Testosterone therapy in boys with constitutional delay of growth and puberty: a PubMed-based systematic review and exploratory meta-analysis
Article information

Abstract
Constitutional delay of growth and puberty (CDGP), the most common cause of delayed puberty in boys, accounts for the majority of pediatric endocrinology referrals. Although traditionally viewed as a variant of normal development, affected adolescents frequently experience short stature relative to their peers, delayed secondary sexual characteristics, and clinically meaningful psychosocial distress. Short-course low-dose testosterone has been used for more than 5 decades to accelerate pubertal progression and linear growth; however, the evidence base is heterogeneous and has not been synthesized in a PubMed-indexed review anchored in original testosterone studies. To systematically review PubMed-indexed studies from the last 40 years evaluating testosterone therapy in boys with CDGP or closely related self-limited delayed puberty and perform an exploratory meta-analysis of outcomes for which directly extractable comparative data are available. PubMed was searched from January 1, 1986, to March 10, 2026, for relevant original studies, systematic reviews, and meta-analyses. Eligible reports enrolled boys with CDGP or self-limiting delayed puberty treated with testosterone and reported growth, pubertal progression, bone age, predicted or near-adult height, or safety outcomes. Randomized studies were appraised by the Cochrane revised tool for risk of bias in randomized trials, while nonrandomized studies were appraised using the Risk of Bias in Non-randomized Studies – of Interventions. Random-effects mean differences (MDs) for height velocity were calculated when comparative means and dispersions were extractable. Twenty original studies involving 1,329 boys met the qualitative inclusion criteria, together with 2 supporting evidence syntheses. Across formulations (intramuscular testosterone enanthate or cypionate, depot ester mixtures, oral testosterone undecanoate, and transdermal gel), the literature consistently showed greater short-term height velocity and more rapid pubertal progression in treated boys without a clinically meaningful adverse effect on near-adult height when conservative regimens were used. Only 2 controlled studies (46 boys) directly provided pooled height velocity data. Random-effects pooling showed a statistically significant increase in short-term height velocity with testosterone versus placebo or no treatment (MD, 2.40 cm/yr; 95% confidence interval, 1.49–3.32; I²=0%). Narrative evidence from long-term studies does not support the detrimental effects of brief low-dose testosterone administration on near-adult or adult height. Testosterone therapy in boys with CDGP was associated with faster short-term growth and pubertal maturation, and long-term data did not show a detrimental effect on near-adult height when conservative time-limited regimens were used. The quantitative evidence base is small and methodologically heterogeneous, and modern multicenter randomized trials incorporating validated patient-reported outcomes and long-term follow-ups are necessary.
Key message
In boys with constitutional delay of growth and puberty, a short course of low-dose testosterone consistently accelerates linear growth and advances pubertal maturation. Long-term follow-up studies do not show a clinically meaningful effect of conservative regimens on near-adult height. As the pooled quantitative evidence represents only 46 boys in 2 controlled studies, treatment should remain individualized, while larger randomized trials using standardized patient-reported outcomes are needed.
Graphical abstract. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Introduction
Delayed puberty in boys is clinically defined as failure of testicular enlargement to a volume of at least 4 mL by 14 years of age. The most common cause is self-limited delayed puberty, historically termed constitutional delay of growth and puberty (CDGP), which accounts for approximately 60%–80% of boys referred to pediatric endocrinology for the evaluation of delayed sexual maturation [1,2]. Although CDGP is ultimately benign, distinguishing it from permanent hypogonadotropic hypogonadism, chronic systemic disease, and syndromic causes remains a central clinical challenge and often requires prolonged observation or biochemical testing [1,2].
Although CDGP has been traditionally described as a variant of normal development, it is not clinically trivial. Affected adolescents often present with short stature relative to their peers, the absence of secondary sexual characteristics, school- and sports-related embarrassment, and measurable psychosocial distress. Longitudinal data also suggest that self-limiting delayed puberty is not entirely consequence-free; moreover, possible associations with adult skeletal health, psychosocial adjustment, and metabolic endpoints have been reported [2,3].
