


Introduction
Diffuse alveolar hemorrhage (DAH) is a clinical syndrome that is characterized by alveolar bleeding, which ranges from mild bleeding that requires chronic transfusions to catastrophic bleeding with hemoptysis, pulmonary infiltrates (typically diffuse and bilateral), and hypoxic respiratory failure1,2). The etiology of DAH is diverse and includes pulmonary capillaritis, drugs, toxins, allogeneic hematopoietic stem cell transplantation (HCT), coagulopathies, and blast lung injury. It is a life-threatening condition that is associated with a high mortality rate. However, the treatment of DAH is empirical and ranges from supportive treatment to high-dose corticosteroids, immunosuppressants, and plasmapheresis. Furthermore, the overall mortality remains high.
Recombinant factor VIIa (rFVIIa) was developed for the management of bleeding in hemophiliac patients with inhibitors or in FVII-deficient patients. Despite the narrow indications, the off-label use of rFVIIa has increased among nonhemophiliac patients in order to prevent or treat uncontrolled bleeding in adults, children, and neonates (including preterm neonates)3,4). Recombinant FVIIa has also been reported to have a significant hemostatic effect in patients with DAH5,6,7,8). However, many reports on the use of rFVIIa for DAH were based on adult patients, and few have evaluated rFVIIa use in pediatric patients. This review discusses the diagnosis and etiologies of DAH, the treatment options, and a new treatment paradigm that includes the off-label use of rFVIIa in pediatric patients.
Diagnosis of DAH
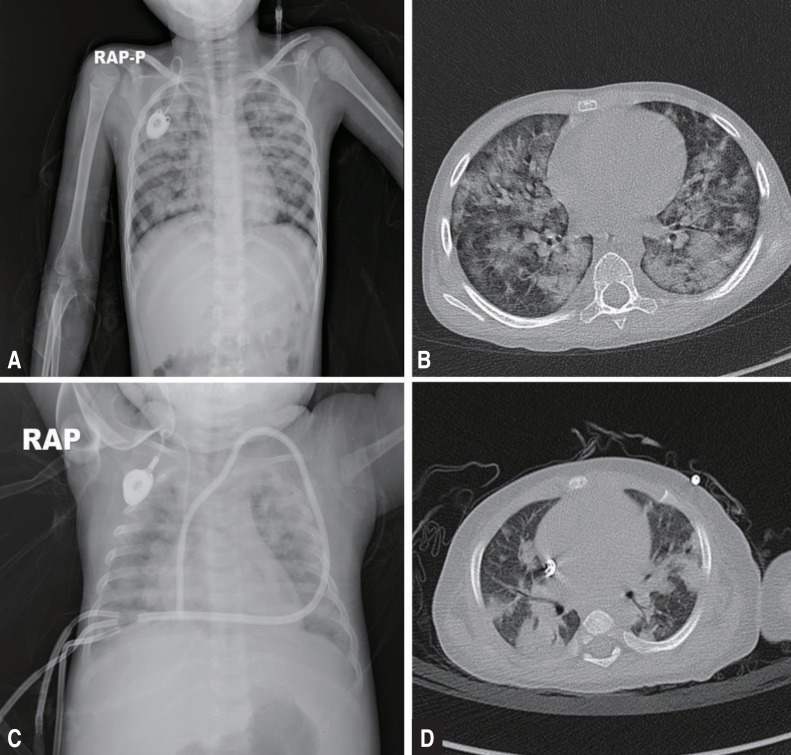
DAHs is characterized by hypoxia, progressive dyspnea, cough, infiltrates on a chest x-ray (CXR), progressively more blood in successive aliquots of bronchoalveolar lavage (BAL) fluid, and the absence of evidence for infectious etiologies in the BAL fluid cultures or other diagnostic studies. Robbins et al.9) first described DAH in 1989. The disease is characterized by damage to the alveolar-capillary basement membrane, which allows red blood cells to enter the alveolar spaces. In adults, DAH is typically a syndrome of pulmonary capillaritis, which is observed with autoimmune diseases or after HCT, and pulmonary hemorrhage after HCT has a high mortality rate10,11). However, DAH may also occur as a consequence of diffuse alveolar damage in patients with acute respiratory distress syndrome/acute lung injury (ARDS/ALI), and can occur in any age group secondary to various underlying diseases and conditions12,13,14,15,16,17). The differential diagnosis is broad, and the etiologies of DAH can be broadly divided according to immune- and non–immune-mediated causes (Table 1)18). A careful history and physical examination can often help to establish the risk factors and most likely etiology of the alveolar hemorrhage. Flexible bronchoscopy is recommended as soon as possible. The diagnosis is established when sequential BAL fluids are progressively more hemorrhagic. Samples should also be sent for routine bacterial, fungal, viral, and Pneumocystis jiroveci studies to rule out infection. The role of open or transbronchial lung biopsies has not been established, but in any child presenting with DAH of unclear cause (particularly after cardiovascular causes have been ruled out), a lung biopsy is strongly recommended to determine