Kidney complications associated with COVID-19 infection and vaccination in children and adolescents: a brief review
Article information

See the letter "Clinical considerations and practical issues of kidney complications in children after COVID-19 infection or vaccination" on page 35.
Abstract
Coronavirus disease 2019 (COVID-19) has spread considerably across the globe, affecting numerous children and adolescents besides adults. Despite its relatively lower incidence rates in children and adolescents than in adults, some infected children and adolescents exhibit a severe postinflammatory response known as multisystem inflammatory syndrome in children, followed by acute kidney injury, a common complication. Meanwhile, few reports have been available regarding kidney complications such as idiopathic nephrotic syndrome and other glomerulopathies associated with COVID-19 infection and vaccination in children and adolescents. However, the morbidity and mortality of these complications are not exceptionally high; more importantly, causality has yet to be clearly established. Finally, vaccine hesitancy in these age groups should be addressed, considering the strong evidence of COVID-19 vaccine safety and efficacy.
Key message
Several observational studies have shown that acute kidney injury affects up to 46% of children and adolescents who develop severe postinflammatory responses, such as multisystem inflammatory syndrome in childhood, due to coronavirus disease 2019 (COVID-19). Although causality has not been established, some cases of glomerulopathy or nephrotic syndrome occurring after COVID-19 infection or vaccination have been reported. Therefore, kidney complications associated with these conditions in children and adolescents warrant attention.
Graphic Abstract. Kidney complications associated with coronavirus disease 2019 (COVID-19) infection and vaccination in children and adolescents. MIS-C, multisystem inflammatory syndrome in children; PIMS-TS, pediatric inflammatory multisystem syndrome temporally associated with COVID-19; AKI, acute kidney injury; GN, glomerulonephritis; IgAN, immunoglobulin A nephropathy; ATIN, acute tubulointerstitial nephritis; NS, nephrotic syndrome; MCD, minimal change disease.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has affected millions worldwide, including children and adolescents. Although most infected children experience mild to moderate symptoms or remain asymptomatic, some exhibit a severe postinflammatory response known as multisystem inflammatory syndrome in children (MIS-C) or pediatric inflammatory multisystem syndrome temporally associated with COVID-19 [1]. This condition reportedly occurs within 2–6 weeks after COVID-19 infection or exposure to an infected person and is characterized by persistent fever, inflammation, and dysfunction of multiple organs, including the heart, kidneys, and lungs. Despite the relatively lower incidence rate of MIS-C (1 of every approximately 3,000–4,000) than that of COVID-19 in adults and its risk of mortality and serious complications, it requires immediate recognition and management [1-6].
Since the beginning of the pandemic, reports have shown that acute kidney injury (AKI) in children with MIS-C or critically ill children requiring hospitalization is significantly associated with intensive care unit (ICU) admission [7,8]. Furthermore, several studies reported other kidney complications, including idiopathic nephrotic syndrome (INS) and various types of glomerulonephritis (GN), in populations with COVID-19 who received the vaccination [9]. Understanding the epidemiology and pathophysiology of AKI and other kidney complications in relation to COVID-19 infection and vaccination can aid the establishment of treatment strategies and improve clinical outcomes.
This review provided a brief overview of our current understanding of the epidemiology, pathogenesis, and clinical characteristics of AKI, nephrotic syndrome, and GN in children and adolescents who experienced COVID-19 infection and received vaccination.
Kidney complications associated with COVID-19 infection in children and adolescents
1. Acute kidney injury
The Kidney Disease: Improving Global Outcomes defines AKI as one or more of the following criteria: increase in serum creatinine by ≥0.3 mg/dL within 48 hours, increase in serum creatinine to ≥1.5 times the baseline value within the preceding 7 days, or a urine volume of ≤0.5 mL/kg/hr for 6 hours [10].
The pathogenesis of COVID-19-associated AKI is multifactorial. First, the virus binds to the angiotensin-converting enzyme 2 receptors distributed across the proximal tubules, podocytes, epithelial cells, and endothelial cells of the kidneys, subsequently causing direct cell damage, resulting in glomerular collapse, endothelial damage, coagulopathy, and complement activation, leading to AKI. In addition, systemic consequences of viral infection, such as cytokine release, hypovolemia, ischemia, or iatrogenic nephrotoxin exposure, or the presence of viruses in distant organs such as the lungs (i.e., lung-kidney cross-talk) can indirectly cause AKI [1,11].
