Impact of short and intensive art-based intervention on symptomatology and social interactions among children with autism spectrum disorder
Article information

Abstract
Background
Consensus on the effectiveness of art therapy in children with autism spectrum disorders (ASDs) is lacking in the literature.
Purpose
Here, we examined the effectiveness of a short and intensive art-based intervention on autistic symptomatology and social skills among children with ASD levels 2 and 3.
Methods
This pre- and postexperimental investigation included 13 children previously diagnosed with ASD levels 2 and 3 in Kurdistan Region in 2019. They completed the art-based intervention 2 hours/day for 3 days/week for 1 month. The activities included cutting and pasting squares and triangles, coloring black-and-white images, and recognizing and coloring shapes. Children used wooden and aquatic pens and scissors under guidance. Symptom severity was measured using the Social Responsiveness Scale (SRS-2), a validated tool for measuring the severity of autistic traits and symptoms that features subscales of social awareness, social cognition, social communication, social motivation, and autistic mannerisms. Children with ASD level 2 require significant support and experience notable difficulties in verbal and social communication, while those with ASD level 3 require extensive support and have the most severe form of autism. The outcome was measured one day before the course commenced and one week after completion.
Results
The mean patient age (n=13) was 8.15 years (standard deviation, 1.95; range, 5–11 years). Most patients were male (n=11, 84.62%). The mean SRS-2 score did not change significantly pre- to postexperiment (159 vs. 157, P=0.601). Similarly, we found no significant changes in social awareness (19 vs. 19, P=0.779); social cognition (28 vs. 27, P=0.199); social communication (56 vs. 54, P=0.600); social motivation (26 vs. 24, P=0.684); and autistic mannerisms (33 vs. 32; P= 0.780), respectively.
Conclusion
The art-based intervention did not improve autism symptoms or social interactions among children with ASD levels 2 and 3.
Key message
Question: Does a short and intensive art-based intervention affect symptoms and social interactions among children with autism spectrum disorder (ASD)?
Finding: The short and intensive art-based intervention did not affect symptoms in children with ASD level 2 or 3, including social awareness, social cognition, social communication, social motivation, and autistic mannerisms.
Meaning: The short and intensive art-based intervention did not improve the symptoms of patients with ASD.
Introduction
Autism spectrum disorder (ASD), also known as a pervasive developmental disorder, is one of the diagnostic developmental disabilities. It has 4 distinct disorders including autistic disorder, Asperger syndrome, childhood disintegrative disorder, and pervasive development disorder not otherwise specified. Persons who are diagnosed with ASD experience the following health issues; difficulty in social interaction, and communication, and issues of repetitive and self-stimulatory behaviors. ASD persons commonly experience sensory issues; experiencing a severe sensitivity or desensitivity to special auditory, visual, and tactile sensations. These symptoms limit the individuals’ ability in engaging and interact with their environment [1]. However, these symptoms may not be recognized until later childhood ages. Impairments in social interactions are in the following ways; impairments in using or comprehending eye contact, facial expression, and body postures. These symptoms can happen among children despite a lack of social and emotional responsiveness among ASD children [2].
According to the estimates of the trend in the burden of ASD at global, regional, and national levels from 1990 to 2019 of the Global Burden of Disease, the global incidence, prevalence, and disability-adjusted life year rates of ASD among children under 5 years were 91.09 per 100,000, 439.39 per 100,000, and 68.67 per 100,000 in 2019, respectively. The global incidence rate of ASD has decreased, but the prevalence and DALY have raised between 1990 and 2019. The regions with low sociodemographic index had the highest prevalence of cases (80.26%) and DALYs (81.24 %). Also, male children under 5 years have roughly 3 times ASD compared to female children. North Africa and the Middle East had 75.36 (61.72–90.27) and prevalence rates of 363.75 (298.26–435.12) per 100,000 population in 2019 [3]. A similar pattern was found in another systematic review [4].
Expressive arts therapy, particularly art-based therapeutic interventions presents a unique and comprehensive approach to dealing with autism symptoms among children. The art-based interventions could be effective to improve the relational capacity of ASD patients and to solve tactile and sensory integration, communication, emotion, and regulation, as well as social skills [5]. These interventions are important because ASD children suffer from difficulties in overall development, particularly issues in interpersonal relations, language, and behavior owing to brain damage. Scholars have tried to find out the internal aspect of autistic children through different therapeutic techniques. However, it seems that the children are more conformable to art-based interventions such as painting because art is the most simple and familiar language for children to express their minds [6]. ASD children are regularly referred to art therapy by clinicians [7] in coping with their communication and behavior issues and low self-esteem [8].
