Telomere biology disorders associated with childhood interstitial lung disease
Article information
 , Christina Katharina Rapp, PhD2, Katrin Knoflach, MD2, Daniel Gräfe, MD3, Franz Wolfgang Hirsch, MD3, Julia Ley-Zaporozhan, MD2, Simone Reu-Hofer, MD4, Julia Hentschel, MD5, Stefan Zielen, MD6, Monika Helena Tedy, MD7, Heymut Omran, MD, PhD7, Ernst Rietschel, MD8, Tuğba Sismanlar Eyuboglu, MD9, Ayse Tana-Aslan, MD9, Nagehan Emiralioglu, MD10, Nicola Ullmann, MD11, Samuele Naviglio, MD12, Massimo Maschio, MD12, Fabian Beier, MD13,14, Tuğba Ramaslı Gürsoy, MD15, Matthias Griese, MD,2, Freerk Prenzel, MD,1
, Christina Katharina Rapp, PhD2, Katrin Knoflach, MD2, Daniel Gräfe, MD3, Franz Wolfgang Hirsch, MD3, Julia Ley-Zaporozhan, MD2, Simone Reu-Hofer, MD4, Julia Hentschel, MD5, Stefan Zielen, MD6, Monika Helena Tedy, MD7, Heymut Omran, MD, PhD7, Ernst Rietschel, MD8, Tuğba Sismanlar Eyuboglu, MD9, Ayse Tana-Aslan, MD9, Nagehan Emiralioglu, MD10, Nicola Ullmann, MD11, Samuele Naviglio, MD12, Massimo Maschio, MD12, Fabian Beier, MD13,14, Tuğba Ramaslı Gürsoy, MD15, Matthias Griese, MD,2, Freerk Prenzel, MD,1
Abstract
Background
Telomere biology disorders (TBDs) are rare inherited defects in telomere maintenance associated with multisystem diseases. Although pulmonary fibrosis has been well described in adults, data remain limited on childhood interstitial lung disease (chILD) related to TBDs.
Purpose
This study aimed to characterize the pulmonary phenotype, genetic spectrum, and clinical course of pediatric TBD-associated chILD.
Methods
We performed this registry-based cohort study using the European chILD-EU database to identify children with telomere maintenance gene variants. Their clinical data, longitudinal outcomes, telomere length (quantitative polymerase chain reaction), high-resolution computed tomography (HRCT), and histopathology findings were systematically analyzed.
Results
Ten children were identified with genetically confirmed or suspected TBDs harboring variants in TERT, TERC, WRAP53, DKC1, PARN, and RTEL1. Telomere length was below the 1st age-adjusted percentile in 6 of the 8 tested patients. The HRCT findings were heterogeneous and included ground-glass opacities, reticular changes, cystic lesions, and emphysema. The histopathological patterns included cellular nonspecific interstitial pneumonia, usual interstitial pneumonia, follicular bronchiolitis, and pleuroparenchymal fibrosis. The disease course was frequently severe: 7 of the 10 patients required long-term oxygen therapy, 3 underwent hematopoietic stem cell transplantation, and 4 died during follow-up.
Conclusion
TBD-associated chILD is a rare but clinically aggressive multisystem disorder with a broad radiological and histopathological spectrum. Early genetic testing and multidisciplinary management are essential since affected children may experience rapid disease progression and substantial mortality.
Key message
Question: What are the pulmonary manifestations and clinical characteristics of telomere biology disorders in children with interstitial lung disease?
Finding: Telomere biology disorders are an important but often underrecognized cause of childhood interstitial lung disease and are associated with variable pulmonary, radiologic, and histopathologic findings, frequent multisystem involvement, and often severe disease progression.
Meaning: Early genetic testing and multidisciplinary evaluation are essential for timely diagnosis, optimized management, and improved outcomes in affected children.
Graphical abstract. ILD, interstitial lung disease; DKC, dyskeratosis congenita.
Introduction
Childhood interstitial lung disease (chILD) comprises over 200 rare and heterogeneous pulmonary conditions, with a reported prevalence of 44–46 cases per million children [1,2]. Telomere shortening has been identified in adult studies and in rare pediatric case reports as a contributing factor in interstitial lung disease (ILD) [3,4].