Studies in adults reported that AKI affects more than 20% of hospitalized patients with COVID-19 and more than 50% of ICU patients [11]. Moreover, several observational studies of various sizes conducted from the beginning of the pandemic reported AKI incidence rates as high as approximately 11%–46% in children and adolescents with COVID-19 who are critically ill or developed MIS-C, similar to those observed in adults [8,12-20]. In contrast, only a few studies reported the incidence of AKI in those with mild to moderate COVID-19. A multicenter cross-sectional study conducted in Turkey reported incidence rates of 16.9% for AKI and 31% for subclinical AKI. Subclinical AKI was defined when at least one of 3 urine biomarkers—neutrophil gelatinase-associated lipocalin, kidney injury molecule-1, and interleukin-18—was positive without an elevated serum creatinine level [21].
A small number of systematic reviews and meta-analyses recently reported the pooled incidence of AKI as 20%–30% in children and adolescents with severe COVID-19 infection such as MIS-C or ICU admission [22,23]. In a meta-analysis by Tripathi et al. [22], the pooled proportion of death in children with MIS-C was approximately 4% (95% confidence interval [CI], 1%–14%), whereas MIS-C patients with AKI had a 4.68 (95% CI, 1.06%–20.7%) higher odds of death than those without AKI. Moreover, evidence suggests that nearly 15% (95% CI, 4%–42%) of AKI patients with MIS-C require renal replacement therapy (RRT). In contrast, a meta-analysis by Raina et al. [23] revealed that the mortality rate of ICU children with COVID-19 was 2.55% (95 % CI, 1.67%–3.73%) and that the pooled proportion of AKI patients requiring RRT was 0.56% (95% CI, 0.16%–1.43%), significantly lower than that reported by Tripathi et al. [22].
AKI associated with COVID-19 was diagnosed in the early stages of hospitalization in most patients, and they were reportedly infected with COVID-19 approximately 33 days (27.5– 46 days) before ICU admission. This appears consistent with reports that MIS-C develops a mean 2–6 weeks after infection with COVID-19. In addition, children with AKI have significantly lower serum albumin levels and higher white blood cell counts than those without AKI at admission [6,14,18].
A large-scale retrospective study (n=2,546) conducted on pediatric ICU inpatients in North America found that COVID-19 patients with AKI had a 6.29-day (95% CI, 3.95–8.64) longer length of hospital stay, 2.69 times greater odds for mortality (95% CI, 1.48–4.88), and 5.34 times greater odds for kidney support (95% CI, 2.15–13.25) than COVID-19 patients without AKI [24]. Therefore, evidence suggests that AKI after COVID-19 infection in children should be considered a major risk factor for increased severity and mortality.
Table 1 summarizes the major observational studies to date of AKI development in children and adolescents with COVID-19.