The effectiveness of art therapy and art-based interventions on symptoms among children with ASD has been examined in the literature. The current systematic reviews have recommended that art therapy may help ASD children in their social communication and interaction, and limited and repetitive behavior patterns [8]. ASD is a neurodevelopmental medical condition in which children have a reduction in social aspects. In other words, impairment in social communication is the main issue among ASD children. This impairment in social interaction and atypical attention of ASD children impacts cognition and behavior impairment [9,10]. Although the literature has paid the attention to the effectiveness of art therapy and art-based interventions on symptoms in children with ASD, there is no consensus on the effectiveness of art therapy on symptoms in children with ASD in the systematic reviews [8]. Also, many of these experimental studies have included ASD children with level 1. Due to the long-term and chronic nature of ASD, treating patients within a short period of time presents challenges. The effectiveness of intensive art-based intervention has not been evaluated in children with ASD. Therefore, we attempted to examine the effectiveness of a short-term, intensive art-based intervention. Both children with ASD and their parents require a short and highly effective technique for alleviating symptoms. Consequently, this study holds double importance. Therefore, we need more robust and high-quality experimental studies to investigate this issue, particularly in Iraq where we know little about the effectiveness of the therapy on children with ASD. In this regard, we aimed to examine the effectiveness of a short and intensive art-based intervention on autistic symptomatology among children with ASD levels 2 and 3. We hypothesized that social interaction will be improved after completing with the art-based intervention.
Methods
1. Study design and sampling
This paper is based on a pre and postexperimental research design. To our knowledge, this study was the first project that examined the effectiveness of art-based intervention among ASD children in Iraq. In the study, we included children aged 6 and 16 years old who were previously diagnosed with ASD in a 1-month art-based course. We recruited the ASD patients from the list of children who were previously diagnosed by a physician and were registered in the Mental Health Center in Duhok city. The patients were included in a 1-month art-based intervention course and were followed up by 1 month. The patients received the art-based intervention 2 hours per day for 3 days/wk. To recruit the patients, we contacted the Mental Health Center in Duhok city. Patients who are diagnosed with mental disorders are referred to this center for the next medical care and follow-up. In this regard, the center has all patients who were diagnosed with ASD across the Duhok governorate. We checked the medical records of the patients with ASD for the eligibility criteria. The children who were diagnosed with ASD and met the eligibility criteria were separated and others were crossed accordingly. We found that 56 children met the initial eligibility criteria of the total 125 patients with ASD. The children with ASD levels 2 and 3 met the initial eligibility criteria in this study. The center then contacted the parents of the patients. Of the total 56 patients with ASD, the parents of 28 children accepted to take part in this study. Out of 28 children, the parents of 15 children registered for the course on the first day. The remaining 13 children did not register for the course owing to unknown reasons. We determined the dates and times of the course at a meeting before the course. We presented 11 two-hour sessions to the children within a month. In session 12, we conducted an exhibition of the artworks made by the children. The parents of the children participated in the art course as well.
2. Study setting and intervention area
The children who were included in this study were recruited from the Mental Health Center in Duhok city. This center has been established to provide diagnostic and therapeutic care to children with psychiatric disorders in the Duhok governorate. In addition, this center presents some psychiatric and psychological interventions to the children. The Mental Health Center is the only center for the provision of psychiatric health to children. The Duhok General Directorate of Health administers the center. A convenient calm and large hall was devoted by the center for the art-based intervention. The hall was located on the second floor of the Mental Health Center. It was a calm hall afar from the victors of the center.
3. Diagnosis of autism
We included ASD children with levels 2 and 3 in this study. The patients with ASD level 2 require substantial support and have more evident verbal and social communication issues compared to those children with ASD level 1. Also, these patients have difficulties changing their concentrations from one activity to another one. These children have very narrow interests and engage in repetitive behaviors leading to difficulty in function in certain states and tend to speak in sentences and struggle with nonverbal forms of communication.
