Environmental changes surrounding congenital heart disease
Article information

Abstract
As the outcomes of patients with congenital heart disease (CHD) improve, the number of patients is accumulating and the proportion of adult CHD patients is gradually increasing. Accordingly, the proportion of typical adult diseases such as coronary arterial disease, diabetes, dyslipidemia, and hypertension among patients with CHD is increasing, as is the medical burden due to residual cardiac problems, heart failure, and arrhythmias. Due to increasing genetic knowledge, efforts are being made to provide active medical support through risk stratification. Surgical techniques and prostheses are also developing, the instruments used for transcatheter intervention are diversifying, and the range of therapeutic options is expanding. In addition, owing to the development of electronic devices, heart rhythm and blood pressure monitoring instruments have been miniaturized and diversified. In this process, a vast amount of information is collected; therefore, the current systematic review examined their clinical usefulness. A team approach consisting of experts from various fields is essential for the treatment of patients with CHD and advanced heart failure.
Key message
· As the number of patients with congenital heart disease increases, the medical burden increases.
· Various fusion imaging techniques using percutaneous procedures have been introduced.
· With advances in technology, convenient ambulatory devices have been introduced.
· A well-organized team approach is required to resolve advanced heart failure in patients with congenital heart disease.
Graphical abstract.
Introduction
Congenital heart disease (CHD) is the most common cause of major congenital anomalies and represents a major global heart problem [1,2]. In recent decades, thanks to advances in perinatal diagnosis, improvements in imaging quality, diversification of surgical techniques, various mechanical devices and drugs, and surprising changes in percutaneous transcatheter intervention, the number of patients with CHD is gradually increasing. Jang et al. [3] reported that the prevalence of CHD in Korean adults increased from 35.8 cases per 100,000 persons in 2006 to 65.6 cases per 100,000 persons in 2015 using the National Health Insurance Service in Korea, while the mortality rate decreased. In Korea, the number of newborn CHD patients is also decreasing due to the markedly low fertility rate, whereas the number of patients with CHD, whose survival rate has increased due to improved treatment, is accumulating and the number of adults with newly discovered CHD due to the increase in healthcare and imaging quality is also increasing [4].
Owing to these changes surrounding CHD, the medical care required for it is also changing as the affected patient group is not limited to newborns but extends to adolescents and adults. Most people would agree that CHD is by far the most commonly treated disease by pediatric cardiologists. However, as the proportion of adult patients with CHD increases, new medical staff and services are needed to adequately treat them. Therefore, this review examined how the underlying environment of CHD is changing.
Increasing CHD population and medical burden
One of the largest changes in CHD is its affected population. Individuals with CHD are still being born today, but in the case of Korea, the number is decreasing naturally, as the country is recording an unprecedented low birth rate. The number of newborn babies in Korea has decreased rapidly from 640,089 in 2000 to 470,171 in 2010 and 272,337 in 2020 (https://index.go.kr). However, outcomes of CHD are gradually improving [5], and as the number of patients undergoing surgery or transcatheter intervention is increasing, overall patient numbers and ages are gradually increasing. Moreover, due to increased interest in cardiovascular health, the generalization of ultrasound examinations, and improvements in image quality, CHD such as small atrial septal defect (ASD), partial anomalous pulmonary venous return, congenitally corrected transposition of the great arteries, and mild Ebstein anomaly, which were not previously detected, are increasing in adults, so the overall age of CHD patients is increasing [6,7]. Some patients require reoperation or other interventional procedures among those who have already been treated.
As the number of cases requiring additional treatment for problems such as arrhythmia or heart failure (HF) increases, the proportion of adult CHD (ACHD) cases is rapidly increasing beyond expectations. Since adult patients with CHD have many comorbidities, it is natural that the medical burden they occupy in the medical field increases [8,9]. In the early 2000s, the number of patients with grown up CHD (GUCH) in Europe began to exceed that of pediatric CHD patients [10]. Since 2015, adults have accounted for more than 2/3 of all CHD patients [11,12]. According to data released by the Korea Heart Foundation (https://www.heart.or.kr), percutaneous ASD occlusion, a representative percutaneous procedure, increased from 27 cases in 2000 in Korea to 722 cases in 2010 and 946 cases in 2020. Medical insurance coverage underlies this change, but an increase in the proportion of adult patients is also a factor. In Korea, as the number of GUCH patients increases, personnel who can care for them are increasingly lacking. According to Jang et al. [3], the number of ACHD patients in Korea in 2015 reached approximately 34,000. Pediatric cardiologists may lack an understanding of the medical needs and comorbidities of adults, while adult cardiologists are likely to no understand CHD itself. Therefore, the training of such professional manpower is an urgent task.