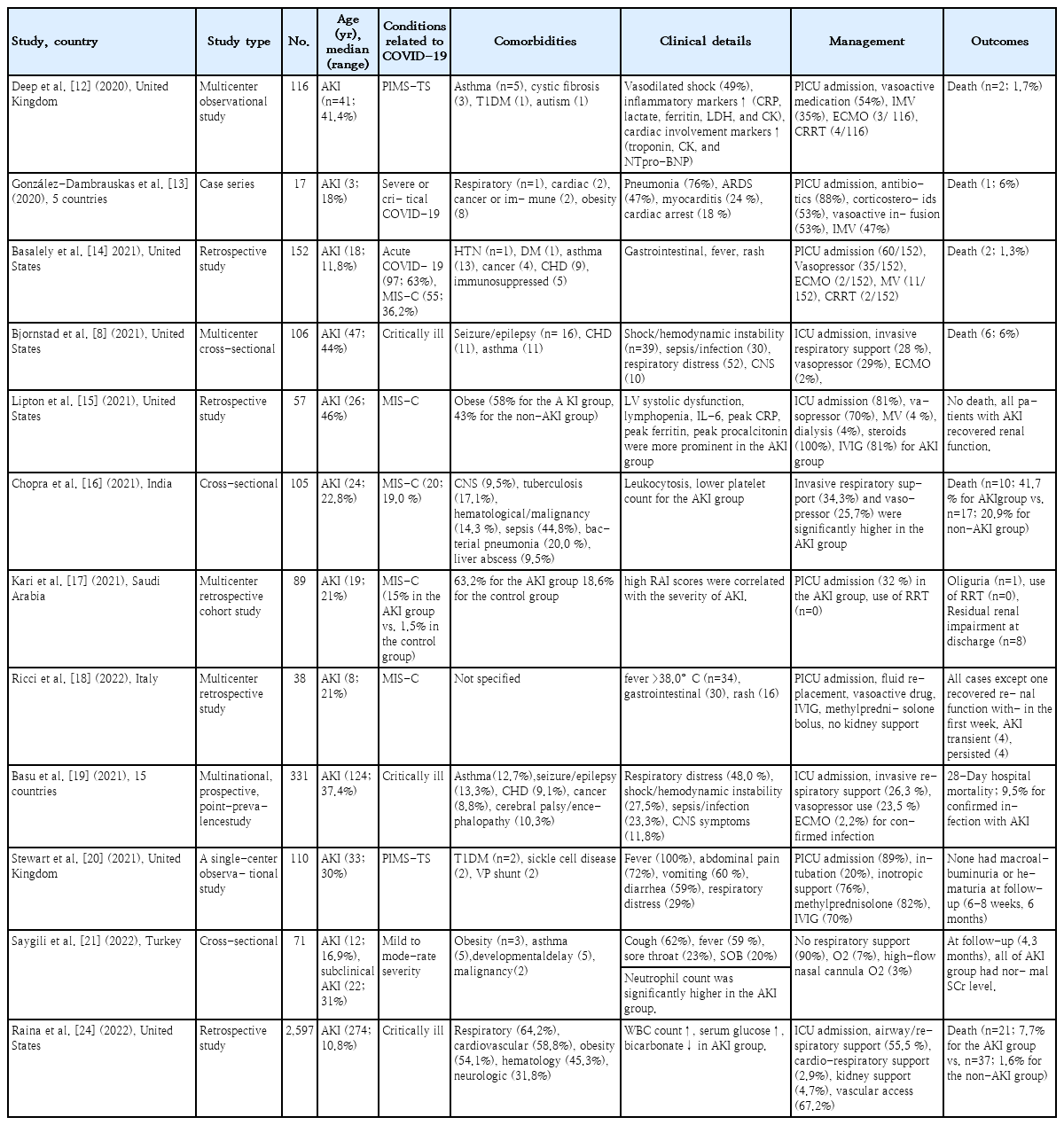
Summary of studies of AKI development in children and adolescents with COVID-19 infection
2. Idiopathic nephrotic syndrome
INS in children is defined as nephrotic-range proteinuria (≥40 mg/m2/hr or a urine protein/creatinine ratio of ≥2 or 3+ protein on a urine dipstick) of unknown etiology plus hypoalbuminemia, edema, or hyperlipidemia [25]. Most children with INS receive chronic immunosuppressive therapy to control the disease activity, which is known to increase the risk of infectious diseases including viral infections [26].
Morello et al. [26] conducted a systematic review of COVID-19 cases in children with INS. In this comprehensive review of 13 studies (43 children with COVID-19 of 1,126 children with INS) children with INS did not have a particularly high COVID-19 infection rate. Moreover, despite COVID-19 infection, they generally showed a mild clinical course, with low ICU hospitalization rates and a need for respiratory support. They also recommended that immunosuppressive therapy be continued regardless of the pandemic situation. In addition, despite the few cases of INS relapse during the COVID-19 infection period (n=5), they showed a good response to steroids, even de novo cases (n=2) showing typical symptoms and clinical improvement with steroid treatment.