Telomeres, which consist of noncoding tandem DNA repeats (TTAGGG in humans), serve a protective function at the ends of chromosomes, preventing degradation and fusion with other chromosomes. In humans, telomere length ranges from 5–15 kilobases and progressively shortens during mitosis. When telomeres become shortened to a critical length, a nonreplicative state known as cellular senescence occurs, which can lead to apoptosis in certain cell types [5,6]. Telomerase protects telomeres from damage and shortening and is active during embryogenesis as well as in rapidly proliferating adult tissues, such as hematopoietic stem cells and immune cells. Similarly, the bronchoalveolar epithelium is continuously regenerated by progenitor cells known as alveolar epithelial type II cells, whose replicative capacity is limited by telomere length and who therefore play a key role in the development of fibrotic lung disease [7-9]. The telomerase complex consists of the telomerase reverse transcriptase (encoded by TERT) and the noncoding telomerase RNA (encoded by TERC), and it binds to the ends of telomeres. The telomerase RNA provides the template for the synthesis of telomeric nucleotide repeats, while telomerase reverse transcriptase serves as the rate-limiting catalytic subunit of the telomerase complex. Other essential components involved in telomere maintenance include the shelterin complex (composed of the 6 proteins: TRF1, TRF2, RAP1, TIN2, POT1, and TPP1), which protects the telomeric DNA repeats; dyskerin (encoded by DKC1), a nucleolar protein that plays a critical role in the assembly and activity of the telomerase complex; Poly(A)-specific ribonuclease (encoded by PARN), which is involved in the maturation and stabilization of TERC; telomerase Cajal body protein 1 (encoded by WRAP53) is involved in the trafficking and localization of TERC, playing a crucial role in telomerase assembly and telomere maintenance. Another important role has the regulator of telomere elongation helicase 1 (encoded by RTEL1), which prevents telomere fragility and inappropriate recombination [10-12].
Telomere biology disorders (TBD) are a group of diseases caused by genetic variants in components of the telomerase complex, characterized by abnormally short telomeres and an annual telomere loss exceeding 120 base pairs, compared to the normal rate of approximately 60 base pairs. Telomere lengths are generally below the first age-adjusted percentile in TBDs, but they are not the only factor contributing to differences in disease severity among subtypes [13-19]. Telomere damage and dysfunction can lead to a broad spectrum of phenotypes, ranging from complex multisystem disorders such as dyskeratosis congenita (DKC), Hoyeraal-Hreidarsson syndrome, Revesz syndrome, and Coats-plus syndrome to pulmonary fibrosis, bone marrow failure, and liver disease. DKC is a rare pediatric multisystem disorder (prevalence: approximately 1 in 1 million) characterized by a mucocutaneous triad: leukoplakia, lacy reticular skin pigmentation, and dystrophic nails.
To date, pathogenic variants in the following genes have been shown to cause TBDs and result in critically short telomeres: ACD, CTC1, DKC1, NAF1, NHP2, NOP10, PARN, POT1, RPA1, RTEL1, STN1, TERC, TERT, TINF2, WRAP53, and ZCCHC8. Variants in these genes can be inherited in an X-linked, autosomal dominant, or autosomal recessive manner, or may occur de novo. They often exhibit incomplete penetrance, and those diseases tend to follow a pattern of anticipation–with increasing severity and earlier onset in successive generations [20-28].
Critical telomere shortening in alveolar stem cells induces profibrotic signaling, inflammation with infiltration of innate immune cells, and increased expression of transforming growth factor-beta. Pulmonary fibrosis subsequently develops because of excessive myofibroblast accumulation.
In adult cohorts with idiopathic pulmonary fibrosis (IPF), pathogenic variants in TERT have been identified in up to 15% of families with familial pulmonary fibrosis and in 1%–3% of sporadic cases. Evidence in the pediatric population remains scarce and is primarily based on isolated case reports [3,9,29,30]. TBD-associated children's ILD represents a subgroup of chILD characterized by a fibrosing phenotype, which is associated with progressive disease, increased symptom burden, higher morbidity, and declining lung function [31]. Currently, no curative therapy is available. To date, symptomatic treatment approaches have included corticosteroids, antibiotics, androgens, antifibrotic agents, and lung transplantation [32-39]. The use of systemic corticosteroids remains controversial, as data from adult studies suggest that immunosuppressive therapy may be associated with increased mortality in patients with telomere-related ILD. Therefore, treatment decisions should be made cautiously and individualized, particularly in pediatric patients with suspected or confirmed TBDs.