Increasing redo operations
A large number of CHD patients undergo surgical treatment during their neonatal and infancy years. However, additional surgery is required if residual defects, valve regurgitation, and stenosis become significant hemodynamic problems during follow-up. For example, if a patient with tetralogy of Fallot (TOF) who underwent thoracotomy in infancy developed HF due to gradual enlargement of the right ventricle due to pulmonary valve regurgitation, pulmonary valve replacement should be performed at an appropriate time. In addition, in these patients, pulmonary valve replacement is required when the lifespan of the pulmonary valve expires (approximately 10– 15 years). Moreover, reoperation is required when the function of the previously operated conduit, artificial valve, or mechanical valve deteriorates or the relative size fails as the patient grows. In a pacemaker-implanted patient, an additional surgical procedure is required for a generator or pacemaker lead change. In other words, since the treatment of CHD consists of care and support rather than cure, continuous medical help is necessary and additional surgery may become required. As such, reoperations are increasing in patients with CHD. Various technical problems related to heart surgery, such as cardiopulmonary bypass machines and ventilators, have greatly improved. However, increased number of surgeries and patient age at surgery increase surgical morbidity and mortality rates.
Advances in genetic knowledge
CHD is the most common birth defect, affecting approximately 1%–1.2% of births. According to epidemiologic studies, genetic or environmental causes are identified in approximately 20%–30% of cases. Among them, gross chromosomal anomalies or aneuploidy account for approximately 8%–10%, singlegene disorders are identified in 3%–5%, and pathogenic copy number variants are identified in 3%–25% of cases. Cases associated with CHD accompanied by a chromosomal abnormality include Down syndrome and Turner syndrome. Examples of CHD associated with specific copy number variants include 22q11.2 deletion syndrome, Williams-Beuren, and Jacobsen syndromes (11q terminal deletion disorder). Diseases caused by a single-gene variation include Alagille syndrome, Holt-Oram syndrome, and CHARGE syndrome.
As the use of new genetic testing techniques such as chromosomal microarray and next-generation sequencing has become increasingly more common, the discovery of new genes related to CHD has accelerated, confirming the correlation between cardiovascular genotype and phenotype. In addition, it is becoming possible to predict cardiovascular features and related medical conditions [13-15]. For example, in CHD patients, despite excellent correction, HF or exercise intolerance occurs more frequently in this versus the general population with age. However, the main reason for this is the genetic interaction between CHD and HF [16].
There is currently limited information available regarding the parameters of ventricular function or long-term outcomes in carriers of causal mutations. However, as more profound genotype-phenotype studies continue in the areas of long QT syndrome or hypertrophic cardiomyopathy, it is possible to achieve greater accuracy predicting recurrence risks and identifying atrisk fetuses. Long QT is classified into 17 subtypes based on mutations associated with 15 autosomal dominant genes. Hypertrophic cardiomyopathy is a heterogeneous disease with variable expressivity and incomplete penetrance, but it is also known as the most disease-causing variant of cardiac β-myosin heavy chain (MYH7) and myosin binding protein C3 (MYBPC3). Recent attempts to utilize it for the risk assessment and prevention of sudden cardiac death with the help of genetic tests have been actively made. Although hypertrophic cardiomyopathy exhibits a wide variety of clinical manifestations, most are closely associated with MYH7 and MYBPC3.
Ultimately, genetic information is crucial for planning care and enabling clinical research. Rare monogenic causes of CHD and HF include Noonan, Williams-Beuren, and 22q11 syndromes. Overlapping molecular pathways between CHD, HF, and cardiomyopathy are often expressed together when there is a genetic mutation such as MYH7, MYH6, or ACTC1 as well as for the MYBPC3 and TNNI3 genes [17]. Their investigation will pave the way for an increased understanding of the development of HF in CHD [18].
Development of transcatheter intervention
It is impossible for cardiac interventions to replace cardiac surgery completely. However, as instruments for percutaneous procedures are diversified and improved, catheter-based interventions are expanding their scope for various diseases and conditions that require surgery. Percutaneous device closure is possible for various defects, such as ASD, ventricular septal defect, patent ductus arteriosus, residual ventricular septal defect leak, and paravalvar leak. In addition to clipping to correct mitral valve regurgitation or tricuspid valve regurgitation [19], it is possible to reduce the annulus [20]. Moreover, percutaneous valve replacement of the aortic valve or pulmonary valve is actively being performed in clinical practice [21].