A recent retrospective study of 59 pediatric INS patients from a single center in Korea reported that 20 were infected with COVID-19 during the study period (34%). Consistent with other studies, this study showed that all patients had mild clinical symptoms that improved with symptomatic treatment comprising antipyretic or cold medications and did not require hospitalization or antiviral therapy. Furthermore, the relapse rate among INS patients with COVID-19 (3 of 20 [15%]) did not differ significantly from that of INS patients without COVID-19 (8 of 39 [20.5%]) [27].
Chiodini et al. [28] performed a retrospective cohort analysis of 218 children with INS in Belgium and Italy. Comparison of the relapse rate between the 5 years immediately preceding the COVID-19 outbreak (i.e., 2015–2019) and the first year of the outbreak (i.e., 2020) showed no statistically significant difference, with an incidence rate ratio of 0.9 (95% CI, 0.76–1.06). Moreover, no severe complications among the study participants, such as death or hospitalization due to COVID-19, were reported.
Morello et al. [29] retrospectively analyzed a cohort of 176 children with INS from the beginning of the pandemic to May 31, 2022. A total of 61 (34.7%) were infected with COVID-19 during the study period. After the spread of the omicron variant, children with INS showed a significantly higher COVID-19 infection rate than previously reported. However, the clinical symptoms were mild in children with INS taking immunosuppressive medication or had proteinuria. Moreover, none of the patients required immunosuppressive therapy discontinuation due to the COVID-19 infection.
3. Glomerulopathy
In adults with COVID-19, several pathological findings of kidney biopsies, such as podocytopathies (collapsing glomerulopathies), immune-mediated glomerular diseases (membranous glomerulopathy), tubulointerstitial diseases (acute tubular injury), and thrombotic microangiopathy, have been reported [1,30,31]. In contrast, pathological data in children and adolescents are lacking [32].
A recent case report showed that a previously healthy 11-year-old boy hospitalized with gross hematuria and generalized edema 2 weeks after contracting the COVID-19 infection in Korea was diagnosed with crescentic immune-complex GN through a kidney biopsy. Steroid therapy, immunosuppressants, including cyclophosphamide and azathioprine, and antihypertensive treatment clinically improved his condition [33].
Another case study reported on 2 patients (13- and 16-year-old boys) who developed severe, rapidly progressive GN and end-stage renal disease after COVID-19 in India. A kidney biopsy confirmed immunoglobulin A (IgA) nephropathy with crescentic GN, acute tubular injury, and focal medium-artery vasculitis [34].
In Italy, 2 consecutive renal biopsies were performed in a 10-year-old girl after a COVID-19 infection; the first revealed diffuse and segmental mesangial-proliferative GN, while the second revealed crescentic GN. The same case study also confirmed acute tubulointerstitial nephritis (TIN) through a kidney biopsy in a 12-year-old girl infected with COVID-19 [32].
Furthermore, case reports showed the presence of acute necrotizing GN in 17- and 16-year-old boys infected with COVID-19 in Iran, whereas another report from the United States showed the presence of necrotizing GN in a 17-year-old boy with perinuclear antineutrophil cytoplasmic antibodies/myeloperoxidase vasculitis [35,36].
Kidney complications associated with COVID-19 vaccination in children and adolescents
Research has demonstrated the safety and efficacy of COVID-19 vaccines (Pfizer-BioNTech BNT162b2 and Moderna mRNA-1273) in children and adolescents, and the eligibility age for vaccination has been gradually expanded. Since June 2022, vaccination has become available for infants over 6 months of age. A well-known side effect of vaccination is the increased risk of myocarditis and pericarditis after the second dose in young men aged 12–24 years. However, most of these patients improved with conservative treatment, and the condition had no significant impact on their quality of life [37]. In contrast, several cases of renal side effects, such as minimal change disease (MCD), IgA nephropathy (IgAN), and vasculitis, have been reported after vaccination in adults. Nevertheless, causality has yet to be clearly established, with large population-based observational studies suggesting no increase in the risk of occurrence [9].