Given the limited treatment options for this progressive disease, it is essential to generate more evidence on genetic mutations, patterns of manifestation, and clinical course in children. Therefore, the aim of this study was to characterize this rare condition using data from the European Children's Lung Registry, chILD-EU [40].
Methods
This cohort study investigated a group of patients with ILD who carried genetic variants in genes associated with TBDs. To identify the patients, we searched the database of the chILD-EU registry including August 2025. The registry (www.childeu.net) is an observational, web-based platform that prospectively collects clinical data on children diagnosed with chILD across multiple international centers. It includes patients with suspected or confirmed ILD from approximately 20 participating countries in Europe and beyond. The registry captures detailed information on clinical presentation, radiologic findings, histopathology, genetic data, treatment, and longitudinal outcomes. All cases are reviewed by a multidisciplinary expert panel including pediatric pulmonologists, radiologists, pathologists, and geneticists.
1. Ethics
The study was approved by the Ethics Committee of the Ludwig Maximilian University of Munich (approval numbers: EK 23-5-2011, EK 111-13, 20-329). Written informed consent was obtained from all patients or their legal guardians who participated in the study. Additionally, written informed consent for the publication of individual patient data was obtained from all patients who were old enough to provide consent, as well as from their parents or legal guardians.
2. Availability of data and materials
The datasets supporting the conclusions of this article are available within the article and Supplementary Table 1.
3. Telomere length measurement
Telomere length was measured in patients for whom a sufficient ethylenediaminetetraacetic acid blood sample was available in the registry's biobank. Genomic DNA was extracted from leukocytes, and telomere length was determined using the quantitative polymerase chain reaction (PCR) assay developed by Cawthon [41]. This method provides an estimate of average telomere length across leukocyte populations and does not allow differentiation between specific cell subtypes.
4. Radiology
High-resolution computed tomography (HRCT) was centrally peer reviewed by agreement of 2 specialized pediatric radiologists based on the recommendations of the Fleischner Society [42]. HRCT examinations were performed at the time of initial clinical evaluation and, where available, during follow-up. We present selected images from diagnostic examinations demonstrating disease-related abnormalities.
5. Histopathology
All lung biopsies were analyzed by a local pathologist prior to inclusion in the chILD-EU and re-evaluated centrally for the study by a pathologist specializing in chILD. Lung biopsies were obtained as part of the diagnostic work-up prior to initiation of specific therapies.
6. Lung function tests
Pulmonary function tests were performed at baseline and, where available, longitudinally during follow-up. Pulmonary function testing was performed according to European Respiratory Society/American Thoracic Society international standards. Lung function parameters (forced expired volume in 1 second [FEV1], forced vital capacity [FVC], diffusing capacity of the lungs for carbon monoxide [DLCO]) were expressed as percent predicted values based on Global Lung Function Initiative reference equations [43].
Due to the retrospective design of the study, data completeness was variable. Although the registry prospectively collects longitudinal data based on clinical visits, detailed information was not available for every visit in all patients, particularly for cases included retrospectively.
7. Genetic analysis
Genetic analysis was performed using exome sequencing. The genetic variants were evaluated according to American College of Medical Genetics and Genomics guidelines using in silico prediction tools and comparison database, as described in Supplementary Table 1 [44].
Results
Ten patients with TBDs-associated chILD were identified in the registry search. According to the etiologic classification system, all patients were classified as systemic disease, with one child having a hepatopulmonary syndrome [45].
1. Clinical presentation
The clinical features and key findings of the cohort are summarized in Tables 1 and 2. Overall, patients presented with heterogeneous respiratory symptoms and multisystem involvement. The most common respiratory manifestations included dyspnea, cough, and impaired gas exchange, while extrapulmonary features such as bone marrow dysfunction and liver involvement were also observed in several patients.
