


Introduction
Hemorrhagic cystitis (HC) occurs in 9%-31% of all stem cell transplantation (SCT) recipients1,2,3,4,5,6). This complication is associated with increased morbidity and mortality, and particularly with urinary tract obstruction, renal dysfunction and renal failure, longer hospital stay, and increased hospital costs2,6,7,8,9,10). In the early period after SCT, chemotherapeutic agents such as cyclophosphamide and busulphan as well as irradiation administered during the pretransplant conditioning period can directly damage the bladder urothelium11,12,13,14,15). However, several complicating factors such as viral infection and acute graft-versus-host disease (GvHD) may cause HC in the late period following SCT3,11,14). In particular, a relationship between BK virus (BKV) infection and late-onset HC after SCT has been described1,3,16,17,18,19). Few reports have examined the impact of BKV infection on HC after SCT in Korea, where pediatric SCT has been performed since 198320,21).
This review will introduce the pathogenesis, clinical features, diagnosis, and treatment of BKV-associated HC after SCT.
Definition and grading of HC
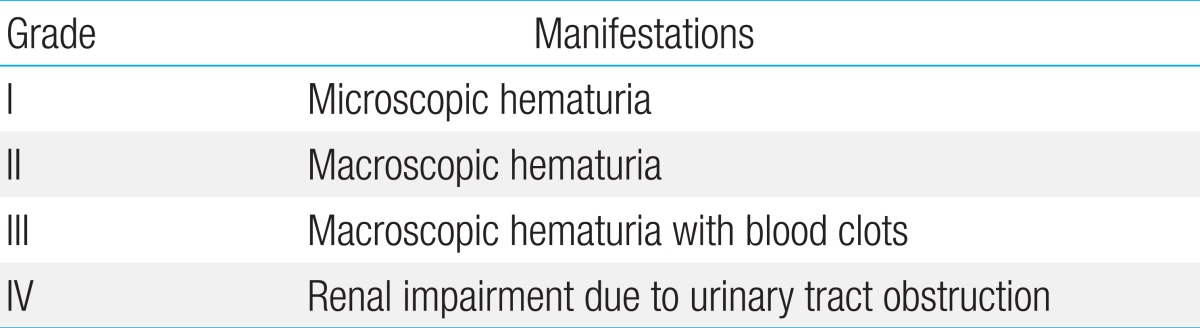
HC is defined as the development of microscopic or gross hematuria accompanied by lower urinary tract symptoms such as dysuria, frequent urination, urgency, and suprapubic pain. Other causes of bleeding such as bleeding tendency, bacterial or fungal infection, urinary tract mass, and vaginal bleeding should be excluded14,22). HC is categorized into four grades based on the severity of hematuria and its effect on the upper urinary tract (Table 1)14).
Causes of HC in SCT
While a variety of time frames ranging from 48 hours to two weeks have been proposed1,12,19,23,24), post-SCT HC is generally divided into early-onset or pre-engraftment HC and late-onset or postengraftment HC. Early-onset HC is caused by chemotherapeutic agents including cyclophosphamide, ifosfamide, busulphan, and etoposide. It can also be caused by the irradiation administered to the pelvic area during the pretransplant conditioning period and by sustained thrombocytopenia prior to engraftment11,12,14,25). Sustained thrombocytopenia and coagulopathy may also cause HC in the late period after SCT. However, infections with viruses such as BKV, JC virus, cytomegalovirus (CMV), and adenovirus have been reported as major causes of late-onset HC after SCT1,11,17,18,19,23). Urinary BKV is detected in 35%-100% of SCT recipients with HC1,3,17), compared to ranges of 10%-15%9,26,27), 4%-26%9,23,27), and 4%-7%3,26) for adenovirus, CMV, and JC virus, respectively. Thus, BKV is the most important pathogenic microorganism of late-onset HC after SCT.
Pathophysiology of BKV-associated HC
BKV is a member of the Polyomaviridae family and is a nonenveloped double-stranded DNA virus. First detected in 1970 in a postkidney transplant patient suffering from nephropathy, the virus was named "BK virus" after the patient's initials28). While BKV infects humans during childhood, a latent infection is maintained in the urinary tract16,29). Anti-BKV antibodies are present in approximately 80% of the general population and 91% of children aged 5-9 years30,31), and urinary BKV excretion is detected in 7%-14% of all immune-competent hosts30,32). Latent BKV is reactivated under immunosuppressed conditions, and BK viruria and viremia are detected in 53%-71%10,16,33) and 17%-51%10,34) of SCT recipients, respectively, regardless of HC status.