Although the Pulsta valve (Taewoong Medical Confidential, Seoul, Korea) developed and produced in Korea is in its initial stage, it is preparing to enter the international market [22]. The Pulsta valve is a self-expandable knitted nitinol-wire stent mounted with a treated tri-leaflet α-Gal-free porcine pericardial valve (unlike the Melody valve developed and commercialized first) that can be applied to patients with an enlarged right ventricular outflow tract because it has a usable size of up to 32 mm. Using various stents, it is also possible to widen narrow areas, such as the coarctation of the aorta or branch pulmonary arterial stenosis [23]. Hemodynamic function can be improved through percutaneous occlusion of fistulae or collateral vessels that can unnecessarily cause HF. Even interventions for partial anomalous pulmonary venous return repair [24] or coronary sinus–type ASD closure [25], which are thought to be only possible with surgical treatment, are being attempted; therefore, percutaneous treatment is expected to expand infinitely in the future.
Increased HF and arrhythmias
With aging, coronary artery disease, HF, and arrhythmias increase in adults. In patients with CHD, these diseases also worsen owing to residual defects or valve lesions. In particular, HF and arrhythmia are serious complications that are directly related to mortality in ACHD patients; eventually, a ventricular assist device (VAD) or heart transplant must be considered. HF in newborns or infants with CHD is mostly caused by volume overload associated with shunts or obstructive lesions. However, HF in adults with CHD is associated with functional impairment, neurohormonal activation, and adverse cardiac remodeling and is often associated with right-sided heart disease. Therefore, there is a limit to applying HF management due to traditional left ventricular systolic dysfunction [26,27]. Active efforts are being made to prepare for the increase in the number of GUCH patients and the medical burden due to their HF.
Arrhythmias are the most frequent long-term complications in the CHD population and the leading cause of morbidity and mortality in adulthood [28]. Although some arrhythmias are due to congenitally malformed or displaced conduction systems, they often occur in association with mechanical or hypoxic stress and residual or postoperative sequelae due to hemodynamic abnormalities, so they tend to increase with age. It is easy to predict that most adult patients with CHD and HF will die of pump failure or arrhythmia. Therefore, managing arrhythmias is a critical component of caring for CHD patients with HF [29,30]. The most common symptomatic tachyarrhythmia in postoperative CHD patients is intra-atrial reentrant tachycardia. When these arrhythmias are treated with drugs, more careful attention is required to avoid undesirable side effects such as concomitant bradyarrhythmia, negative inotropic effects, and proarrhythmia effects in patients with repaired CHD and decreased heart function.
Serious ventricular arrhythmias are rare among CHD patients during the first two decades of life; however, in adulthood, ventricular tachycardia and sudden death are serious risks associated with ventriculotomy, TOF, and severe ventricular dysfunction. For example, one-third of patients with corrected TOF develop symptomatic atrial tachycardia by adulthood, 10% develop advanced ventricular arrhythmias, and 5% require pacemaker implantation for surgically acquired atrioventricular block or sinus node dysfunction [2]. Sinus node dysfunction is also a common disorder of CHD in adults that results from isomerism syndromes with absent or dual sinoatrial nodes or direct surgical trauma to an artery during surgical procedures such as the Mustard, Senning, and Fontan procedures [2]. The sudden cardiac death rate in patients with CHD is 25–100 times higher than that in the general population, but this risk stratification itself is very difficult and often does not correspond with actual clinical practice [29]. There are many discussions about the risk of sudden cardiac death associated with arrhythmias in TOF patients, but the relationship between a Fontan patient and systemic right ventricle has not yet been clearly identified.
Surgical techniques for CHD have made remarkable progress in recent decades, but patients with complex cardiac anomalies that cannot be resolved must resort to palliative Fontan surgery. Among them, the proportion of unpredictable complications such as chronic liver disease, protein-losing enteropathy, and arrhythmia is increasing. Protein-losing enteropathy occurs in approximately 5%–15% of Fontan patients, while virtually 100 % of Fontan patients develop clinically silent hepatic fibrosis by adolescence. Up to 40% of Fontan patients have been reported to present with moderate to severe HF [31]. In these cases, Fontan takedown or cardiac transplantation should be prepared before progression to multiorgan failure occurs.