the underlying etiology12,19,20). Imaging studies including CXR and high-resolution chest computed tomography scans can provide additional information to support a diagnosis of DAH. However, radiological findings are frequently nonspecific and subject to change throughout the course of the disease. Typical patterns indicative of DAH include focal or diffuse areas of ground glass opacities or consolidations consequent to alveolar filling (Fig. 1). Laboratory studies usually include a complete blood count with differential; coagulation studies; serum blood urea nitrogen and creatinine analysis; antineutrophil cytoplasmic antibody (ANCA) testing (cytoplasmic [c-ANCA] and perinuclear [p-ANCA]); antigen-specific enzyme-linked immunosorbent assay (proteinase 3 or myeloperoxidase-ANCA); analyses of antiglomerular basement membrane antibodies, anti-nuclear antibodies, rheumatoid factor, and antiphospholipid antibodies; urinalysis with urine sediment assessment; and a urine drug screen (Table 2)2).
Treatment of DAH
DAH is a general alveolar response associated with many underlying diseases and conditions. This response can be categorized into 3 subtypes; acute macroscopic bleeding, chronic microscopic alveolar bleeding, and blast lung injury8). DAH, particularly acute macroscopic hemorrhage, has a very high mortality rate; therefore, prompt and aggressive acute management of DAH is critical for survival. It is important to treat the alveolar hemorrhage separately from the underlying diseases, which are treated with plasmapheresis, corticosteroids, immunosuppressants, and antivirals or antibiotics for example (Table 1)8). Acute management of DAH involves supportive care including ventilator support, which ranges from oxygen supplementation to mechanical ventilation with high positive end-expiratory pressure (PEEP). PEEP during mechanical ventilation may produce a tamponade effect to limit capillary bleeding. The coagulation cascade should be evaluated, and any coagulation abnormalities should be corrected. Commonly accepted targets are platelet counts more than 50,000/µL and a prothrombin time-international normalized ratio less than 1.5. Depending on the causes of the coagulation, platelet transfusions, vitamin K supplements, cryoprecipitates, and fresh frozen plasma can be administered for correction.
To control the inflammatory activity, prompt administration of high-dose corticosteroids has been recommended along with treatment for the underlying cause of the hemorrhage. Corticosteroids have been accepted as a mainstay of treatment in most cases, including DAH after HCT, and are aimed at reducing possible acute inflammatory responses to hemorrhage induced by lung alveolar epithelial swelling, thrombotic microangiopathy, and inflammatory cells and cytokines12,20,21). Treatment with high-dose corticosteroids is typically initiated with intravenous methylprednisolone at a dose of 500 mg to 2 g/day or 30 mg/kg/day for the first 3 to 5 days, followed by gradual tapering5,10,20,22). However, these treatments are insufficient to stop acute macroscopic pulmonary bleeding and can be fatal if the etiology is infectious or if the patient is in an immunocompromised state. Despite the widespread use of high-dose corticosteroids for DAH, the overall mortality has remained high; thus, additional treatments for hemostasis are urgently needed.