Late-onset HC after SCT is believed to develop in three phases14,16,33,35). The first is direct bladder mucosal damage caused by chemotherapeutic agents and irradiation received during pretransplant conditioning. During the second phase, BKV replication is activated in conjunction with the activated regeneration of damaged urothelial cells under the immunosuppressed status immediately following SCT. The third and final phase comprises an excessive inflammatory response of the reconstituted host immunity against activated BKV.
Although BK viruria were detected in 47%-52% of all SCT recipients1,26,33), only 38%-44% of them exhibited HC1,26). Moreover, 9%-50% of SCT recipients with HC did not exhibit BK viruria2,6,26,27,33). These findings indicate that factors other than BKV reactivation may contribute to the development of late-onset HC. Old age, acute GvHD, receiving stem cells from an unrelated donor, myeloablative conditioning, and allogeneic transplantation have all been suggested as possible contributing factors1,3,4,5,7,9,19,23,24,36,37).
Clinical features of BKV-associated HC
BKV infection after kidney transplantation mainly manifests as BKV-associated nephropathy while BKV infection after SCT mainly manifests as HC25,35). In various studies, BKV-associated HC was found to occur 25-57 days (median values) after SCT, with symptoms lasting for 10-38 days (median values)3,4,8,16,17,20,34,38). In terms of severity, HC of grades I, II, III, and IV occurred in 0%-30%, 16%-57%, 36%-67% and 0%-12% of cases, respectively3,4,8,20,38). Conservative care tends to be effective in patients with lower grades of HC, while those with higher grades may suffer from renal complications and even death.
Diagnosis of BKV-associated HC
BKV-associated HC is diagnosed when an SCT recipient with grade II or higher HC complains of lower urinary tract symptoms such as dysuria, urinary frequency, urgency, and suprapubic pain and shows laboratory evidence of BKV replication39). Ultrasonography can be useful in the evaluation of blood clot formation and the severity of upper urinary tract complications22). Polymerase chain reaction (PCR)-mediated detection of BKV DNA is the modality of choice for diagnosing BK viruria11). BK viruria tend to precede clinical symptoms of HC, and therefore, PCR for urinary BKV can be useful in the early diagnosis of BKV-associated HC1,17,19,33). Previous studies reported that 106 copies/mL or 9×106 copies/mL of urinary BKV DNA was an amount significantly associated with the development of BKV-associated HC1,17). However, PCR for blood BKV DNA may be an even more valuable predictor of the development of BKV-associated HC since compared with BK viruria, BK viremia has been shown to be more significantly related to the severity of HC and the development of renal complications2,6,8,10). In addition, various cutoff values of blood BKV DNA titers, including 103 and 104 copies/mL, have been reported to predict the development of BKV-associated HC2,17,34).
