Distinct age-dependent phenotypes of abnormal liver function tests derived from national Emergency Department data
Article information

Abstract
Background
Abnormal liver function tests (LFTs) are frequently performed in Emergency Departments (EDs); however, the systematic characterization of age-dependent clinical phenotypes and pathogen associations remains limited.
Purpose
Here we aimed to identify the distinct clinical presentations and pathogen-specific associations of pediatric and adult ED visits for abnormal LFTs.
Methods
This retrospective cohort study analyzed 26,874 ED visits for abnormal LFTs in South Korea's National Emergency Department Information System (2019–2023). Patients were stratified into pediatric (0–18 years) and adult (19–64 years) groups. We characterized the clinical presentations, concurrent diagnoses, temporal correlations with infectious pathogens, and metabolic comorbidity patterns.
Results
The ED visits included 3,152 pediatric (11.7%) and 23,722 adult patients (88.3%). Pediatric presentations demonstrated fever-predominant profiles (47.3%), respiratory symptoms (6.4%), and infectious disease diagnoses (39.8%) as well as temporal correlations with respiratory viruses (rhinovirus, r=0.30; adenovirus, r=0.28; P<0.001). Adult presentations revealed previously unreported population-level temporal associations with enteric pathogens, including astrovirus (r=0.35), sapovirus (r=0.32), enteropathogenic Escherichia coli (r=0.38), and enterotoxigenic Escherichia coli (r=0.36, all P<0.001) coupled with infectious gastroenteritis (20.9%) and upper gastrointestinal disorders, including gastritis (18.3%). Adults demonstrated clustering of the following metabolic comorbidities: dyslipidemia (7.9%), hypertension (7.8%), and diabetes (6.0%). During the coronavirus disease 2019 pandemic, pediatric visits remained stable, whereas adult visits increased following the implementation of social distancing measures (rate ratio, 0.82; P=0.004).
Conclusion
The ED presentation of abnormal LFTs results demonstrated distinct age-dependent phenotypes with divergent temporal pathogen associations. Pediatric cases reflected acute respiratory viral infections, whereas adult presentations showed novel population-level enteric pathogen associations with upper gastrointestinal disorders and clusters of metabolic comorbidities. These findings provide evidence supporting age-stratified diagnostic approaches for EDs.
Key message
Question: What are the clinical phenotypes and pathogen associations of pediatric and adult Emergency Department visits for abnormal liver function tests?
Finding: Pediatric visits showed fever-predominant profiles with temporal correlations with respiratory viruses, whereas adult visits revealed population-level temporal associations between enteric pathogens and infectious gastroenteritis, upper gastrointestinal disorders, and metabolic comorbidity clustering.
Meaning: These findings provide novel population-level evidence of age-specific pathogen associations and support distinct age-stratified clinical diagnostics.
Graphical abstract. GE, gastroenteritis; GI, gastrointestinal; HTN, hypertension; ED, Emergency Department; EPEC, enteropathogenic Escherichia coli; ETEC, enterotoxigenic Escherichia coli; COVID-19, coronavirus disease 2019.
Introduction
The liver plays a central role in metabolism, detoxification, and systemic homeostasis, with liver function disrupted by infections, metabolic disorders, toxins, and inflammatory processes [1,2]. Age-related changes in liver structure, immune responses, and regenerative capacity fundamentally modify disease susceptibility and clinical presentations [3,4]. Liver function tests (LFTs), which assess hepatocellular injury, cholestasis, and synthetic function, are essential tools for detecting liver dysfunction and guiding clinical management [5,6]. Abnormal LFTs are among the most frequently encountered laboratory abnormalities in Emergency Departments (EDs), often presenting diagnostic uncertainty requiring timely evaluation [5].
The clinical context of abnormal LFTs differs substantially between age groups. In children, transient aminotransferase elevations primarily result from acute respiratory viral infections, with most cases resolving spontaneously [7-10]. Real-world practice demonstrates that most children with abnormal LFTs have self-limited infectious etiologies requiring conservative management [11]. In contrast, adults predominantly present with chronic conditions, including metabolic dysfunction-associated steatotic liver disease (MASLD) [12]. Despite these recognized differences, systematic characterization of pathogen-specific profiles and temporal dynamics in ED presentations for abnormal LFTs across age groups remains limited.