ASD children with level 3 need very substantial support. ASD level 3 is considered the most severe form of autism and has many same behaviors as levels 1 and 2. Despite these children expressing themselves verbally and nonverbally, they have difficulties functioning, interacting socially, and deal with a change in focus or location, and engaging in repetitive behaviors. They have too many limitations to speak evidently. They start interacting with other people and speak so awkwardly. Also, they respond to only very direct social approaches from other people [11]. The ASD level was detected from the medical records of the patients and their parents.
4. Inclusion and exclusion criteria
We included ASD with any type in this study. The ASD types were autistic disorder, Asperser syndrome, pervasive developmental disorders (PDD-NOS [not otherwise specified]), Rett syndrome, and childhood disintegrative disorder. We included both genders in this study. The patients with other severe mental disorders that made difficulty in communication were not included in the study. Also, we included patients from different sociodemographic characteristics.
5. Art therapy intervention
We provided some art-based templates to the children in each session. The templates were different for each session to avoid boredom amongst the children. We presented some of these templates in Fig. 1. In one of these templates, there were 3 different size squares on the bottom page. On the top side of the paper, there were 3 empty squares the same as size the bottom squares. We asked the children to cut the squares and locate them in the suitable empty squares and stick them on the paper. This template was repeated with triangles in another session. In another template, there were 2 colorful bees on the top side of the paper. The bees were not colored on the bottom side of the paper. We asked the children to color the black-and-white images. Also, we gave a template of a black-and-white house to color as they like. We gave the required wooden pen colors to the children to color the house and other templates as required. In another assignment, there were one colorful square, one circle, and one trainable. There were some noncolored triangles, squares, and circles on the bottom side of the paper. We asked the children to color the same as the color of the triangles, circles, and squares. This assignment helped the children to search for the colors and recognize them for use in convenient places. Apart from these templates, we gave some wooden handwork to the children to play with them during the course. We gave some templates to the parents of the children to repeat the art-working at home (Fig. 1).
A sample of templates given to children with autism in the art-based intervention.
During the art-based intervention, the children used a pen (wooden and aquatic) and scissors for performing these activities. The children were trained on how to keep and use the pen and scissors taking into account safety considerations. Some of these activities were shown in Figs. 2 and 3.
A sample of tasks given to children with autism during the art-based intervention.
Images of children with autism completing the art-based intervention.
In the course, 1 artist and 1 psychologist helped the intervenor in this study. We trained these 2 persons on how to help the intervenor during the course because controlling the ASD children without help is not possible especially since we included the ASD children with levels 2 and 3 only. Also, the parents of the children assisted the intervenor and trainer in controlling the children in the course because a few children did not follow the instructions of the intervenor. The trainers were the staff of the Mental Health Center and had 5 and 8 years experience of working with children in the center. The art-based intervention was performed between September 14, 2019, and October 7, 2019, in Duhok city. Community involvement: not applicable
6. Techniques of bias reduction
We tried to include a representative sample of the ASD population from this region. In this regard, we asked the center to call all eligible parents of the children. In addition, only 1 researcher with the cooperation of 2 trainers applied the intervention and the outcomes were measured by another researcher. In terms of the allocation bias, we had not any problem because we did not include any control group in this study. Also, we did not have any family with 2 or more children with ASD in this study.
7. Measurement criteria
We recorded the children’s information in a predesigned questionnaire. The general information was recorded in the first part of the questionnaire. The general information was age, sex, sleeping hours, current disease, medicine use, parents’ education, and the number of family members. The autism severity items were recorded in the second part of the questionnaire.
8. Autistic symptomatology
The symptoms were measured using the parent version of the Social Responsiveness Scale (SRS)-2. The SRS-2 has 65 items for the measurement of ASD severity. The scale emphasizes social impairment the items are rated from 0 to 4 and added together to obtain the overall score. The scale measures 5 subscales including social motivation, social cognition, social awareness, social communication, and repetitive behavior) [12]. The scale is used for children with ASD and general pupations. The scale can be filled out by a parent, teacher, spouse, or another adult informant. The scale measures the children with natural social context and reflects what has been consistently observed over weeks or months. The scale measures the severity of autistic traits and symptoms, and distinguishes ASD from other psychiatric conditions. Higher total and subscale scores indicated worse severity of social impairments.
Each question on this scale rates the severity of behaviors rated on a 4-point Likert scale as not true, sometimes true, often true, and almost always true for children aged 4 to 18 years. The subscales of this scale are:
(1) Social awareness: Social awareness is defined as the ability to pick up on social assignments. The following items are included in the social awareness are the sensory aspects of reciprocal social behavior.