Problems related to pregnancy and childbirth
As CHD patient age increases, a number of new issues are emerging. One is that patients who have been treated for CHD face a new gateway in their lives of pregnancy and childbirth as they reach adulthood. Although pregnancy and childbirth are a natural part of life for healthy people, the pregnancy and delivery process in women with CHD or repaired CHD can cause rapid maternal hemodynamic changes. Because it can affect maternal and fetal health, more careful preparation and help are required than in the general population. Although risk scores such as the Zwangerschap bij Aangeboren HARtAfwijking (Pregnancy in Women With Congenital Heart Disease) (ZAHARA), Cardiac Disease in Pregnancy Study (CARPREG), and modified World Health Organization classification are widely used to predict the risk of pregnancy-related complications, they are thought to have some limitations predicting the actual outcome [32-34]. ZAHARA scores include prior arrhythmia, New York Heart Association (NYHA) functional class III or IV, left heart obstruction, mechanical valve prosthesis, moderate to severe atrioventricular valve regurgitation, cardiac medication before pregnancy, cyanotic heart disease, twin or multiple gestation, and smoking during pregnancy. CARPREG scores included prior cardiac events, NYHA functional class III or IV, left heart obstruction, reduced systemic ventricular systolic function, multiple gestation, smoking, and heparin or warfarin use during pregnancy. Cesarean rather than vaginal delivery is advantageous for mothers in cases of severe HF, an ascending aorta exceeding 45 mm in Marfan patients, or severe aortic valve stenosis, even if pregnancy has been properly maintained. If a woman of childbearing age and CHD wishes to avoid pregnancy, counseling and guidance on appropriate contraceptive methods and spousal education is required. If a CHD patient wishes to become pregnant, a risk assessment is advisable during and after pregnancy through cooperation with a special cardiologist and obstetrician. Genetic counseling and a heritability analysis are also required. Counseling for families expecting a child with CHD and preparing for childbirth in a stable environment are also required of medical staff treating patients with CHD.
Emphasis on exercise therapy
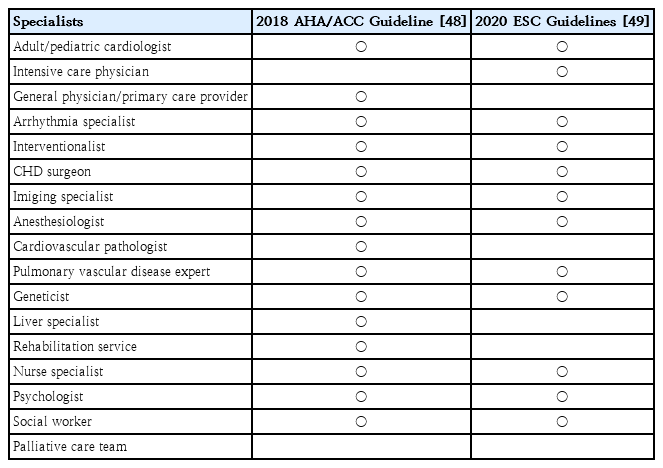
As modern society advances, the physical activity of people decreases and the number of patients with metabolic syndromes, such as obesity, hypertension, and dyslipidemia, is increasing under the adverse conditions of exacerbating malnutrition. Niwa et al. reported that the prevalence of metabolic syndrome in the general population of Japan was approximately 5.5%, whereas that in patients with ACHD was 16% [35]. Therefore, it is necessary to broaden the field of view to health problems other than the heart and manage CHD patients more holistically. Some papers that discuss the requirements of a specialist for ACHD patient management are summarized in Table 1.
Multidisciplinary team for treating adult patients with congenital heart disease
A common opinion is that multidisciplinary experts in CHD are needed; in the long term, palliative care is also needed. Due to this situation, a multidisciplinary team approach is increasingly needed. With the changing trend of increasing interest in quality of health, the importance of daily health care is emerging. In particular, as the importance of exercise in a healthy life is emphasized, many efforts are being made to improve cardiopulmonary function by improving the exercise ability of CHD patients. Data are currently limited regarding whether exercise training can improve outcomes in ACHD-related HF, but it can improve quality of life or self-perception as well as exercise performance [36]. Therefore, it is desirable to increase physical activity through exercise in CHD patients to increase the quality of life and mental health problems of patients with chronic diseases.
In 2020, the European Society of Cardiology (ESC) recommended that adolescent and ACHD patients with CHD be evaluated for ventricular structure and function, pulmonary artery pressure, aorta, arrhythmia, and cyanosis before participating in competitive sports. Subsequently, it was announced that possible exercise types should be recommended after additional observation of changes in the exercise load test process [37]. It is very important that the actual clinical process guides appropriate exercise through this process, even for CHD patients who are not athletes.
