary contributor to the shift in the parents' decision about vaccination. Therefore we believe it is crucial to specify these 'unfavorable opinions about vaccination', and implement educational interventions to reduce these feelings.
The results of the telephone interview indicated that, of the 46 parents who had changed their opinion about vaccination after the educational intervention, 23 had their children vaccinated. These 23 participants account for approximately 70% of the 33 parents who were reached by telephone. We believe that this result demonstrates the effectiveness of the intervention in increasing vaccination coverage because these parents not only changed their opinions about childhood vaccination but also allowed their children to be vaccinated. These numbers are relevant because they indicate that education can change the parents' perception of diseases and vaccination and the behavior of parents concerning the preservation of child health, as previously demonstrated by the Health Belief Model.
Despite these obvious changes in perception through education, additional studies are necessary to enhance the magnitude of these changes. Our results indicated that 59 parents—approximately 8% of the total sample—did not change their opinions about vaccination even after the intervention (Table 6) and the intervention did not significantly change the agreement scores in this group. In addition to this group, there were some participants whose agreement scores to some of the statements did not change significantly despite the intervention. This suggests that other factors other than educational sessions may affect parent's decisions on childhood vaccination. Some of these factors include more complicated dynamics, such as the healthcare system, government policies affecting the cost, and accessibility to vaccination, among other factors.
The socioeconomic status of the parents affected the decision-making about childhood vaccination against influenza. Parents with lower household income and lower education levels tend not to vaccinate their children, and therefore the provision of focused and frequent educational interventions for this group is essential. In addition, further studies are needed to implement these educational programs effectively, taking into account the drivers and barriers to vaccination.
This study has limitations. First, the number of participants was small and a larger study sample may better evaluate the effects of educational interventions. Second, the tool used for parental education was based on text-based material. Although the content was easy-to-understand, visual aids may help parents to understand the content. Third, we did not evaluate the reasons based on which parents had their child vaccinated during the telephone interview. This approach may help identify the drivers and barriers to vaccination.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