(2) Social cognition: Social cognition is defined as the ability to analyze social missions. The following items are included in social cognition; the cognitive-interpretive aspects of reciprocal social behavior.
(3) Social communication: Social communication is defined as expressive social communication and reflects the motoric aspects of reciprocal social behavior.
(4) Social motivation: Social motivation is defined as the extent to which a person is generally motivated to engage in social-interpersonal behavior. Social motivation presents elements of social anxiety, inhibition, and empathic orientation is included among these items.
(5) Autistic mannerisms: Autistic mannerisms are defined as stereotypical behaviors or highly restricted interests characteristic of autism [13].
9. Statistical analysis
The general characteristic of the children was presented in descriptive statistics. The uncertainty was determined in a 95% confidence interval (CI). The comparisons of ASD severity and its subscales between pre and postcourse in children were examined in a Wilcoxon signed-rank test. The difference between pre and postcourse was determined by mean difference and 95% CI. The null hypothesis was rejected in a P<0.05. The statistical calculations were performed in JMP Pro 14.3.0 (https://www.jmp.com/en_us/home.html).
10. Ethical statement
We obtained ethical approval from the Duhok General Directorate of Health in Duhok city in 2018. The written consent forms were obtained from the parents of the children before inclusion in the course. The participants had the right to reject the participation to leave the course whenever they way. The art-based intervention had not any risk to the children. The protocol of this study was registered on 12th March, 2019 as the reference number 12032019-2 by the Scientific Research Divison, Department of Planning of Duhok Directorate General of Health in Duhok city.
Results
The mean age of the patients was 8.15 (standard deviation, 1.95) aged 5 and 11 years old. Most patients were males (11, 84.62%). The patients slept between 8 and 11 years. Three patients had epilepsy and only 2 patients used medicines. The educations of mothers and fathers were most in under high school and college. The patients had family members between 4 and 16 people (Table 1).
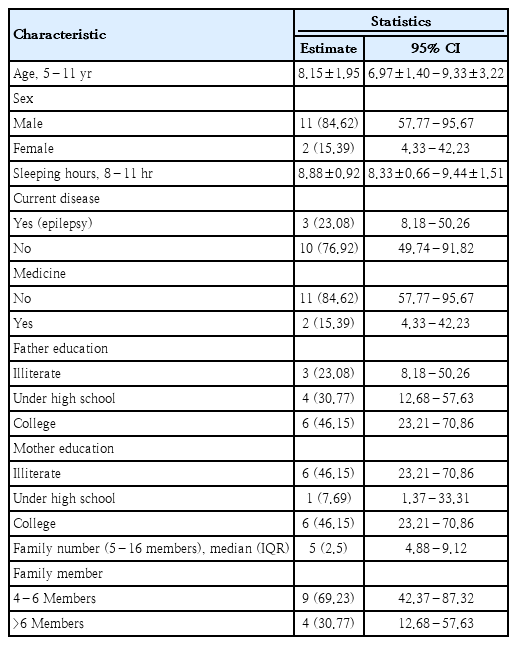
General characteristics of children with autism spectrum disorders (n=13)
The study showed that the mean score of autism was not changed significantly from pre to postcourse (159 vs. 157; mean diff [95% CI], -3.38 [-15.74 to 8.97]; P=0.601). Similarly, we did not find any significant change in social awareness (19 vs. 19, P=0.779); social cognition (28 vs. 27; P=0.1992); social communication (56 vs. 54, P=0.600); social motivation (26 vs. 24, P=0.684), and autistic mannerisms (33 vs. 32, P=0.780), respectively (Table 2, Fig. 4).