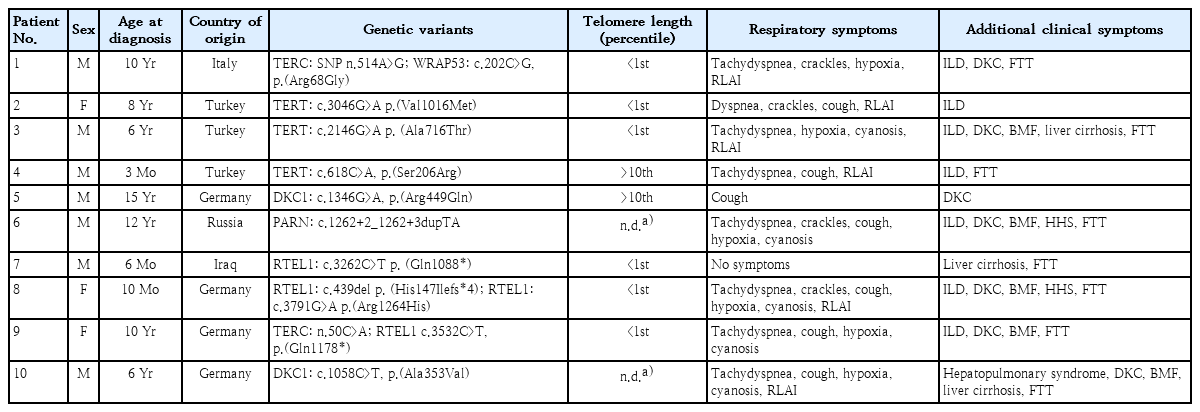
Characteristics of the pediatric study cohort with telomere biology disorders (N=10)
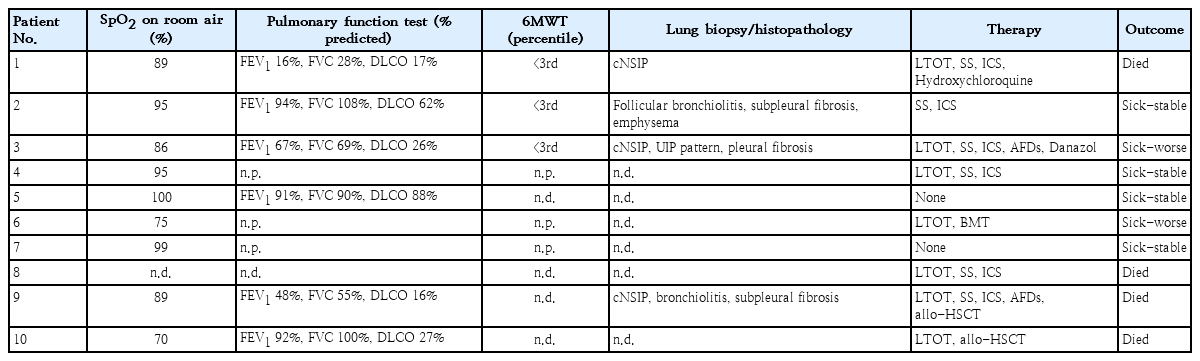
Clinical findings, treatment, and outcomes of pediatric telomere biology disorders study cohort (N=10)
2. Telomere length measurement
Telomere length could be measured in 8 patients. In 6 of them, the values were below the 1st percentile of a healthy cohort of pediatric patients aged 2–18 years. In 2 patients, telomere length was not shortened compared to the values of the pediatric reference cohort. In both cases, there were pronounced symptoms consistent with TBDs, suggesting that telomere dysfunction may be present even in the absence of telomere shortening [46].
3. Chest CT analysis
The structured evaluation of the HRCT scans is shown in Fig. 1A, representative images are displayed in Fig. 1B. The most common chest HRCT findings were diffuse or patchy ground-glass opacities, cystic lesions and linear or reticular opacities.