The natural history of untreated CDGP is more complex than the traditional assumption of fully spontaneous catch-up. Several cohort studies have shown that most boys eventually reach an adult height within their target range, while a minority fall short of their target or predicted adult height. This appears to be driven by a combination of delayed pubertal onset, a possibly shortened pubertal tempo, and an attenuated peak pubertal growth velocity [4,5]. These findings have motivated interest in treatments that can induce a pubertal growth spurt without compromising the patient's near-adult height.
Testosterone in different formulations and doses has been used for this purpose for more than 5 decades, including intramuscular (IM) testosterone enanthate or cypionate, depot ester mixtures, oral testosterone undecanoate, and, more recently, transdermal gel preparations. Most older studies reported short-term gains in height velocity and pubertal maturation, but the evidence is methodologically heterogeneous, with variations in age at initiation, baseline bone age delay, dose, injection interval, duration, comparator, and outcome definitions [6-21]. Treatment strategies have also evolved over the past 4 decades. The long-course IM depot regimens of the 1980s–1990s have increasingly given way to short, low-dose IM courses in the 2000s and oral and transdermal preparations more recently. Aromatase inhibitors such as letrozole have emerged as alternatives that preserve endogenous hypothalamic-pituitary-gonadal (HPG) axis activity [20,22].
Recent evidence syntheses have highlighted the same problem from a different angle: despite widespread clinical use, the testosterone evidence base in adolescent boys remains fragmented and often has a high or unclear risk of bias. One recent systematic review focused mainly on formulation comparisons, while a separate meta-analysis of CDGP centered on letrozole and treated testosterone largely as an active comparator [22,23]. Therefore, a focused synthesis is needed of testosterone anchored in PubMed-indexed original studies over the last 4 decades.
The present study aimed to accomplish the following: (1) Systematically review original PubMed-indexed studies, systematic reviews, and meta-analyses on testosterone treatment in boys with CDGP or closely related self-limited delayed puberty published over the last 40 years; and (2) Perform an exploratory meta-analysis of quantitative outcomes for which directly extractable comparative data were available with a particular focus on height velocity and height-related safety.
Methods
1. Study design and search strategy
We conducted a structured PubMed-based systematic review for relevant articles published between January 1, 1986, and March 10, 2026. The search terms combined concepts related to testosterone, delayed puberty, constitutional delay in growth and puberty, self-limiting delayed puberty, adolescent boys, and specific testosterone formulations. PubMed-indexed original studies formed the primary evidence base, while PubMed-indexed systematic reviews and meta-analyses were included to contextualize the field.
2. Inclusion criteria
The study inclusion criteria were as follows: original human studies of boys and adolescent males with CDGP or closely related self-limited delayed puberty treated with a testosterone-based regimen; randomized, comparative, retrospective, or prospective cohort designs; and reporting at least one clinically relevant endpoint, including height velocity, pubertal progression, testicular volume, Tanner stage, bone age progression, predicted adult height, near-adult or adult height, endocrine response, and safety. PubMed-indexed systematic reviews and meta-analyses were included for contextual discussion only and not pooled with the original studies.
3. Exclusion criteria
The study exclusion criteria were as follows: female-only studies; non-human studies; reports focused on permanent hypogonadism, chronic systemic disease, or syndromic conditions without a separable CDGP or self-limited delayed puberty subgroup; conference abstracts lacking extractable data; clearly duplicate or nonindependent secondary reports from the same primary dataset; and no testosterone intervention.
4. Outcomes
The primary endpoint of the meta-analysis was height velocity (cm/yr). Secondary outcomes for the systematic review included testicular volume progression, Tanner stage advancement, bone age progression, predicted adult height, near-adult or adult height, endocrine markers (luteinizing hormone [LH], follicle-stimulating hormone [FSH], testosterone, insulin-like growth factor-1 [IGF-1]), patient-reported outcomes, and adverse effects.