Novel mRNA vaccines for SARS-CoV-2, including BNT162B2 (Pfizer), are based on an mRNA lipid nanoparticle-encapsulated platform and induce a stronger cell-mediated response by upregulating CD4+ and CD8+ T cells. Therefore, studies have suggested that the pathogenic mechanism involves the sequential production of proinflammatory cytokines, such as interferon-γ and tumor necrosis factor-α, which can exacerbate existing immune-mediated glomerular disease or cause de novo GN, including IgAN [38-40].
In developed countries such as the United States and Japan, the eligibility age for COVID-19 vaccination, especially the Pfizer-BioNTech vaccine, has gradually expanded to include those aged 16+ years (December 2020), 12–15 years (May 2021), 5–11 years (October 2021), and 6 months to 4 years (June 2022). Therefore, case reports on kidney side effects in children and adolescents have been reported mainly in these countries and adolescents aged 12+ years with de novo or relapsed forms of glomerular disease (primarily IgAN and INS). Cases of IgAN mainly occurred de novo within 1–2 days after the second dose of the Pfizer-BioNTech vaccine, manifesting as gross hematuria and proteinuria of varying degrees. In most cases, the symptoms improved with intravenous/oral steroid therapy, angiotensin receptor blockers, and supportive care [39-45].
In contrast to cases of IgAN, there have been cases in which kidney failure and oliguria were severe enough to require hemodialysis. A case report of a 16-year-old girl in Korea showed a relatively long interval between vaccination and symptom onset. She experienced nonspecific symptoms, such as respiratory distress and headache, for 6 weeks after receiving her second dose of the vaccine and was diagnosed with crescentic GN through a kidney biopsy after receiving hemodialysis for acute kidney failure [46]. In Luxembourg, a case of rapidly progressive GN was reported; a 13-year-old girl developed systemic symptoms, including gross hematuria, just 1 d after the first dose of the vaccine and rapidly progressed to AKI, requiring hemodialysis [47].
Among patients with INS, most had a de novo occurrence than a relapse, and the interval between vaccination and symptom onset was 1–19 days. MCD was the main pathological finding in patients who underwent kidney biopsy, all of whom responded well to steroid treatment [48-52]. On the other hand, 2 reports showed cases of new-onset acute TIN after the second vaccination in Korea that reportedly responded well to oral steroid treatment (a 12-year-old boy) and supportive care (a 17-year-old boy) [53].