(A) HRCT findings in children with TBD-related ILD. Bar chart summarizing the most common HRCT features observed in pediatric patients with genetically confirmed telomeropathy and ILD. Ground-glass opacity was the most frequent finding, followed by bronchial wall thickening, emphysema, and cystic lesions. Other notable patterns included linear or reticular opacity, focal consolidation, mosaic attenuation, and nodular opacity. The frequency of the patterns among the 10 patients is shown. (B) HRCT findings in children with TBDrelated ILD. Panel A: Patient 1, a 10-year-old boy with diffuse GGO (arrow), reticular opacity, mosaic attenuation, and cystic lesions. Panel B: Patient 2, a 7-year-old girl with nodular opacity, diffuse GGO, cystic lesions (arrow), and mosaic attenuation. Panel C: Patient 3, a 17-yearold boy with patchy areas of GGO and reticular opacity. Panel D: Patient 4, a 2-year-old boy with patchy areas of GGO (arrow) and reticular opacity. Panel E: Patient 6, a 12-year-old boy with diffuse GGO and bronchial wall thickening. Panel F: Patient 8, a 10-month-old girl with diffuse GGO and bronchial wall thickening. Panel G: Patient 9, a 10-year-old girl with diffuse GGO and emphysema. HRCT, high-resolution computed tomography; TBD, telomere biology disorder; ILD, interstitial lung disease; GGO, ground-glass opacity.
4. Histopathology
The results of the lung biopsy are shown in Table 2 and Fig. 2. Different histological patterns were found, including cellular nonspecific interstitial pneumonia (NSIP), follicular bronchiolitis and usual interstitial pneumonia combined with predominantly lymphocytic infiltration of the alveolar septa.
Histopathology of lung biopsies in children with TBD. Key findings are indicated by arrows. Patient 1 (panels A–C): Lung sections showing dense interstitial lymphomononuclear infiltrates with septal thickening. The pleura was moderately thick and contained small lymphoid aggregates. Occasional intra-alveolar histiocytes were also visible. These findings are consistent with a cellular NSIP pattern in the context of TBD. Patient 2 (panels D–F): Sections demonstrating pleural and subpleural fibrosis as well as features of follicular bronchiolitis with prominent bronchial-associated lymphoid tissue. Patient 3 (panels G–I): Histological sections showing UIP-typical fibrosis affecting the periphery of the lobulus, associated with alveolar wall thickening and lymphocytic inflammatory infiltrate. TBD, telomere biology disorder; NSIP, nonspecific interstitial pneumonia; UIP, usual interstitial pneumonia.
5. Lung function tests
Lung function data were recorded in 6/10 patients and are listed in Table 2. A substantial impairment of diffusing capacity was found in 5/6 children. Fig. 3A and B show the lung function over time for patients 3 and 9 with severe diffusion impairment and loss of FEV1 and FVC.
(A) Longitudinal lung function parameters in patient 3 with TBD-associated ILD. Serial pulmonary function tests performed over a 31-month period starting at an age of 7 years in a child with TBD-associated ILD. The graph illustrates the progressive loss of lung function in FEV1, FVC, DLCO, and KCO (expressed as the percentage predicted). Initial therapy with nintedanib was administered from months 1 to 18, followed by a switch to pirfenidone. Although FEV1 and FVC remained relatively stable, a moderate decline was observed in patients with DLCO and KCO during the first 12 months, with partial recovery during pirfenidone treatment. This course reflects the complex and variable trajectories of telomeropathy-related ILD during antifibrotic therapy. (B) Longitudinal lung function parameters in a Patient 9 with TBD-associated ILD. This figure illustrates the longitudinal course of lung function and oxygen saturation in patient 9, who was diagnosed with dyskeratosis congenita and underwent bone marrow transplantation at 5 years of age. Serial measurements of FVC, FEV1, DLCO, and SpO2 are shown from age 6 to 18 years. Owing to progressive deterioration, pirfenidone therapy was initiated at 11 years of age. Following the initiation of treatment, temporary stabilization of lung function was observed, particularly DLCO and oxygen saturation, followed by a gradual decline in later adolescence. TBD, telomere biology disorder; ILD, interstitial lung disease; FEV1, forced expired volume in 1 second; FVC, forced vital capacity; DLCO, diffusing capacity of the lungs for carbon monoxide; KCO, carbon monoxide transfer coefficient; SpO2, peripheral oxygen saturation.
6. Genetic analysis
Of the 10 patients, 3 patients had variants in the TERT gene, 2 in the DKC1 gene, 1 patient simultaneously in the TERC gene and WRAP53 gene, another in the TERC gene and in the RTEL1 gene, 1 patient in the PARN gene, and 2 patients in the RTEL1 gene. All variants were heterozygous except for the hemizygous variants in DKC1. In addition, one of the patients with RTEL1 variants harbored two variants that were most likely in trans. Five of the identified variants have not previously been described and were classified in this study as variants of unknown significance (VUS) based on in silico analyses and available frequency data. The remaining variants have been reported in patients with DKC or BMFS; of these, six were classified as (likely) pathogenic, while two were considered common SNPs due to their high population frequency.