5. Data extraction
We extracted the following data from each eligible study: first author, year, country, design, sample size, age at initiation, baseline pubertal stage when available, testosterone formulation and dose, injection interval, treatment duration, comparator, follow-up window, observation window over which height velocity was calculated, main outcomes, and extractability of the comparative numerical data. The evidence synthesis is summarized separately.
6. Risk of bias assessment
Randomized studies were appraised using the Cochrane revised tool for risk of bias in randomized trials, while nonrandomized studies were evaluated using the Risk of Bias in Non-randomized Studies – of Interventions. The studies were categorized pragmatically as low risk, some concerns, moderate risk, serious risk, or high or unclear risk according to design and reporting quality.
7. Statistical analysis
For the quantitative synthesis, random-effects mean differences (MDs) with 95% confidence intervals (CIs) were calculated. When a study reported standard error of the mean (SEM) instead of standard deviation (SD), SD was derived as SEM × √n. Heterogeneity was quantified using I². As only 2 studies were pooled for the primary outcome, publication bias testing was not performed. All other outcomes were synthesized narratively.
Results
1. Study selection and PRISMA flow
From the 126 records identified in PubMed and retained from a prior evidence map, 39 were subjected to fulltext review; 17 were excluded for lacking a testosterone intervention, including mixed or inseparable populations, being nonoriginal reports, including duplicate or secondary datasets, or disclosing insufficient eligibility details. Twenty original PubMed-indexed studies (1,329 boys) were included in the qualitative synthesis. Two PubMed-indexed evidence syntheses were retained for contextual discussion. Eighteen of the 20 original studies could not be included in the primary meta-analysis because of active comparator designs, single-arm designs, near-adult height-only outcome reporting, or missing comparative mean/SD data. Two controlled studies (46 boys) provided directly extractable comparative data on short-term height velocity (Fig. 1).
PRISMA-style study flow chart. The PRISMA-style diagram shows 126 records screened, 39 full-text articles assessed, 17 excluded (no testosterone intervention, mixed/inseparable populations, nonoriginal reports, duplicate/secondary datasets, or insufficient eligibility details), 20 original studies (1,329 boys) included in the qualitative synthesis, 2 supporting evidence syntheses included for contextual discussion, and 2 