The coronavirus disease 2019 (COVID-19) pandemic profoundly altered healthcare utilization and infectious disease epidemiology. Stringent infection control measures dramatically reduced circulation of respiratory and enteric pathogens, particularly affecting pediatric populations [13,14]. Pediatric ED utilization declined sharply during pandemic restrictions, while adult emergency care experienced complex shifts influenced by delayed care-seeking and lifestyle changes [14-17]. However, evidence examining how ED visits for abnormal LFTs evolved across pandemic periods and how visit patterns relate to age-specific pathogen epidemiology remains scarce.
In this study, we aimed to characterize age-specific patterns of ED visits for abnormal LFTs using nationwide data from South Korea. We examined clinical characteristics, pathogen associations, and temporal changes across COVID-19 social distancing periods.
Methods
1. Study design and data sources
This nationwide retrospective cohort study utilized data from the National Emergency Department Information System (NEDIS), a comprehensive registry capturing ED visits across South Korea. ED visits occurring between January 1, 2019, and December 31, 2023, were analyzed. Patients presenting with abnormal LFTs were identified using the International Classification of Diseases, 10th Revision (ICD-10) code R94.5 (abnormal results of liver function studies). Because NEDIS does not include quantitative laboratory values, this code was used to identify ED visits in which liver function abnormalities represented the primary or a clinically significant presenting concern requiring emergency evaluation, regardless of underlying etiology. Patients were categorized into pediatric (0–18 years) and adult (19–64 years).
2. Clinical variables and outcomes
Clinical variables extracted from NEDIS included patient demographics (age and sex), presenting symptoms at ED arrival, triage acuity, concurrent diagnoses, and disposition outcomes. Triage acuity was assessed using the Korean Triage and Acuity Scale (KTAS), a standardized 5-level triage system used nationwide, and was categorized as high acuity (KTAS levels 1–2), moderate acuity (KTAS level 3), and low acuity (KTAS levels 4–5). Disposition outcomes were classified as discharge from the ED, hospital admission to a general ward, admission to an intensive care unit, or transfer to another facility. Presenting symptoms were identified from structured symptom fields recorded at ED presentation and included fever, gastrointestinal symptoms (nausea, vomiting, or diarrhea), abdominal pain, respiratory symptoms, and other systemic complaints. Systemic symptoms included dizziness, myalgia, chest pain, and generalized weakness. Concurrent diagnoses were identified using ICD-10 codes assigned during the ED visit and were grouped according to major ICD-10 diagnostic chapters to characterize the clinical context accompanying abnormal LFT-related visits.
3. Definition of COVID-19 social distancing periods
To evaluate temporal changes in ED utilization, the study period was divided into 3 phases according to national COVID-19 social distancing policies implemented in South Korea. The predistancing period was defined as January 1, 2019, to March 21, 2020, representing baseline patterns before the introduction of nationwide social distancing measures. The during-distancing period spanned from March 22, 2020, to April 17, 2022, corresponding to sustained government-mandated social distancing and public health interventions. The postdistancing period was defined as April 18, 2022, to December 31, 2023, following the formal lifting of social distancing policies. These period definitions were applied uniformly across all analyses to facilitate comparisons of ED visit patterns between pediatric and adult patients.
4. Infectious pathogen surveillance data
To examine temporal associations between ED visits for abnormal LFTs and circulating infectious pathogens, national infectious disease surveillance data provided by the Korea Disease Control and Prevention Agency (KDCA) were used. ED visit data from NEDIS and pathogen surveillance data from KDCA were analyzed independently at the population level and were not linked at the individual patient level. This surveillance system compiles weekly aggregated reports from designated sentinel institutions across South Korea and monitors community-level circulation of respiratory and enteric pathogens. Respiratory pathogens included rhinovirus, adenovirus, parainfluenza virus, human bocavirus, human metapneumovirus, respiratory syncytial virus, influenza virus, and human coronavirus. Enteric pathogens comprised enteric viruses (astrovirus, sapovirus, norovirus, and rotavirus) and enteric bacteria, including enteropathogenic Escherichia coli (EPEC) and enterotoxigenic Escherichia coli (ETEC).
To analyze population-level temporal relationships between the 2 independent datasets, we performed temporal alignment using contemporaneous weekly data from both NEDIS and KDCA. This approach enabled assessment of temporal correlations between ED visit trends and community-level pathogen circulation patterns, without establishing individual-level linkage. Detailed characteristics of the KDCA surveillance system, including annual sentinel institution numbers, and pathogen case counts, are provided in Supplementary Table 1.