7. Outcome
In this pediatric cohort, disease course was frequently severe. Three patients underwent hematopoietic stem cell transplantation; however, outcomes remained poor, with progressive respiratory failure and death in 4 cases. Long-term oxygen therapy was required in 7 of 10 patients, reflecting advanced pulmonary disease. Antifibrotic therapy with nintedanib or pirfenidone was administered in 2 patients. While treatment was associated with initial stabilization of pulmonary function and a slower rate of decline, overall clinical status continued to deteriorate over time.
Overall, the clinical course was characterized by progressive respiratory impairment in the majority of patients, with only limited periods of stabilization. In several cases, disease progression occurred despite intensive medical treatment, highlighting the aggressive nature of TBD-associated chILD. Notably, extrapulmonary manifestations, including hematologic involvement, further contributed to disease burden and complexity of management.
These findings underscore the heterogeneity of disease trajectories but consistently indicate a high morbidity and mortality in this patient population.
Discussion
This study presents one of the largest pediatric case series of TBDs-associated childhood ILD, highlighting the evolving understanding and clinical nuances of this rare genetic syndrome in children.
Our cohort exhibited diverse clinical presentations and genetic variants, including variants in TERT, TERC, DKC1, PARN, RTEL1, and WRAP53, half of which are novel and were classified as VUS. Based on the clinical presentation and associated findings like the functional analysis of telomere length measurement, we can classify 2 of 5 variants pathogenic, which were previously classified as VUS. This mirrors findings from adult IPF cohorts, where up to one-third of familial and 10%–25% of sporadic cases carry telomere-related mutations and share similar genetic heterogeneity [18,47,48]. Histology in our series revealed different patterns of lung injury, including pleural/subpleural fibrosis, follicular bronchiolitis, and cellular NSIP. Several patients showed clear signs of pulmonary fibrosis [31], which likely had a substantial negative impact on clinical outcome. These findings are consistent with adult studies reporting pleuroparenchymal fibroelastosis-like and NSIP patterns among telomere mutation carriers.
The coexistence of fibrotic, inflammatory, and lymphoid patterns in pediatric patients suggests a continuum of pathobiological changes over time.
HRCT imaging revealed typical findings of pediatric ILD, including ground-glass opacities, mosaic attenuation, reticular changes, and cystic lesions; however, no distinct radiographic pattern was observed that could be attributed specifically to TBDs-associated ILD.
Lung function follow-up showed progressive reduction in DLCO, FVC, and FEV1. In 2 patients, antifibrotic therapy with nintedanib and pirfenidone appeared to stabilize or improve lung volumes during midterm follow-up. This might align with adult IPF data demonstrating slowed FVC decline in mutation carriers treated with antifibrotics. Importantly, the InPedILD trial recently established that weight-based nintedanib dosing in children (6–17 years) with fibrosing ILD is safe, well tolerated, and achieves plasma exposure similar to adults. While specific data on telomere-related pediatric ILD remain limited, our observations support extrapolating antifibrotic strategies to this subgroup [49-52]. Danazol has shown promise in adult TBD cohorts for extending telomere length and stabilizing hematologic and pulmonary parameters. However, randomized trials in IPF have not demonstrated clinical benefit in advanced disease and highlight concerns over hepatic toxicity. The ongoing TELO‑SCOPE study (NCT 04638517) is currently evaluating danazol’s safety and efficacy in subjects aged >5 years with PF and TBD [14,18,53].
The clinical course in our cohort was predominantly severe. Four children died despite intensive medical treatment. Three patients underwent allogeneic hematopoietic stem cell transplantation or bone marrow transplantation; two died due to transplant-related complications, while the other experienced only transient stabilization. These findings are consistent with data from adult cohorts, which report increased mortality and complication rates in patients with telomeropathies undergoing transplantation. Overall, long-term survival remains limited in both pediatric and adult patients. These observations underline the need for early risk stratification and alternative therapeutic strategies. TBDs confer higher risk pre‑ and postlung transplant, including hematologic, renal, airway healing complications, and mortality [54,55]. Our observation of systemic involvement and bone marrow impairment reinforces the need for early transplant referral and multidisciplinary coordination.