controlled studies (46 boys) included in the exploratory quantitative synthesis (mean difference [MD], 2.40 cm/yr; 95% confidence interval [CI], 1.49–3.32; I²=0%). The discrepancy between qualitative and quantitative inclusion reflected active comparator designs, singlearm designs, near-adult height-only outcome reporting, and missing comparative mean/standard deviation (SD) data in 18 of the 20 original studies. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
2. Characteristics of testosterone regimens across included studies (Table 1)
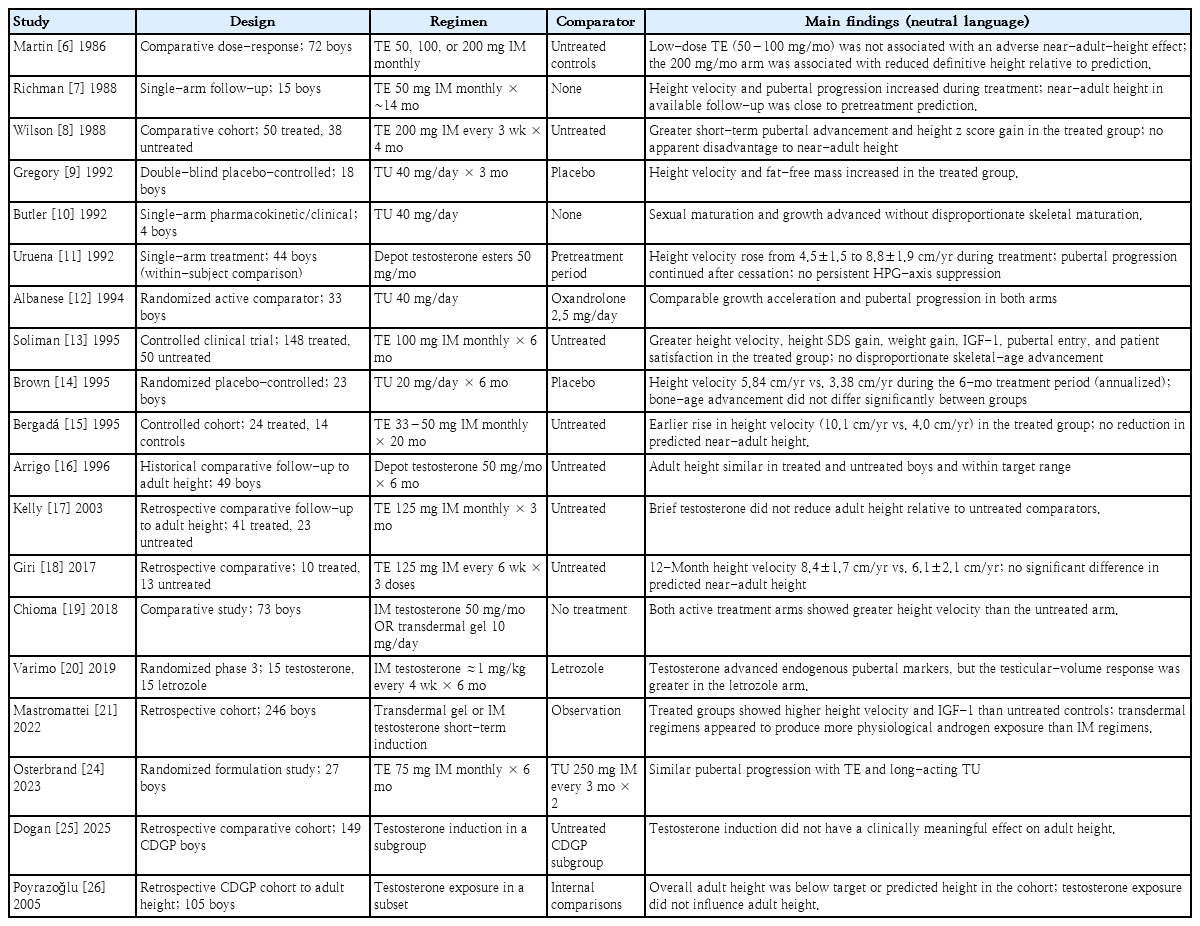
Original studies of testosterone therapy in boys with CDGP or self-limited delayed puberty
1) Age at treatment initiation
Across the 20 included studies, the mean or median age at initiation was 10.5–16.2 years, with a pooled central estimate of approximately 13.8 years. The most common age band was 13.5–14.5 years, consistent with the current clinical practice of offering short-course testosterone in boys whose testicular volume remains below 4 mL at 14 years of age.
2) Formulation-specific dosages
The formulation-specific dosages were as follows: (1) IM testosterone enanthate or cypionate: 50–125 mg per injection (overall range, 33–200 mg). The 50–100 mg range was used in 9 of the 12 IM studies, reflecting the progressive shift away from higher-dose regimens after the Martin 1986 dose-response study6); (2) Depot testosterone ester mixtures (Sustanon-type preparations) (an injectable mixed testosterone ester formulation designed to provide both rapid and prolonged testosterone release): most commonly 50 mg/mo [11,16]; (3) Oral testosterone undecanoate (20–40 mg/day): within the standard range [9,10,12,14]; (4) Transdermal testosterone gel: 10 mg/day [19,21]; and (5) Long-acting testosterone undecanoate depot injection: 250 mg every 3 months [24].
3. Height velocity: narrative findings
All 20 studies that reported height velocity as an outcome showed an increase during or after testosterone treatment relative to the pretreatment period, untreated comparator, or placebo arm. Intrasubject increments ranged from approximately 2 to 6 cm/yr and intergroup differences ranged from 1.4 to 6.1 cm/yr. The observation windows over which height velocity was calculated varied: 6-month treatment period, annualized [14]; 12 months [18], during and shortly after treatment, annualized [11]; and 6-month intervals within a 20-month follow-up [15]. In the Discussion section, we note that the velocities derived from observation windows shorter than 12 months are more susceptible to seasonal and intrasubject variability and should be interpreted accordingly (Fig. 2).