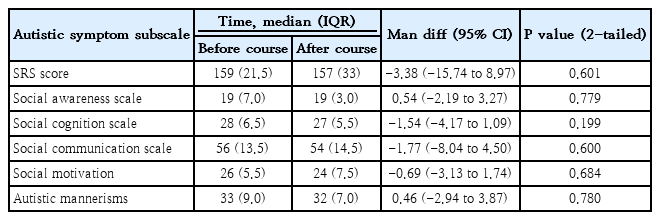
Autism symptomatology and subscale scores before and after the art-based intervention (n=13)
Pre- and postintervention comparisons of total autistic symptomatology score (A) and autistic symptom subscales (B). SRS, Social Responsiveness Scale
Discussion
This study showed that art-based intervention was not effective in improving autism symptoms and social skills (social awareness, social cognition, social communication, social motivation, and autistic mannerisms) among children with ASD levels 2 and 3 after one month. Children diagnosed with ASD have qualitative limitations in social communication skills. They often have stereotypic and repetitive patterns in behavior, interests, and activities [14]. In the literature, there is no consensus on the effectiveness of art-based interventions on symptoms in children with ASD. For example, a systematic review of 18 descriptive studies identified the main elements of art therapy for children up to 18 years. The systematic review reported that art therapy could be effective in assisting a more flexible and relaxed perception, improved communication and learning skills, and better imagination in ASD children. The study reported that the art therapy may reduce social communicative issues and restricted and repetitive behavior patterns. Also, they found that typical art therapeutic elements (e.g., sensory experiences with sight and touch) improve social behavior, flexibility, and attention abilities of children with ASD [8]. In another attempt, the researchers showed that drawing is an effective technique to improve participants’ cognitive, social, and motor skills [15].
It seems that the art establishes a unique bridge for a relationship between ASD children and the world. Emery [16] suggested that creative art-making activities help children with ASD to be mindful of themselves and to make an association with their environment because the children observe, recognize, and find out the world as observed in their art. In the art-based interventions, the children choose their favorite materials and take part in the artworks leading to the expression of their thoughts and feelings. But in this study, we selected the materials for the children because ASD children with levels 2 and 3 were unable to choose their favorite art materials. Koo and Thomas [15] claimed that basic anticipation from an art therapy or art-based intervention could be an improvement in motor skills and sensory integration through media and different art creative activities. Also, the improvement in motor skills can be occurred by using coping skills, and eye-hand coordination in art activities like tearing, cutting, drawing, and touching new materials. The activities made for the sensory aspects of humans are effective in managing and adjusting new materials and reducing oversensitivity to the world. Gabriels [17] approved that learning motor coordination is considered the preliminary step to taking part in a multistep project and art group activities. The longer art-based sessions may help the children to establish a better relationship with autistic children in the environment because an intensive short course may not provide sufficient opportunities for the children to make this kind of relationship and experience their senses for better communication.
Lee et al. [18] applied for an art program on two 6-year-old children with ASD in an educational setting. They provided opportunities for the children to raise their social communication skills through a behavior-analytic instructional methodology once a week for 17 sessions. They reported that the art intervention facilitated the children’s expression of their own emotions and social interactions with each other during the art sessions. An analysis of the findings of the study claimed that the children learn on how to use images as a means of communication (creating), to present their artwork in the classroom (presenting), to describe their works (responding), and to associate themselves to others and their surrounding environment (relating).
In this study, we tried to avoid measurement bias as much as possible. The art-based intervention and measures of outcomes were performed by 2 independent researchers. But the outcomes reported in this study may not be comparable to the findings reported in other studies because we included ASD children with levels 2 and 3 in this study. Other studies have not reported the severity of ASD. Also, we did not include an art therapist in this study as our region has no art therapist. Also, the majority of the patients who were included in this study were males because boys are at higher risk for autism compared to girls [19].
We could not include an art therapist in this study, but we recommend other researchers include an art therapist as much as possible. Also, we recommend longer and more sessions of art-working for the children because an intensive and short art-based intervention may not be adequate to improve the autism symptoms among children. We recommend the role of familybased art therapies on symptoms in patients with ASD for the next attempts. There were insufficient studies on family-based art therapy in the literature [20].
In conclusion, this study showed that art-based intervention is not an effective technique to improve autism symptoms and social interactions (social awareness, social cognition, social communication, social motivation, and autistic mannerisms) among children with ASD levels 2 and 3. We recommend more sessions of art-based interventions for a longer period for the improvement of symptoms and social interactions for children with ASD.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study was funded by the Duhok General Directorate of Health as a health promotion activity for children with autism spectrum disorders.
Author Contribution
Conceptualization: DMA, BMA; Formal analysis: DMA, PL; Funding acquisition: BMA; Methodology: DMA; Project administration: DMA; Visualization: DMA, BMA; Writing-original draft: DMA; Writing- review & editing: BMA, PL
Acknowledgements
The authors of this study would like to present their deep thanks to the Mental Health Center and Duhok General Directorate of Health in Duhok city, specifically Dr Nezar Ismet Taib who agreed to fund this project. In addition, we would like to give our deep gratitude to the parents of the children.