Overlapping Guillain-Barré syndrome and Bickerstaff's brainstem encephalitis associated with Epstein Barr virus
Article information
Abstract
A flaccid tetraparesis in Bickerstaff's brainstem encephalitis (BBE) is presumed to be a sign of overlapping Guillain-Barré syndrome (GBS). In addition, BBE and Fisher syndrome, which are clinically similar and are both associated with the presence of the immunoglobulin G anti-GQ1b antibody, represent a specific autoimmune disease with a wide spectrum of symptoms that include ophthalmoplegia and ataxia. A 2-year-old boy presented with rapidly progressive ophthalmoplegia, ataxia, hyporeflexia, weakness of the lower extremities, and, subsequently, disturbance of consciousness. He experienced bronchitis with watery diarrhea and had laboratory evidence of recent infection with Epstein-Barr virus (EBV). He was diagnosed as having overlapping GBS and BBE associated with EBV and received treatment with a combination of immunoglobulin and methylprednisolone, as well as acyclovir, and had recovered completely after 3 months. In addition, he has not experienced any relapse over the past year. We suggest that combinations of symptoms and signs of central lesions (disturbance of consciousness) and peripheral lesions (ophthalmoplegia, facial weakness, limb weakness, and areflexia) are supportive of a diagnosis of overlapping GBS and BBE and can be helpful in achieving an early diagnosis, as well as for the administration of appropriate treatments.
Introduction
Bickerstaff's brainstem encephalitis (BBE) is a rare immune disorder in children. BBE is characterized by progressive ophthalmoplegia, ataxia, disturbance of consciousness, pyramidal signs, extensor plantar responses, and long track sensory disturbance1). Limb weakness in patients with BBE was considered the result of overlapping with the axonal subtype of Guillain-Barré syndrome (GBS)1,2). Although the etiology of BBE is unknown, it has been linked to various antecedent infections, such as Campylobacter jejuni, Cytomegalovirus (CMV), Varicellar zoster virus, Epstein Barr virus (EBV), and Mycoplasma pneumoniae1,3,4,5,6).
In overlapping cases, such as Miller Fisher syndrome (MFS) and GBS, the clinical features may cause confusion so that a correct diagnosis of BBE is difficult. Presence of antiganglioside antibodies (GQ, GM, and GD) in serum or CSF is informative for the diagnosis of BBE. Here, we describe a patient with overlapping GBS and BBE associated with EBV who recovered completely without relapse by treatment with a combination of immunoglobulin (Ig) and methylprednisolone as well as acyclovir. This case supports the hypothesized continuity between GBS and BBE.
Case report
A 2-year-old boy was referred to Chosun University Hospital with symptoms of ophthamoplegia, walking disturbance, and irritability. He had suffered from acute bronchitis and enteritis three weeks before admission.
On admission, the vital signs were body temperature of 36.5℃, pulse rate of 121 beats/min, and blood pressure of 100/60 mmHg. Mild abdominal distention was observed. The pupils were 4 mm bilaterally and light reflexes were intact. He was alert, with no other abnormal neurological findings except for ptosis and ophthalmoplegia (restriction of lateral gaze of both eyes). The muscle strength of his lower extremities was grade 2. Deep tendon reflexes of his lower extremities were absent, but sensation was intact. No signs of meningeal irritation were observed during admission. By the following day, he had become confused, had dysphasia, and had bilateral facial palsy. Treatment with intravenous immunoglobulin (IVIG) (0.4 g/kg/day for five days) was started. On the third day of admission, he developed difficult respiration. Muscle strength of his upper extremities was decreased to grade 2, and that of his lower extremities was decreased to grade 0. Treatment with a high dose of methylprednisolone (30 mg/kg for three days) was started. On the fourth day of admission, self respiration was absent. The patient's consciousness level worsened to a coma state. Pupil size decreased (2 mm/2 mm), and there were no light reflexes. His blood pressure and pulse rate had increased (120/80 mmHg, 200 beats/min, respectively). An angiotensin converting enzyme inhibitor was started for management of hypertension. He required assisted ventilation until day 19 due to respiratory failure.