Effect of testosterone therapy on height velocity in boys with delayed puberty across selected studies. Height velocity increased during testosterone treatment in all included studies, with the largest absolute increments observed with low-dose intramuscular regimens. The observation window differed across studies: Brown et al. [14] reported velocity annualized from a 6-month treatment period; Uruena et al. [11] compared pretreatment and treatment-period velocities within the same patients (so the apparent magnitude of effect partly reflected intrasubject change); Bergadá and Bergadá [15] reported velocities calculated at 6-month intervals within a 20-month follow-up; and Giri et al. [18] reported 12-month velocities. The dark bars represent the comparator or pretreatment period, while the light bars represent the testosterone regimen. TE, testosterone enanthate; TU, testosterone undecanoate.
4. Pubertal progression and testicular volume
All controlled and comparative studies reporting the Tanner stage showed at least one stage of advancement over 3–6 months of treatment compared with minimal or no advancement in untreated boys. Testicular volume increased in treated boys in most studies; however, in a randomized comparison with letrozole [20], the testicular volume response was greater in the letrozole versus testosterone arm. This difference is mechanistically explained by the preservation of endogenous gonadotropin levels during aromatase inhibition (Table 2).
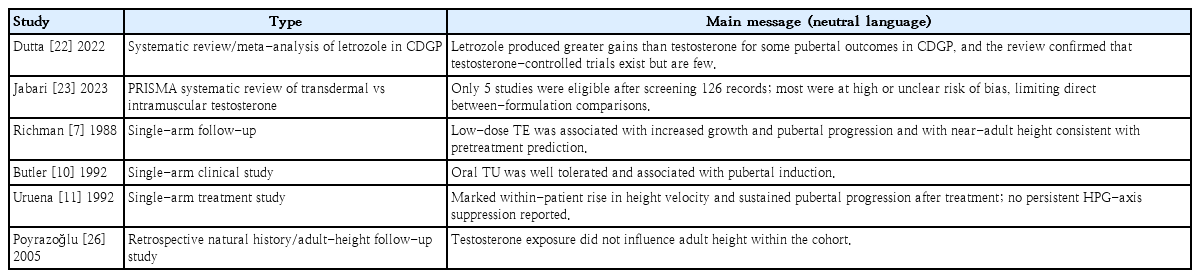
Supportive evidence syntheses and narrative-only studies
5. Bone-age progression and predicted height
Across the included studies, bone-age advancement in treated boys did not exceed chronological age progression in a clinically meaningful manner with low-dose regimens (≤100 mg depot testosterone every 4 weeks or equivalent). Brown et al. [14] reported no statistically significant intergroup differences in bone-age advancement. In contrast, Martin et al. [6] showed that the 200 mg/mo dose arm produced disproportionate bone-age advancement and a reduction in definitive versus predicted height, establishing a dose-skeletal-maturation relationship that has since shaped clinical practice.
6. Near-adult and adult-height outcomes from long-term studies
Five studies provided long-term follow-up to near-adult or adult height [6,16,17,25,26]. All 5 showed that brief, low-dose testosterone did not produce a clinically meaningful reduction in adult height relative to untreated comparators or target height, with the important caveat that the study of Martin et al. [6] 200 mg/mo arm did compromise definitive height.
7. Endocrine and body-composition outcomes
IGF-1 levels increased during treatment according to Soliman et al. [5], while fat-free mass increased according to Gregory et al. [9], consistent with the known anabolic and growth hormone (GH) axis-stimulating effects of testosterone. Endogenous LH and FSH levels were measured during treatment [11,20], and transient suppression was observed with subsequent recovery after their discontinuation in studies that reported post-treatment endocrine data.