Traditionally, other treatment modalities for hemostasis have included the use of antifibrinolytics, specifically lysine analogues tranexamic acid (TXA) and epsilon aminocaproic acid (EACA). Although the evidence available for the use of these antifibrinolytics in patients with hematological disorders is limited, they have been used to control perioperative bleeding, mainly in cardiac surgery23,24). In addition to intravenous delivery of TXA, both aerosolized and intrapulmonary administrations have been used to treat DAH and have yielded positive results25). However, a study of TXA in patients with acute promyelocytic leukemia did not reveal any difference in mortality due to bleeding between the patients who received TXA and those who did not26). In addition, some studies have reported an increased risk of postoperative seizures in patients who received TXA, which has since been withdrawn from the market27). An alternative treatment, EACA, which was used in addition to corticosteroids in patients with posttransplant DAH, was reported to result in a lower 100-day mortality rate than treatment with corticosteroids alone28). However, this drug is not available in Korea, and a recent study that included more patients reported that adjuvant treatment with EACA did not yield a difference in the outcomes of patients with DAH after HCT. The overall mortality on day 100 was still high, at 85%29).
In contrast, rFVIIa has generated significant interest and controversy as a potential 'broad-spectrum hemostatic agent' to enhance hemostasis in patients with life-threatening bleeding. Numerous case reports and clinical studies have reported the effectiveness of rFVIIa in various conditions including thrombocytopenia, functional platelet defects, hemorrhagic complications after HCT (e.g., DAH and hemorrhagic cystitis), gunshot wounds, and coagulopathy of liver failure30,31,32,33,34,35,36,37). Whereas there is overwhelming evidence that rFVIIa has hemostatic effects in nonhemophiliac patients, information on the efficacy and side effects of rFVIIa in nonhemophiliac settings is largely anecdotal. Furthermore, many questions remain regarding the appropriate settings and guidelines for use; risks of thrombotic complications; and appropriate monitoring, dosing, and integration with transfusion therapy. A recent Cochrane review regarding the off-label use of rFVIIa concluded that therapeutic use of rFVIIa did not significantly decrease mortality compared with placebo (odds ratio [OR], 0.91; 95% confidence interval [CI], 0.78–1.06), nor did it significantly increase the incidence of thromboembolic events (OR, 1.18; 95% CI, 0.94–1.48). However, there was a trend towards control of the bleeding, and a lower number of transfusions favoring rFVIIa (OR, 0.95; 95% CI, 0.88–1.03; and OR, 0.94; 95% CI, 0.89–1.00), whereas there was a significant increase in arterial thromboembolic events (OR. 1.45; 95% CI. 1.02–2.05)38). Because this meta-analysis included a wide range of disorders (from HCT to trauma to hemorrhagic stroke), a significant effect on the outcome in one clinical setting might have been diminished by a lack of benefit in another. There are many anecdotal reports on the successful use of rFVIIa in patients with DAH following various diseases and injuries including pneumonia, HCT, metastatic cancer, idiopathic pulmonary hemosiderosis, and immune-associated vasculitis; therefore, the use of rFVIIa for the treatment of DAH deserves consideration.
rFVIIa treatment for DAH
There are an increasing number of studies in the literature supporting the use of rFVIIa to stop acute pulmonary hemorrhage. Due to the lack of a randomized controlled study, rFVIIa has been used in patients with severe pulmonary hemorrhage as a final effort to stop the bleeding. Recently, several studies have reported the successful use of rFVIIa for life-threatening DAH in adults, as well as in children and infants6,13,39,40,41,42). In refractory cases of immune- and non–immune-mediated DAH, including cases due to pulmonary vasculitis, connective tissue diseases, post-HCT, or infections, rFVIIa has been successfully administered both systemically (intravenously) and bronchoscopically. Although the optimal dose and dosing intervals remain to be determined, systemic administration usually involves the intravenous administration of 35–200 µg/kg as either a single dose or repeated doses every 2–4 hours5,7,40,43). Intrapulmonary therapy typically involves bronchoscopy, with a total dose of 50–90 µg/kg of rFVIIa diluted in normal saline and administered as either a single dose or, if bleeding continues, as repeated doses over 24 hours 8,13,44,45).