Several case reports of kidney complications, such as IgAN and INS after COVID-19 vaccination in children and adolescents are summarized in Table 2.
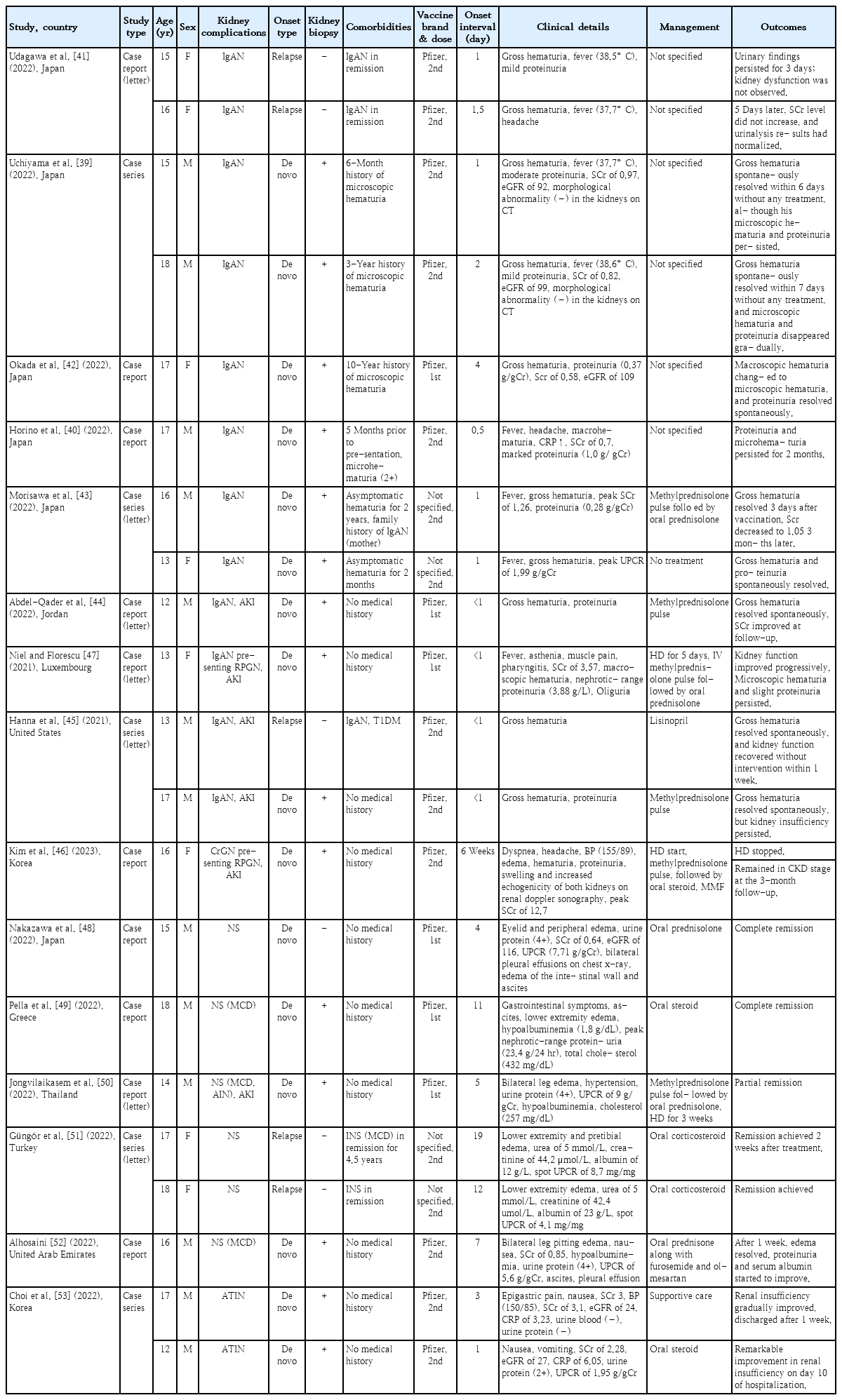
Summary of studies of kidney complications in children and adolescents with COVID-19 vaccination
Management of kidney complications and vaccine hesitancy in children and adolescents with COVID-19
Children and adolescents hospitalized with COVID-19 are at a high risk of developing AKI regardless of disease severity, thereby increasing their morbidity and mortality. In fact, evidence has shown that kidney disease in childhood and adolescence significantly impacted long-term outcomes, such as adult health status, social and behavioral adjustment, educational success, and employment security [1,54]. Therefore, the medical staff caring for these patients should pay special attention to their respiratory and systemic symptoms besides their urinary symptoms and kidney function. If AKI or other kidney complications are diagnosed, a referral to a pediatric nephrologist for active treatment is recommended.
Despite strong evidence of the safety and effectiveness of COVID-19 vaccines, hesitancy remains widespread [55,56]. Wang et al. [57] analyzed vaccine hesitancy and current attitudes toward vaccines among parents of children with chronic kidney disease (n=207). Accordingly, approximately two-thirds of parents were hesitant or unsure about vaccinating their children, and parents with higher education levels were more willing to vaccinate their children. The main reasons for vaccine hesitancy were concerns about vaccine safety, a lack of sufficient information, and a lack of communication with medical experts. Therefore, medical professionals who frequently interact with parents must provide consistent and standardized COVID-19 vaccination information tailored to the parents’ level of understanding and maintain consistent communication to increase the COVID-19 vaccination rate.
Conclusion
The current review briefly examined the existing literature on kidney complications reportedly associated with COVID-19 infection and vaccination. A high incidence of AKI is shown in children and adolescents diagnosed with MIS-C or are critically ill because of infection, similar to that in adults. However, INS and other glomerulopathies did not appear to have particularly high morbidity or mortality rates. Vaccine hesitancy in these age groups should be addressed through consistent communication with the parents or guardians based on strong evidence regarding the safety and efficacy of COVID-19 vaccines.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.