White blood count (13,500/µL) mildly increased. Hemoglobin, platelet count, routine chemistries, liver function profile, ammonia, electrolytes, erythrocyte sedimentation rate, and cerebrospinal fluid (CSF) examination were within reference ranges. Blood tests for recent infection by CMV and the influenza virus were negative. The results of serum antibody testing for Mycoplasma, C. jejuni were negative. The result of a repeat CSF examination on day 3 was normal: pressure, 12 cmH2O; leukocytes, 4/µL; red blood cell, 1/µL; protein, 33.5 mg/dL; glucose, 65.3 mg/dL. The myelin basic protein and oligoclonal bands were normal. A specific polymerase chain reaction (PCR) examination of the CSF was negative for the Herpes virus group or for an Enterovirus infection. Serum and CSF antiganglioside antibodies, which were measured using an enzyme-linked immunoadsorbent assay, showed an absence of anti-GQ1b IgG and IgM antibodies, anti-GM1 IgG and IgM antibodies, and anti-GD1 IgG and IgM antibodies. A CSF analysis on day 5 showed a protein concentration of 54 mg/dL without leukocyte. A positive result was obtained for EBV viral capsid and antigen-IgG and IgM antibodies and EBV confirmed seroconversion of the nuclear antigen antibody. EBV-DNA was detected in the CSF by PCR. These findings indicate prior infection by EBV.
Brain and spine magnetic resonance images (MRIs) performed on the fourth and 13th days detected no abnormal signals in either the cerebrum or brainstem (Fig. 1). An electroencephalogram (EEG) without sedative drugs showed slow wave bursts at both occipital lobes (Fig. 2). Nerve conduction and electromyogram studies were not performed. Acyclovir was started for more effective treatment of EBV infection.
Brain magnetic resonance imaging (MRI) (A) and spine MRI (B) revealed no abnormalities.
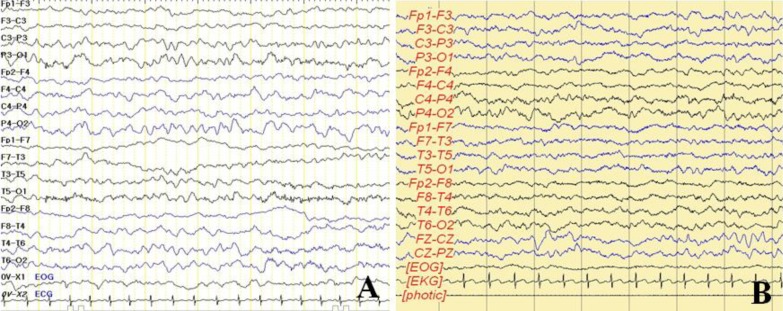
Electroencephalogram showed slow wave activity in the theta to delta range in both occipital areas at 4 days after admission (A) but showed no abnormalities at 23 days after admission (B).
By the final day of treatment, the patient's mental status, blood pressure, and pulse rate were normal. Facial palsy, ptosis, ophthalmoplegia, dysarthria, and deep tendon reflex showed improvement. Muscle strength remained impaired and he exhibited a slight stagger while walking. Three months after the beginning of his neurological disease, he had almost completely recovered. One year after treatment, he had fully recovered without relapse.
Discussion
BBE is a rare immune disorder in children, which was first described by Bickerstaff and Cloake7) in 1951. The clinical features and course of the condition, the associated auto-antibodies against relevant antigens, and the response to treatment all suggest that Bickerstaff's encephalitis is an autoimmune disease.
Like some other autoimmune diseases, the condition usually follows a minor infection, such as a respiratory tract infection or gastroenteritis. An immunological mechanism induced by infection could potentially play a pathogenic role in BBE3). A previous infectious disease is frequently reported before the appearance of neurological symptoms, which might be suggestive of an infectious etiology1). Our case was associated with EBV infection.
Major manifestations of BBE associated with facial and bulbar weakness, and a flaccid tetraparesis include acute ophthalmoplegia, ataxia, and disturbance of consciousness. After opthalmoplegia, facial weakness is more common than bulbar palsy. Involvement of respiratory muscles is rare and recovery is usually complete. Therefore, it is important to provide ventilation for all patients. BBE with limb weakness was considered the result of overlapping with the axonal subtype of GBS1). BBE and MFS are similar clinically and are associated with presence of the IgG anti-GQ1b antibody, representing a specific autoimmune disease with a wide spectrum of symptoms, including ophthalmoplegia and ataxia8). There is certainly an overlap between GBS, MFS, and BBE, as well as other conditions associated with antiganglioside antibodies, such as chronic ophthalmoplegia with the anti-GQ1b antibody9).