Recombinant FVIIa promotes hemostasis via both a tissue factor (TF)-dependent pathway at the sites of endothelial injury and a TF-independent pathway, directly activating factors IX and X on the surface of activated platelets in the absence of TF and at higher doses. Factor X subsequently converts prothrombin to thrombin, which in turn converts fibrinogen to fibrin. The alveolar TF concentration remains high in inflammatory pulmonary conditions including DAH, ARDS, and pneumonia, as well as after local lipopolysaccharide challenge in the alveoli6,46,47,48). The alveolar TF-rFVIIa complex activates coagulation factors IX and X, which in turn initiate a cascade of reactions, leading to thrombin burst and fibrin formation at the site of injury6). Given the separation between the alveolar and systemic compartments of the lung, rFVIIa requires a high systemic concentration to affect specific receptors in the alveolar compartment, similar to most biologics. This effect necessitates higher and repeated doses of rFVIIa, which may be associated with a higher risk of thromboembolic complications8,49,50). Recently, Pathak et al.42) reported that bleeding resolved in 22 of 23 DAH patients after systemically administered rFVIIa treatment, without adverse thrombotic events. However, the mean dose of rFVIIa required to control the bleeding was 5±3 mg, and the authors emphasized that an adequate antithrombin III level should be maintained during rFVIIa treatment to avoid the generation of thrombosis, an adverse effect7).
Meanwhile, successful outcomes have been reported for patients with DAH after treatment with intrapulmonary rFVIIa at a relatively low dose (50 µg/kg)6,13,41). Local administration of rFVIIa into the airways can ensure that it reaches the alveolar receptor (TF), and it may not have systemic adverse effects because the alveolocapillary membrane does not allow the transmembranous passage of rFVIIa. Pulmonary-administered rFVIIa combines with TF and can lead to balanced hemostasis, with a small dose of rFVIIa resulting in both durable hemostasis and a significant improvement in oxygen transport capacity. Moreover, the TF pathway inhibitor, an inhibitor of the local activation of factor X that is produced by alveolar macrophages, is highly expressed in the airspace in inflammatory conditions secondary to ALI. This characteristic may contribute to balanced hemostasis without the theoretical risk of intra-alveolar thrombotic complications when treating DAH with intrapulmonary rFVIIa8,51,52). Accordingly, the treatment with rFVIIa has a potentially high benefit-to-risk ratio in DAH when administered via the local intrapulmonary route.
rFVIIa treatment in pediatric patients
The off-label use of rFVIIa in pediatric patients has also increased despite the absence of adequate studies addressing safety and efficacy. According to a multicenter cohort study by Witmer et al.53), 83% of rFVIIa use was off-label, and the off-label use of rFVIIa increased 10 folds between 2000 and 2007. The Haemostasis Registry reported the results of off-label use of rFVIIa in 388 pediatric patients54). The median age was 12 months, and the median dosages (single and total doses) were 114 µg/kg and 1.2 mg, respectively. A reduction in the number of transfusions after the use of rFVIIa (P<0.01) was observed, and the subjective response rate was 82%. In both studies, thromboembolic complications were reported in 5.4% to 10.9% of patients, which were similar to the published rates for adults49,55,56). The results demonstrated that rFVIIa was an effective and safe hemostatic agent in severely ill children experiencing life-threatening hemorrhages and that rFVIIa, when administered along with standard treatment modalities, reduced blood product requirements in children3,53,54,57). However, the benefits of rFVIIa therapy in neonates and infants less than one year of age remain unclear. Young et al.57) reported that neonates had a lower response rate (47%) and a higher rate of thrombosis (17.6%) than older age groups (greater than one month of age). The SeveNBleeP registry (a Web-based registry of rFVIIa use in nonhemophiliac children) of 42 infants less than 1 year of age also revealed no significant reduction in the requirements for blood products after rFVIIa treatment and indicated that there was no significant increase in thromboembolism (2.4%)3). There is evidence that rFVIIa has a shorter half-life and more rapid clearance in children compared to adults; therefore, higher and more frequent doses of rFVIIa are often required to control significant bleeding in children, especially in neonates and infants less than 1 year of age3,54,57). Considering the relatively poor response to rFVIIa and that the levels of natural inhibitors of coagulation (proteins C and S and antithrombin-III) are reduced, the risk of thromboembolism can increase in neonates and infants, and the risk-to-benefit ratio can be higher. Thus, caution has been recommended when considering treatment of patients in this age group with rFVIIa.