8. Patient-reported and psychosocial outcomes
Only 1 study [13] reported a formal patient-satisfaction assessment, and none of the included studies used a validated standardized psychometric instrument (such as the PedsQL, Rosenberg Self-Esteem Scale, Child Behavior Checklist, or body-image scale). Therefore, the clinical rationale for treatment, which rests primarily on distress related to short stature and the absence of secondary sexual characteristics, is supported by qualitative clinical impressions rather than quantitative psychometric data. This is one of the most important research gaps in the field.
9. Safety and adverse-effect reporting
Adverse events were uncommon in all included studies. Reported events include transient acne, minor injectionsite discomfort, gynecomastia in a small minority of boys (particularly at higher doses), and transient suppression of testicular volume gain during the treatment window. To the best of our knowledge, no study reported clinically significant hepatic, cardiovascular, or hematological adverse events.
10. Exploratory meta-analysis of short-term height velocity (Table 3)

Exploratory meta-analysis of short-term height velocity (n=46 boys across 2 controlled studies)
Only 2 controlled studies [14,18] (combined n=46 boys) reported directly pooled means and dispersion for short-term height velocity. Random-effects pooling yielded a MD of 2.40 cm/yr (95% CI, 1.49–3.32) in favor of testosterone, with no statistical heterogeneity (I²=0%). This pooled estimate should be considered hypothesis-generating rather than confirmatory given the small combined sample size.
Discussion
This review supports the long-standing clinical impression that testosterone accelerates short-term pubertal progression and linear growth in boys with CDGP. The direction of the effect was consistent across the 4 decades as well as formulations. The pooled height-velocity estimate (MD≈2.4 cm/yr) aligns closely with the individual results of the 2 controlled studies that contributed directly extractable data [14,18].
1. Heterogeneity of evidence base
The PRISMA diagram (Fig. 1) demonstrates that a qualitative review is much broader than a quantitative synthesis in this field; this is by design rather than oversight. The principal sources of noncomparability across the 20 included studies are: (1) age at initiation (10.8–16.2 years), (2) baseline pubertal stage (Tanner G1 to G2–3), (3) formulation (enanthate, cypionate, depot ester mixtures, oral undecanoate, transdermal gel), (4) dose (20 mg/day oral to 200 mg every 3 weeks IM), (5) injection interval (every 2–12 weeks), and (6) treatment duration (3–20 months). These are the primary reasons why the data of only 2 of 20 studies were suitable for pooling as well as why meaningful formulation- or dose-level subgroup analyses remain impossible from the published literature.
2. Near-adult height: no detrimental effect of brief low-dose regimens
A clinically important conclusion is that the literature does not support the common concern that brief low-dose testosterone compromises near-adult or adult heights. Biologically, this concern is reasonable; supraphysiological androgen exposure can accelerate aromatization to estradiol and, therefore, accelerate epiphyseal senescence. In practice, however, the studies that followed patients to near-adult or adult height [16,17,25,26] consistently found no meaningful adverse effect when conservative regimens were used, while one dose-response study [6] confirmed that higher-dose regimens (200 mg/mo) create problematic exposure.
3. Defining conservative regimens: the Martin threshold
To make the notion of a "conservative" or "low-dose" regimen operational, we propose anchoring it to Martin's [6] dose-response data. Specifically, conservative regimens in CDGP can be defined as those delivering ≤100 mg of depot testosterone per 4 weeks (or an equivalent cumulative exposure of ≤400–600 mg over a 3–6-month course) in adolescent boys. The study of Martin et al. [6] and all subsequent low-dose studies (100 mg/mo×6 months [5]; 125 mg/mo×3 months [17]; 33–50 mg/mo [15]; 125 mg every 6 weeks ×3 doses [18]) reported no disproportionate increase in bone age/chronological age ratio or a clinically meaningful reduction in the predicted or near-adult height. Above this threshold (Martin's 200 mg/mo arm), accelerated bone maturation and a reduction in definitive height relative to the prediction were observed. The equivalent conservative range for oral testosterone undecanoate appears to be 20–40 mg/day for up to 6 months [9,14].