1. Clinical implications and future directions
Chronic cough and tachypnea are among the most common respiratory symptoms in childhood. Our findings highlight that in children with unexplained ILD, TBDs should be considered as a potential underlying cause, even in the absence of classic DC features. This should prompt further diagnostic evaluation, including genetic testing and telomere length measurement. This study may contribute to increased awareness of TBDs and facilitate earlier recognition, thereby helping to avoid unfavorable diagnostic delays.
1) Genetic screening
Pediatric ILD diagnostics should routinely include telomere maintenance genes—even in absence of classic dyskeratosis signs—to facilitate early diagnosis and personalized care.
Genetic counseling is an essential component in the management of TBDs and should include family screening of at-risk relatives, including siblings and parents. In adolescent patients, counseling may also address reproductive options, including considerations for fertility preservation such as sperm or oocyte banking.
2) Antifibrotic therapy
Early initiation of nintedanib or pirfenidone—supported by adult data and pediatric safety trials—may slow the disease trajectory in cases of fibrosing telomeropathy-associated pediatric ILD.
3) Danazol and beyond
Awaiting results of the danazol trials, novel therapies targeting telomerase activation and senolytic pathways warrant exploration.
4) Integrated care models
A multidisciplinary approach—including pediatric pulmonology, hematology, genetics, and transplant specialists—is essential for optimal management of this multisystem condition.
This study has certain limitations, including the heterogeneity of the cohort and, in some cases, incomplete data collection. Telomere length measurement by quantitative PCR (qPCR) is subject to methodological limitations, including interassay variability, lack of resolution between leukocyte subpopulations, and its inability to detect critically short telomeres.
Notably, 2 patients in our cohort exhibited clinical features suggestive of TBDs despite telomere length within the normal range (>10th percentile). This discrepancy may reflect limitations of average telomere length measurements, as critically short telomeres in a subset of chromosomes may not be detected by qPCR. More sensitive techniques, such as TeSLA or flow-FISH, could provide a more detailed assessment of telomere length distribution across different cell populations. These findings underscore the complexity of genotype-phenotype correlations and highlight the need for cautious interpretation, particularly in cases involving variants of uncertain significance.
In addition, data on early graying and detailed family history of ILD were not systematically available and should be addressed in future studies. Furthermore, detailed longitudinal data on treatment duration and standardized outcome measures were not consistently available, limiting more precise assessment of disease course and treatment response. Nevertheless, to our knowledge, it represents one of the largest pediatric cohorts with TBDs reported to date.
In conclusion, this cohort underscores that TBDs are a rare cause of pediatric ILD. Our histopathologic, functional, and therapeutic insights, together with emerging literature, strengthen the urgent need for early genetic testing and careful consideration of all treatment options, including antifibrotic interventions. Future multicenter studies and randomized trials will be critical to refine management and improve outcomes for these vulnerable patients.
Supplementary materials
Supplementary Table 1 is available at https://doi.org/10.3345/cep.2026.00290.
Genetic findings of pediatric study cohort with telomere biology disorders
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported, except by MG who reports serving on adjudication and advisory board for the InPedILD study sponsored by Böhringer Ingelheim.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgments
The authors thank the participating centers of the European chILD-EU Registry for their collaboration and contribution of clinical data. We acknowledge the patients and their families for their participation. We also thank the multidisciplinary review board for centralized evaluation of radiologic, histopathologic, and genetic findings.
Author contribution
Conceptualization: MGM, MG, FP; Data curation: MGM, CKR, KK, DG, FWH, JLZ, SRH, JH, SZ, MHT, HO, ER, TSE, ATA, NE, NU, SN, MM, FB, TRG, MG, FP; Formal analysis: MGM, CKR, DG, FWH, JLZ, SRH, JH, MG; Methodology: MGM, MG, FP; Project administration: KK, MG; Visualization: MGM, SRH; Writing - original draft: MGM; Writing - review & editing: MGM, CKR, KK, DG, FWH, JLZ, SRH, JH, SZ, MHT, HO, ER, TSE, ATA, NE, NU, SN, MM, FB, TRG, MG, FP