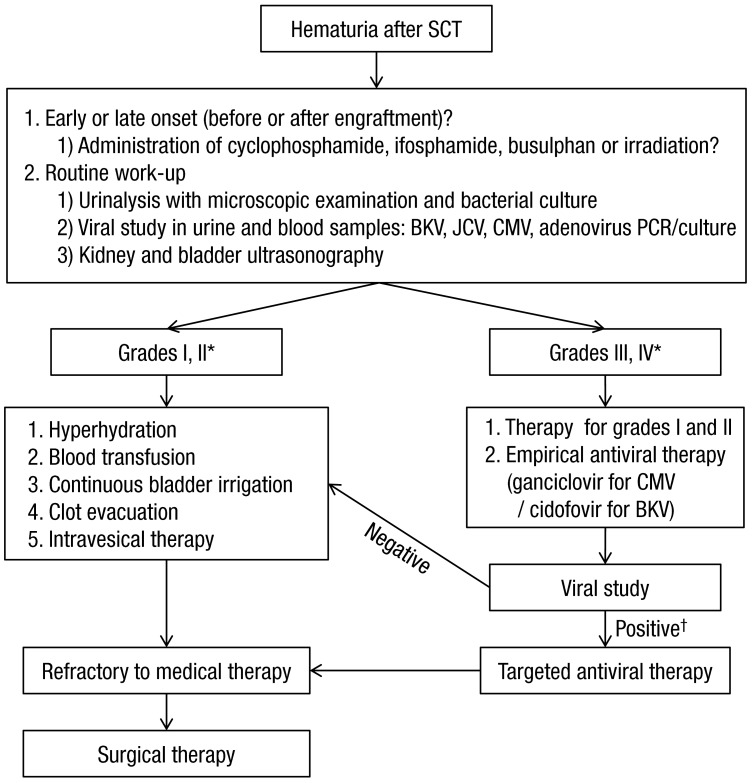
As mentioned above, late-onset HC after SCT can also be caused by other viruses such as adenovirus, CMV, JC virus, and human herpes virus 64,7,26,40). Therefore, blood PCR analyses, urinary PCR analyses, and urine cultures for other viruses should also be considered in SCT recipients with late-onset HC (Fig. 1).
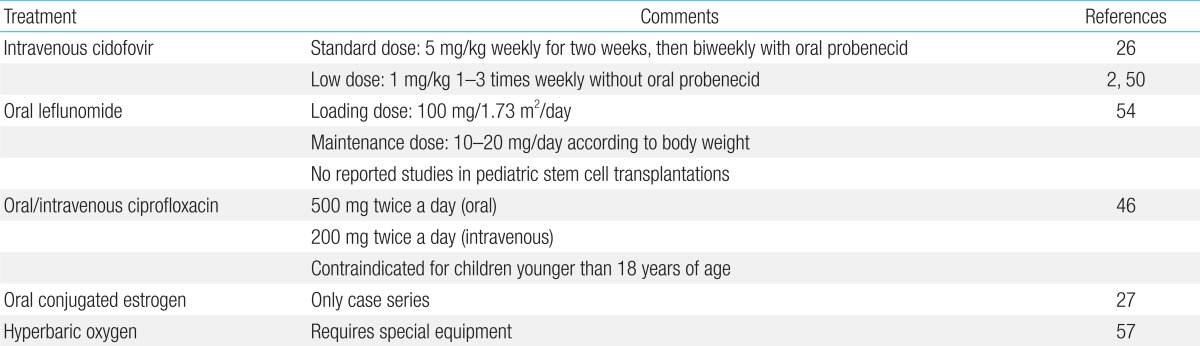
Treatment of HC
Many therapeutic modalities have been applied in HC; however, standard therapeutic guidelines have yet to be established22,35). In addition, evaluating the efficacy of these diverse modalities in clinical trials is complicated by their frequent concurrent administration35). Treatments can be selected based on the patient's general condition and HC grade, and most patients recover with conservative care11). Cases that do not respond to conservative care should receive intravesical therapy or systemic therapy (Table 2). Finally, surgical therapy can be considered if hemorrhage and urinary tract complications do not improve with medical therapy. A proposed diagnostic and therapeutic algorithm for SCT recipients with HC is shown inFig. 1.
1. Conservative care
It is necessary to reduce or stop immunosuppressive therapies in patients with BKV-associated HC35). However, this cannot be achieved in most patients due to the possible aggravation of GvHD. Therefore, analgesic therapy and intensive intensive intravenous hydration (3 L/m2/day) with forced diuretics are administered as an initial treatment11,22). In addition, a platelet count >50,000/µL and hematocrit >25% should be maintained via blood transfusion11,22,35). If HC symptoms do not respond to these therapies or blood clots form in the bladder, continuous bladder irrigation with normal saline through a three-way urethral catheter should be performed22).
2. Cystoscopy
If hemorrhage does not improve or a urinary tract obstruction develops after 3 to 4 days of conservative care, cystoscopy for the complete evacuation of blood clots should be performed22).