4. Mechanistic considerations for growth and skeletal maturation
Mechanistically, testosterone accelerates growth and pubertal tempo via several pathways. It directly induces virilization and pubertal progression, stimulates the GH/IGF-1 axis, increases lean body mass, and may influence appetite, confidence, and physical activity, all of which can support linear growth during the pubertal transition. The rise in IGF-1 levels reported by Soliman et al. [13] and the gain in fat-free mass reported by Gregory et al. [9] are consistent with this integrated anabolic effect.
Low-dose regimens appear to provide sufficient androgenic signaling to initiate puberty and permit an earlier growth spurt without causing disproportionate bone age advancement. This balance is important because excessive androgen is converted to estradiol via aromatization, which is the principal mediator of growth plate senescence and epiphyseal fusion. Therefore, neutral near-adult height findings in long-term studies make physiological sense when treatment is brief and conservative, whereas the less favorable outcomes with higher-dose regimens in Martin et al. [6] fit the biology of accelerated epiphyseal maturation [6,16,17].
5. Mechanistic considerations for aromatase inhibition (letrozole)
Letrozole acts by blocking the aromatase-mediated conversion of testosterone to estradiol, which has 2 simultaneous consequences: (1) endogenous serum testosterone rises approximately 2–3-fold due to reduced negative feedback at the hypothalamic-pituitary level and (2) serum estradiol falls. The clinical effects of letrozole on CDGP—Tanner stage progression, height velocity acceleration, and testicular volume increase—therefore reflect a combination of direct androgenic signaling from elevated endogenous testosterone levels and reduced estrogen-mediated epiphyseal senescence. This mechanistic framing helps explain why letrozole and testosterone can produce comparable short-term pubertal progression in some randomized trials [20], whereas letrozole tends to produce a greater testicular volume response because it preserves the gonadotropin drive [22].
6. Reproductive considerations: testicular volume and spermatogenesis
Exogenous testosterone transiently suppresses the hypothalamic GnRH pulse amplitude and pituitary LH/FSH secretion. During the treatment window, this reduced endogenous testicular stimulation and attenuated testicular volume growth, a mechanism that explains the smaller testicular volume increase observed in the testosterone arm than in the letrozole arm in one study [20]. In boys with true CDGP, this suppression was reversible after discontinuation and endogenous gonadotropin secretion recovered as expected. Uruena et al. [11] specifically investigated this question and found no evidence of persistent HPG-axis suppression after low-dose short-course testosterone; long-term follow-up cohort studies [16,17,25] similarly reported normal adult testicular volumes and gonadotropin trajectories. Nevertheless, the transient nature of suppression should be discussed explicitly with the family before treatment initiation. Data on adult semen parameters, specifically after pediatric CDGP treatment, are limited and represent a meaningful evidence gap.
7. Gonadotropin-based alternatives to testosterone monotherapy
In boys with suspected or confirmed permanent hypogonadotropic hypogonadism, gonadotropin-based regimens (human chorionic gonadotropin [hCG] alone or with recombinant FSH) are preferable to testosterone monotherapy because they directly stimulate the testes, promote testicular growth, and initiate spermatogenesis in the pubertal window. Specifically, testosterone remains the most widely used and best-studied short-term option for CDGP because endogenous puberty is expected to resume spontaneously. However, emerging evidence suggests that hCG±FSH regimens may produce more favorable testicular-volume trajectories while still permitting pubertal progression in boys with more severe delays or specific concerns about fertility-related outcomes. Letrozole, although not a gonadotropin, is an additional endogenous puberty-promoting alternative that was associated with a greater testicular volume response than testosterone in a randomized head-to-head comparison [20]. Direct comparative data between hCG/FSH and testosterone, specifically in CDGP, remain sparse and randomized head-to-head trials are valuable [27-30].