5. Statistical analysis
Descriptive statistics were used to summarize patient characteristics, presenting symptoms, concurrent diagnoses, and disposition outcomes. Categorical variables were reported as frequencies and percentages and were compared between pediatric and adult patients using chi-square tests, as appropriate. Temporal changes in ED visit volumes for abnormal LFTs across COVID-19 periods were evaluated using negative binomial generalized additive models with cyclic splines to account for seasonal patterns and overdispersion in count data. Rate ratios with 95% confidence intervals (CIs) were calculated to compare visit volumes between the predistancing, during-distancing, and postdistancing periods. Analyses were performed separately for pediatric and adult patients. For pairwise comparisons between COVID-19 periods, P values were adjusted using the Bonferroni correction for multiple testing.
Associations between ED visit trends and infectious pathogens were assessed by comparing weekly ED visit counts with weekly pathogen detection counts. Correlation analyses were conducted using Spearman rank correlation coefficients to evaluate population-level associations, and were performed separately for pediatric and adult patients. All statistical analyses were conducted using R ver. 4.4.3 (R Foundation for Statistical Computing, Austria). A 2-sided P value<0.05 was considered statistically significant.
6. Ethical considerations
This study was approved by the institutional review board of Seoul National University Hospital (E-2507-044-1656). The requirement for informed consent was waived due to the retrospective nature of the study and use of deidentified data.
Results
1. Clinical characteristics of patients presenting with abnormal LFTs
Between January 2019 and December 2023, a total of 26,874 ED visits for abnormal LFTs were identified nationwide. Of these, 3,152 visits (11.7%) occurred in pediatric patients aged 0–18 years, while 23,722 visits (88.3%) involved adult patients aged 19–64 years (Fig. 1). Pediatric ED visits remained relatively stable across all age subgroups, while adult visits demonstrated a progressive increase with advancing age, with the most pronounced rise observed in older adult age groups. Pediatric patients demonstrated a male predominance (61.1%), whereas adult patients showed a more balanced sex distribution (54.6%) (P<0.001) (Table 1). Pediatric patients also more frequently presented with high-acuity conditions, with 21.1% classified as KTAS 1–2, compared with 6.4% among adults. Overall admission rates were higher in pediatric patients (72.4%) than in adults (53.3%). Despite this higher initial acuity and admission rate, pediatric patients required intensive care less frequently than adults (1.8% vs. 5.2%). Adults were more likely to be discharged directly from the ED (44.9% vs. 26.7%).
Age distribution of Emergency Department visits for abnormal liver function tests, 2019–2023. Bar graph showing the number of Emergency Department (ED) visits by age. The green bars represent pediatric patients (0–18 years), while the orange bars represent adult patients (19–64 years).
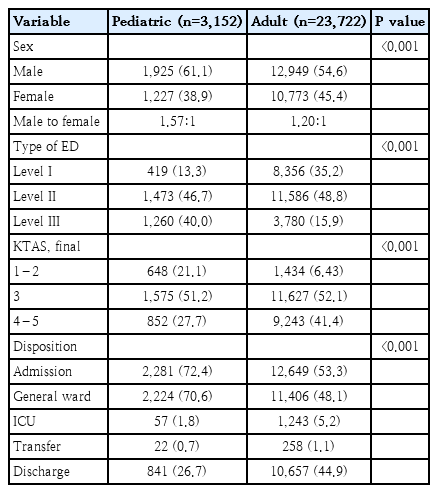
Clinical outcomes of patients with abnormal liver function tests presenting to the Emergency Department
2. Presenting symptoms and distribution of concurrent diagnoses in patients with abnormal LFTs
Presenting symptoms at ED presentation differed substantially between pediatric and adult patients (Table 2). Fever was the predominant symptom among pediatric patients, observed in 47.3% of cases and occurring more than 3 times as frequently as in adults (13.9%). Respiratory symptoms were also more common in pediatric patients (6.4% vs. 4.0%). In contrast, adult patients more frequently presented with abdominal pain (26.4% vs. 14.2%) and systemic symptoms, including dizziness, myalgia, chest pain, and asthenia. Gastrointestinal symptoms such as nausea, vomiting, and diarrhea were observed at comparable frequencies in pediatric and adult patients. The distribution of concurrent diagnoses by ICD-10 diagnostic chapters showed marked differences between the 2 groups (Fig. 2). Adult patients demonstrated higher proportions of endocrine/metabolic disorders (16.4%), circulatory diseases (12.4%), and genitourinary disorders (11.8%) compared to pediatric patients, while pediatric patients showed higher rates of infectious disease diagnoses (39.8% vs. 22.4%).