3. Intravesical therapy
If hemorrhage lasts for 7 to 10 days even after applying the aforementioned therapies, the intravesical instillation of topical agents should be considered22). Formalin, alum, prostaglandins, fibrin glue, and hyaluronic acid have all been applied intravesically as topical agents for HC7,8,9,23,41,42), but their efficacies have yet to be investigated in controlled studies. The use of formalin in children should be restricted due to the potential for severe complications including suprapubic pain, bladder scarring, and subsequent fibrosis and contracture22,43). While alum does not cause these local complications, the systemic absorption of aluminum may cause encephalopathy, seizures, and acidosis22,44,45).
4. Cidofovir
Cidofovir is a cytidine nucleoside analog and an effective antiviral agent. Cidofovir has been shown to inhibit intracellular BKV replication in vitro46,47). In addition, multiple studies have demonstrated the clinical and microbiological effects of intravenous cidofovir on BKV-associated HC2,26,38,48,49,50). In our hospital, all 11 pediatric SCT recipients who received intravenous cidofovir therapy showed a clinical response, and 10 of the recipients showed a microbiological response20). Importantly, no severe side effects of cidofovir were observed20). Nevertheless, the therapeutic efficacy of cidofovir has not been comprehensively confirmed through controlled studies, and the most appropriate dosing regimen (1 mg/kg vs. 5 mg/kg) is still unclear. In addition, the nephrotoxicity of cidofovir should be considered in SCT recipients who receive several nephrotoxic drugs concomitantly.
5. Leflunomide
Leflunomide, which is used in the treatment of rheumatoid arthritis, suppresses immune responses by inducing cytostasis, particularly in activated lymphocytes51,52). Since BKV relies on host factors for its replication, leflunomide is generally assumed to inhibit BKV replication by inhibiting DNA replication in BKV-infected cells51). The clinical and microbiological effects of leflunomide on BKV-associated HC in adult SCT recipients have been reported53). However, reports of its efficacy in children have been limited to kidney transplantation recipients54).
6. Ciprofloxacin
Although the quinolones are well-known as antibacterial drugs, they are also believed to inhibit intracellular BKV replication by inhibiting topoisomerase activity in BKV-infected mammalian cells55,56). The prophylactic and therapeutic effects of ciprofloxacin on BKV-associated HC in adult SCT recipients have been reported36,46). Quinolones are contraindicated in children younger than 18 years, and therefore, the effects of quinolones have not been studied in pediatric SCT recipients.
7. Estrogen
Estrogen has shown therapeutic efficacy against HC in children; it is believed that estrogen exerts these effects by stabilizing the microvasculature22,27). However, the evidence base consists of only a case report and a case series, neither of which was a controlled study. Moreover, other investigators have reported that estrogen is ineffective against HC7).
8. Hyperbaric oxygen
High-pressure oxygen generates a high oxygen gradient between the damaged urothelium and the surrounding healthy tissues. This oxygen gradient promotes macrophage invasion into the damaged tissues and stimulates angiogenesis and tissue healing via the secretion of cytokines by macrophages57). Therapeutic effects have been reported in adults and children with HC after SCT8,38,57), but only in case series and case reports. Moreover, this treatment requires specialized equipment for supplying high-pressure oxygen.
9. Surgical therapy
If HC is refractory to medical therapies, it may be treated with surgical interventions. Supravesical urinary diversion using a bilateral nephrostomy has shown efficacy in children with HC unresponsive to conservative care and intravesical therapy43). Supravesical urinary diversion prevents urokinase, which is secreted from renal cells, from reaching the bladder wall, thereby promoting bladder hemostasis43). Unfortunately, a life-threatening hemorrhage may require the selective embolization of vesical arteries or internal iliac arteries, and even cystectomies58,59). The proper indications and therapeutic efficacies of these surgical therapies have not yet been defined. Thus, future studies of surgical therapies for HC are required.
Conclusions
Although pediatric SCTs have been performed for approximately 30 years, only a few studies of HC, an SCT-related complication, have been reported in Korea. It is possible to predict the development of BKV-associated HC after SCT using urinary and blood BKV DNA titers. However, no standard guidelines for prophylactic or preemptive therapies have been established. A standard treatment for BKV-associated HC has also not been established. Therefore, various therapies are administered to patients based on the attending physician's decision. More studies aimed at establishing appropriate diagnostic and therapeutic guidelines for BKV-associated HC are necessary. Such efforts should be helpful in reducing SCT-related complications and mortality in SCT recipients.
 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