8. Psychosocial and quality-of-life outcomes
One limitation apparent across the 20 included studies was the near-absence of validated psychometric assessments. Only Soliman et al. [5] reported a formal patient-satisfaction measure, and no study has used a standardized instrument such as the PedsQL, Rosenberg Self-Esteem Scale, Child Behavior Checklist, or body-image scale validated in adolescent boys. Therefore, the clinical case for treatment relies primarily on qualitatively reported distress related to short stature, the absence of secondary sexual characteristics, and peer comparisons. Future randomized trials of CDGP treatment should incorporate validated patient-reported outcome measures as coprimary endpoints—at least a generic quality-of-life measure (PedsQL or equivalent), body-image measure suitable for adolescent boys, and self-esteem measure such as the Rosenberg Self-Esteem Scale—to enable a quantifiable rather than assumed psychosocial case for treatment.
9. Formulation: transdermal, oral, and long-acting options
This question remains unanswered. IM testosterone enanthate has the longest clinical track record; however, oral testosterone undecanoate and transdermal testosterone gel appear to achieve comparable short-term clinical effects in selected patients. Chioma et al. [19] and Mastromattei et al. [21] suggested that transdermal therapy may be effective and perhaps more physiological in some settings, while Österbrand et al. [24] found similar pubertal progression with testosterone enanthate and long-acting testosterone undecanoate in a small randomized study. Overall, formulation-specific evidence remains sparse and heterogeneous regarding firm ranking [19,21,23,24].
10. Risk of bias
Most of the included studies had moderate methodological limitations. Nonrandomized cohorts were vulnerable to confounding by indication because boys with greater distress or more severe short stature were more likely to receive treatment. Several older studies had limited blinding, incomplete reporting of variance, or poorly standardized outcome timing consistent with the conclusions of Jabari's systematic review that most eligible testosterone studies had a high or unclear risk of bias [23].
11. Limitations
This study has several limitations. First, our review was PubMed-based; older full texts were not always numerically extractable, and the primary meta-analysis was restricted to 2 controlled studies comprising 46 boys. Second, Brown et al. [14] enrolled prepubertal boys with constitutional growth delay rather than older boys with classic adolescent CDGP; therefore, the pooled effect should be interpreted as exploratory rather than confirmatory. And finally, some recent retrospective cohorts may contain overlapping center-specific populations, which argues against indiscriminate pooling.
12. Clinical implications and future research
Despite these limitations, this review supports a clinically useful conclusion: low-dose testosterone at or below the Martin threshold is a reasonable option for carefully selected boys with CDGP who have substantial psychosocial distress or a marked delay in growth and pubertal progression. The best-supported benefit is the short-term acceleration of height and pubertal progression, whereas the available long-term follow-up data are reassuring regarding near-adult height when conservative regimens are used. What the field now needs is not another small retrospective series but a modern multicenter randomized trial with standardized auxological data, a bone-age assessment, validated patient-reported outcomes (PedsQL, Rosenberg Self-Esteem Scale, body-image measures), endocrine monitoring of the HPG-axis during and after treatment, and long-term follow-up to documented adult height [2,23].
In conclusion, testosterone therapy in boys with CDGP or self-limited delayed puberty is associated with faster short-term height velocity and earlier pubertal progression. This exploratory pooled meta-analysis showed an increase in short-term height velocity of approximately 2.4 cm/yr (95% CI, 1.49–3.32), but this estimate was derived from only 46 boys across 2 controlled studies and must be considered hypothesis-generating rather than confirmatory. The broader narrative evidence does not support a clinically meaningful adverse effect on near-adult height when low-dose, time-limited regimens (≤100 mg depot testosterone every 4 weeks, or equivalent, for 3–6 months) are used. The present evidence base remains limited by small sample sizes, incomplete numeric reporting, the absence of validated psychometric outcome measurements, and interstudy heterogeneity. Therefore, testosterone should remain a carefully individualized therapy. Better-quality multicenter comparative trials with standardized auxological data, psychosocial endpoints, and long-term followup periods are under development.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contribution
Conceptualization: ATS; Data curation: ATS, FA, NA, NH, SA, KAS, MA; Formal analysis: ATS, MA; Methodology: ATS, NA, MA; Project administration: KAS; Visualization: FA, SA; Writing - original draft: ATS, FA, NH, SA, KAS; Writing - review & editing: ATS, NA