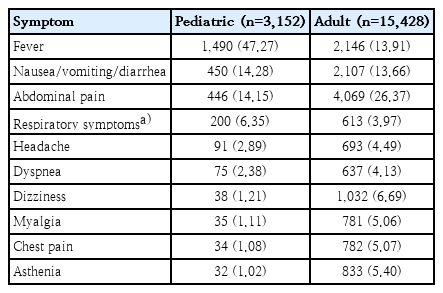
Presenting symptoms of patients with abnormal liver function tests presenting to the Emergency Department
Concurrent diagnoses among pediatric and adult patients visiting the Emergency Department for abnormal liver function tests. Horizontal bar chart comparing the proportion of International Classification of Diseases, Tenth Revision, diagnostic categories between pediatric (0–18 years, shown in green) and adult (19–64 years, shown in orange) patients.
Specific disease patterns differed markedly between groups (Supplementary Table 2). Pediatric presentations featured predominantly infectious etiologies including gastroenteritis (15.8%), unspecified viral infections (6.9%), acute bronchitis (4.5%), sepsis (4.3%), and acute viral hepatitis (4.2%). Respiratory viral syndromes including bronchiolitis (3.4%), influenza (2.3%), and viral pneumonia (1.5%) were common, alongside infectious mononucleosis (2.4%) and cytomegaloviral disease (1.7%). Hematologic conditions were prominent, with agranulocytosis occurring in 10.7% and lymphoid leukemia in 6.4% of cases. In contrast, adult patients demonstrated infectious gastroenteritis as the most frequent concurrent diagnosis (20.9%), followed by gastritis (18.3%) and gastroesophageal reflux disease (9.2%). Conditions associated with metabolic syndrome and MASLD were common, including disorders of lipoprotein metabolism (7.9%), hypertension (7.8%), and type 2 diabetes mellitus (6.0%). Liver-specific conditions included alcoholic liver disease (5.1%), other inflammatory liver diseases (4.5%), and acute pancreatitis (3.7%), with viral hepatitis occurring in 3.4% of cases. Overall, pediatric patients exhibited fever-predominant acute respiratory viral infection profiles, while adult patients showed infectious gastroenteritis, upper gastrointestinal disorders, and clustering of cardiometabolic risk factors consistent with metabolic syndrome.
3. Changes in ED visit volume during the COVID-19 period
Given that COVID-19 social distancing measures substantially altered infectious disease epidemiology, ED visit volumes for abnormal LFTs changed differently between pediatric and adult patients across the COVID-19 pandemic periods (Table 3). Among pediatric patients, visit volumes showed nonsignificant declines during the social distancing period and in the postdistancing period compared with the predistancing period. In contrast, adult patients demonstrated a distinct pattern. While visit volumes showed no significant change during the distancing period compared with the predistancing period, visits significantly increased in the postdistancing period compared with the during-distancing period (rate ratio [during/post], 0.82, 95% CI 0.71–0.95; P=0.004). These findings indicate divergent age-dependent changes in ED utilization for abnormal LFTs during and after the COVID-19 pandemic.
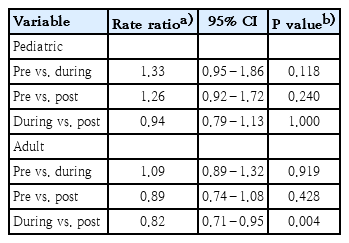
Pairwise comparisons of ED visit rates between intervention periods
4. Temporal trends and pathogen associations of abnormal LFT-related visits
To further explore potential factors underlying the divergent changes in ED visit volumes, we examined population-level temporal patterns of visits for abnormal LFTs in relation to infectious pathogen surveillance data (Fig. 3A). In pediatric patients, visit trends showed close temporal alignment with respiratory viral activity, particularly rhinovirus and adenovirus, which exhibited pronounced seasonal fluctuations during the prepandemic period and altered patterns thereafter. Other respiratory viruses, including parainfluenza virus and human bocavirus, demonstrated episodic increases corresponding to pediatric visit peaks. In contrast, adult patients showed temporal patterns that more closely paralleled enteric pathogens. Increases in visits were temporally associated with enteric viruses such as astrovirus and sapovirus, as well as enteric bacterial pathogens including EPEC and ETEC, particularly during the postdistancing period. These population-level temporal patterns were subsequently quantified through correlation analyses (NEDIS-KDCA correlation).