Perinatal asphyxia, very low birth weight, mechanical ventilation, respiratory distress syndrome, exogenous surfactant therapy, sepsis, hypothermia, patent ductus arteriosus, and coagulopathies can also be causes of pulmonary hemorrhage in children including neonates4,58). There are few reports regarding the treatment of pediatric patients with rFVIIa for pulmonary hemorrhage (Table 3). The data for 37 patients have been published, and the outcome demonstrated a complete response (bleeding completely ceased) in 62% and a partial response (bleeding improved but did not cease) in 24% of the patients. No response to rFVIIa treatment was observed for 13.5% of the patients. Two thromboembolic complications were reported (5.4%)57,59). Twenty-nine patients received intravenous rFVIIa, with a median total dose of 175 µg/kg (range, 60–3,150 µg/kg), and satisfactory hemostasis was achieved through multiple doses of rFVIIa in most cases. Complete hemostasis was reported in 14 cases (48%), a partial response in 10 cases (35%), and no response in 5 cases (17%). Although these data were not the representative of the effect of rFVIIa for DAH in pediatric patients, intravenous rFVIIa appeared to be less effective for the treatment of pulmonary hemorrhage compared to other life-threatening hemorrhages in children, and this finding was consistent with those of previous studies40,57). It is possible that because of pharmacokinetic characteristics, higher and multiple doses of rFVIIa may be necessary to reach an adequate systemic concentration to affect TFs in the alveolar compartment of the lung and to achieve stable hemostasis in children; however, the potential risk for thromboembolic complications also increases concomitantly.
Following the report of Heslet et al.6), several case series have been reported the use of intrapulmonary rFVIIa for the treatment of DAH in pediatric patients. Eight patients were treated with intrapulmonary rFVIIa, and complete hemostasis was observed in all cases with a median dose of 50 µg/kg. Most patients showed a significant improvement in oxygenation capacity (PaO2/FiO2 ratio) on the days following rFVIIa treatment13,60), although one child experienced a thrombotic obstruction in the endotracheal tube (ETT)59). There was no evidence of intra-alveolar thrombotic deposition (hyaline membrane formation) after rFVIIa administration among the eight pediatric patients. The data also suggested that pulmonary hemostasis could be more easily induced from the alveolar side than from the endothelial side, and that the intrapulmonary administration of rFVIIa could be more effective for the treatment of DAH in both children and adults.
Collectively, the data have suggested that intrapulmonary administration of rFVIIa was effective in controlling DAH in pediatric patients who have a lower systemic risk of complications; however, the risk of critical airway or ETT obstruction in young patients should be carefully considered.
Conclusions
DAH should be suspected in any patient who presents with alveolar infiltrates on CXR, hypoxemia, anemia, and hemoptysis. It is a clinical syndrome that can be a manifestation of multiple different etiologies, and identification of the underlying etiology is important for determining the treatment options. In cases of life-threatening DAH, rFVIIa therapy along with the appropriate treatment for the underlying disease may contribute to patient survival. Although most of existing data are based on case series and reports; thus, the results could have been affected by selection bias, the available data have demonstrated the safety and efficacy of rFVIIa therapy in uncontrolled nonhemophiliac bleedings in pediatric patients. The limiting factors in its use include the high cost ($1,000 per gram) and the substantial risk for thromboembolic complications. In this regard, the intrapulmonary administration of a low dose of rFVIIa may be an effective and reasonable treatment option for DAH in children as well as in adults. However, without the appropriate treatment of the primary causes of DAH, rFVIIa therapy would only functions as a temporary solution. Additional data from prospective registries or randomized trials when feasible are necessary to further our knowledge regarding the use of rFVIIa in pediatric patients with DAH.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