A variety of CSF abnormalities with albumino-cytologic dissociation occur late in the illness in one third or more patients. Cumulative evidence has suggested a causal relationship between BBE, GBS, and Fisher Syndrome, and CSF albumino-cytologic dissociations are often being detected in all of them4). CSF albumino-cytologic dissociation was found in 19% of cases of BBE during the first week after the beginning of the illness1). The CSF protein concentration showed a progressive increase after the fourth week. In our case, CSF was normal during the six days after the beginning of illness, after that, CSF albumino-cytologic dissociation was detected.
The EEG is often abnormal but shows only slow wave activity, which also occurs in many other conditions, and is therefore of limited value in diagnosis. High intensity T2-weighted abnormalities of the brainstem or other parts of the central nervous system are observed on brain MRI in 30% of patients1). Cerebral imaging is rarely useful for the diagnosis of BBE. Abnormal findings on MRI brain scans were reported in 39% of cases of BBE without limb weakness and in 23% of cases of BBE with limb weakness10).
In patients with BBE with coexisting limb weakness, decreased motor nerve conduction velocities, prolonged distal latency, reduced compound muscle action potential amplitude, disappearance of F-wave or its prolonged latency, which is indicative of motor nerve demyelination and axon degeneration can be observed on an electromyogram. The somatosensory evoked potentials for early diagnosis are useful and may be more severely impaired than auditory brainstem responses in BBE11).
There is no single diagnostic test which can diagnose BBE. Due to its diverse symptoms, early diagnosis is often difficult. Early diagnosis is important not only for the performance of effective immunotherapies but also for the avoidance of unnecessary evaluation testing and treatment, such as antiviral or antithrombotic agents. However, the diagnosis of BBE is still based on clinical criteria. The presence of anti-GQ1b antibodies and an abnormal brain MRI can help to support its diagnosis. However, the absence of anti-GQ1b antibodies and a normal brain MRI do not exclude the diagnosis.
Our patient was initially diagnosed with MFS and then diagnosed with overlapping GBS and BBE with specific clinical symptoms, including impaired consciousness and limb weakness, and CSF findings, although other tests which might be helpful for the diagnosis of BBE, such as anti-GQ1b antibodies and a brain MRI were normal.
IVIG is effective in immune-mediated disorders such as MFS and GBS12). IVIG is also effective in treatment of BBE with hypothesized immune-mediated etiology, which is similar to the clinical and immunologic features of MFS or GBS, which suggests an overlapping spectrum of MFS and GBS. The therapeutic effect of IVIG (total dose of 2 g/kg given over two days) is related to the neutralization of pathogenic autoantibodies such as anti-GQ1b antibodies13). BBE and GBS are so closely related that combined therapy of IVIG and high-dose methylprednisolone is a more efficacious therapy than IVIG alone. The prognosis was good, with most patients making a full clinical recovery over six months. Cases of recurrent BBE have been reported. IVIG was initially chosen for our patient because of similar symptoms of MFS or GBS. On the third hospital day, methylprednisolone was started because IVIG was ineffective and his mental state showed greater impairment. On the fifth hospital day, acyclovir was started because of a positive result for EBV in serum and CSF which is based on a previous report3). Clinical responses to treatment were observed on the 23rd day, similar to a previous report14), and he recovered completely without recurrence.
We think that our patient was overlapping GBS and BBE following EBV with specific clinical symptoms: progressive opthalmoplegia; ataxia; disturbance of consciousness; progressive bilateral limb weakness; facial weakness; urinary retention and hypertension. We suggest that combinations of symptoms and signs of central lesions (disturbance of consciousness) and peripheral lesions (ophthalmoplegia, facial weakness, limb weakness, and areflexia) are supportive of a diagnosis of overlapping GBS and BBE and can be helpful in achievement of an early diagnosis and for administration of appropriate treatment.
Notes
No potential conflict of interest relevant to this article was reported.