Temporal trends and inter-pathogen correlations during the COVID-19 pandemic. (A) Weekly number of Emergency Department (ED) visits by pediatric versus adult population (top 2 panels) and national pathogen detection trends (lower panels) across 3 periods: Predistancing (January 1, 2019 to March 21, 2020), Duringdistancing (March 22, 2020 to April 17, 2022), and postdistancing (April 18, 2022 to December 31, 2023). (B) Spearman correlation matrices of ED visits and pathogen detections in pediatric (upper) and adult (lower) populations. Circle size represents correlation strength (r); color indicates direction (red: positive; blue: negative). ADV, adenovirus; AstV, astrovirus; COVID-19, coronavirus disease 2019; EPEC, enteropathogenic Escherichia coli; ETEC, enterotoxigenic Escherichia coli; EV, enterovirus; Flu, influenza virus; HBoV, human bocavirus; HCoV, human coronavirus; hMPV, human metapneumovirus; NoV, norovirus; PIV, parainfluenza virus; RHV, rhinovirus; RSV, respiratory syncytial virus; RV, rotavirus; SaV, sapovirus
Population-level correlation analyses highlighted age-specific pathogen associations (Fig. 3B, NEDIS-KDCA correlation). Pediatric visits were positively correlated with respiratory viruses, most notably rhinovirus (r=0.30, P<0.001), adenovirus (r=0.28, P<0.001), and parainfluenza virus (r=0.25, P<0.001), whereas correlations with enteric pathogens were weak or nonsignificant. Conversely, adult visits demonstrated stronger positive correlations with enteric viruses, including astrovirus (r=0.35, P<0.001) and sapovirus (r=0.32, P<0.001), as well as enteric bacteria such as EPEC (r=0.38, P<0.001) and ETEC (r=0.36, P<0.001). These temporal correlation patterns at the population level indicate age-specific pathogen profiles, characterized by predominant alignment with respiratory viruses in pediatric patients and with enteric pathogens in adult patients.
Discussion
In this nationwide cohort study of 26,874 ED visits for abnormal LFTs, we identified distinct age-dependent phenotypes with divergent population-level pathogen associations. While pediatric presentations showed temporal alignment with acute respiratory viral infections, adult presentations demonstrated previously unreported population-level associations with enteric pathogens, coupled with infectious gastroenteritis and clustering of metabolic comorbidities. These findings challenge the perception that abnormal LFTs in emergency settings follow predictable age-dependent patterns and provide evidence for pathogen-specific etiologic profiles warranting mechanistic validation.
Pediatric patients predominantly presented with acute infectious profiles, characterized by fever (47.3%) and infectious disease diagnoses (39.8%), consistent with transient hepatic involvement during systemic viral infections. Strong temporal correlations with respiratory viruses, particularly rhinovirus (r=0.30) and adenovirus (r=0.28), align with Korean and international observations showing that viral respiratory tract infections account for the majority of abnormal liver function in children [7,8,10,11].
Following reports of acute severe hepatitis of unknown etiology in children across multiple countries in 2022, which prompted international alerts due to high rates of liver transplantation (approximately 5%–10%) [18-20], subsequent investigations identified adeno-associated virus 2 coinfection with helper viruses as a potential mechanism in severe cases [21,22]. However, Korean surveillance during the same period confirmed that adenovirus detection rates remained stable and that adenovirus-positive children consistently showed favorable outcomes without progression to acute liver failure or transplantation [10], supporting the typically benign nature of viral hepatic involvement in most pediatric presentations. Despite higher initial triage acuity (KTAS 1-2: 21.1%) and high admission rates (72.4%) in our cohort, intensive care utilization remained low (1.8%), and most children showed rapid recovery with median normalization times of 13–16 days for viral infections [7], indicating that admissions often reflect clinical caution rather than disease severity. The observed male predominance (61.1%) may reflect sex-based differences in immune responses to viral infections [23].