It is desirable to prescribe aerobic and resistance exercise training for CHD patients after an appropriate risk assessment [38]. The measured peak oxygen consumption (peak VO2) during peak exercise was described by the Fick equation as a function of cardiac output and the amount of oxygen extracted from the tissue, including the exercising muscle. In fact, since peak VO2 itself is an important predictor of mortality or hospitalization in patients with ACHD [36], it is clinically useful and necessary to predict and manage patient risk through periodic examinations. Predicting the possibility of sinus node dysfunction by monitoring for chronotropic incompetence in which the increase in heart rate during exercise does not reach 85% of the predicted maximum heart rate and checking how quickly the heart rate normalizes after exercise. It is also important to note the chronic and lifelong decline in exercise capacity among CHD patients through regular cardiopulmonary exercise tests and encourage efforts to appropriately improve it rather than exclude activity from daily life.
Introduction of fusion imaging technology
Echocardiography is a representative imaging technology used to diagnose and guide treatment of pediatric CHD. However, it has limited ability to evaluate the pulmonary blood vessels or other structures in the chest or abdomen, and it is often difficult to obtain sufficient information in patients with a large body size or if the echo window quality is poor. To overcome these limitations, computed tomography (CT) or magnetic resonance imaging has also been used. As the quality of these images improves thanks to technological advancements, methods for obtaining additional hemodynamic information that were previously impossible are becoming possible, and the two techniques are replacing many parts of invasive surgery [39,40].
Another trend is that catheter-based intervention is becoming much easier since it combines the advantages and disadvantages of various images using fusion imaging of fluoroscopy and echocardiography or fusion imaging of CT and echocardiography [41,42]. The concept of fusion imaging, which fuses two different modalities in real time on a single monitor, aims to overcome the shortcomings of individual imaging. Examples include echocardiographic-fluoroscopic fusion imaging, 3-dimensional fusion of coronary CT angiography and CT myocardial perfusion imaging, and fusion of a three-dimensional CT dataset to routine fluoroscopic images. This fusion imaging technology has already been widely used in clinical practice and will be of great help in the clinical field in the future.
Ambulatory monitoring device
Although Holter monitoring has long been the device of choice for cardiac monitoring, continuous monitoring remains difficult. However, owing to the recent development of electronic devices, various ambulatory monitoring devices are making a new paradigm of health care possible [43]. If wearable electrocardiography (ECG) monitoring is used for patients with CHD, important data can be obtained to prevent unnecessary medication and inappropriate treatment. In particular, in the arrhythmia area, wireless ECG monitoring systems or implantable ECG monitoring devices are actively used to diagnose arrhythmias that are not confirmed by conventional Holter monitoring or to check the therapeutic effect. In addition, ambulatory blood pressure monitoring will be of great help in the management and treatment of hypertensive patients.
Smartphone-based cuffless blood pressure monitoring and wearable and flexible pressure sensors based on microfluidic elements have been developed. As such, miniaturization and wireless equipment enable the easy collection of biometric information. As hardware and software algorithms for various wearable sensor systems such as the Zio patch, smart phones, and Google Glass have been developed, it has become possible to obtain information about heart rhythm or blood pressure in a variety of easy ways. Beyond the monitoring level, wireless pacemakers have recently become available. However, determining the extent to which a vast amount of information can be trusted and utilized is also an urgent task.
VAD and heart transplantation
Despite advances in medical and surgical therapies, some CHD patients are not treated satisfactorily and develop progressive HF. In such cases, heart transplantation should be considered as another standard treatment, but due to the limitation of the donor pool, a VAD is also used as a destination or bridging therapy [44-46]. VAD application in children with small stature or complex heart defects such as a single ventricle has limited experience and technical difficulties compared to general adult patients, but it is being continuously attempted. In ACHD patients, morbidity and mortality are expected to be high because there are many cumulative risk factors, such as multiple prior surgeries, longstanding cardiac dysfunction or cyanosis, elevated pulmonary vascular resistance, hepatic dysfunction, and renal dysfunction. Therefore, in addition to evaluating the hemodynamic information and function of multiple organs, it is necessary to prepare for transplantation and perform posttransplant management with the cooperation of a multidisciplinary team including nutritionists, psychologists, and social workers [47].
Conclusion
As the number of GUCH patients exceeds the number of pediatric CHD patients, the problems of HF and arrhythmias become more important and the associated medical burden increases. The use of various images is essential for ensuring the accurate diagnosis and treatment of ACHD patients, and ambulatory monitoring devices are increasingly used. A multidisciplinary team approach is required for VAD or transplantation of CHD patients with advanced HF.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.