In contrast, adult presentations revealed unexpected population-level associations between abnormal LFTs and enteric pathogens. Strong correlations were observed with astrovirus, sapovirus, EPEC, and ETEC. While these pathogens are well-established causes of acute gastroenteritis [24], their potential role in hepatic involvement has received limited attention. Recent metagenomic studies have identified sapovirus and astrovirus in serum from patients with hepatitis of unknown etiology [25], and isolated case reports have described norovirus-associated transient liver dysfunction in adults [26], but population-level epidemiologic evidence has been lacking. The observed population-level temporal associations between enteric pathogens and abnormal LFTs in adults warrant mechanistic investigation. The concurrent high prevalence of metabolic comorbidities, including dyslipidemia (7.9%), hypertension (7.8%), and diabetes (6.0%), suggests that metabolic syndrome and MASLD may constitute underlying susceptibility factors. Whether adults with preexisting hepatic steatosis exhibit enhanced vulnerability to enteric pathogen-related hepatic inflammation requires validation through individual-level studies.
The divergent responses to COVID-19 social distancing between age groups provide additional evidence for distinct etiologic profiles. While pediatric visits remained stable across pandemic periods, adult visits significantly increased following relaxation of distancing measures (rate ratio, 0.82; P=0.004). This pattern temporally coincided with resurgence of enteric pathogen circulation and contrasts with the respiratory virus-driven fluctuations observed in pediatric populations, underscoring fundamental differences in the infectious epidemiology underlying abnormal LFTs across age groups.
Several limitations should be acknowledged. First, the use of ICD-10 code R94.5 identifies ED visits in which abnormal LFTs constituted a clinically significant concern but does not provide quantitative laboratory data or severity grading. Second, concurrent diagnoses recorded in administrative data cannot establish causal relationships with liver function abnormalities. Third, and most importantly, the observed associations between ED visits and infectious pathogens reflect population-level temporal correlations rather than individual-level causal relationships. ED visit data from NEDIS and pathogen surveillance data from KDCA were analyzed independently and were not linked at the individual patient level. Therefore, these patterns may indicate direct pathogen-related hepatic involvement, or may reflect concurrent presentations in patients with preexisting conditions or other confounding factors. The ecological correlation design, while revealing distinct age-specific temporal pathogen profiles, cannot establish individual-level causality. Individual-level linkage studies with laboratory-confirmed pathogen testing and concurrent liver function measurements are needed to establish causal mechanisms. Finally, multiple pandemic-related factors, including changes in healthcare access and behavior, limit causal interpretation of observed temporal trends. The findings reflect the healthcare context of South Korea and may not be directly generalizable to other settings.
In conclusion, ED presentations for abnormal LFTs demonstrate distinct age-dependent phenotypes with divergent temporal pathogen associations: respiratory viral infections predominate in children, while enteric pathogens show previously unreported population-level associations in adults with concurrent metabolic comorbidities. These findings support age-stratified diagnostic approaches and highlight enteric pathogen-associated hepatic involvement as an area warranting mechanistic investigation.
Supplementary materials
Supplementary Table 1-2 are available at https://doi.org/10.3345/cep.2026.00038.
Annual number of sentinel institutions and reported cases of respiratory and gastrointestinal infections (2019–2023)
Top 10 concurrent diagnoses by ICD-10 (International Classification of Diseases, 10th Revision) chapter among pediatric and adult patients with abnormal liver function tests presenting to the Emergency Department
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgments
The authors acknowledge the use of Claude Sonnet 4.5 (Anthropic) for language refinement and manuscript formatting assistance. All AI-generated content was thoroughly reviewed, edited, and verified by the authors, who take full responsibility for the integrity of the manuscript.
Author contribution
Conceptualization: DUK, SC, JSK; Data curation: DUK, SC; Formal analysis: DUK, SC; Methodology: DUK, SC, JSK; Project administration: JSK; Visualization: DUK; Writing - original draft: DUK, SC; Writing - review and editing: YK, LK, JOS, JSM, JWH, HRY, JYC, JSK; Investigation: DUK, SC, YK, LK, JOS, JSM, JWH, HRY, JYC; Supervision: JSK; Validation: DUK, SC