Diagnostic and prognostic value of proadrenomedullin in neonatal sepsis
Article information

Abstract
Purpose
Sepsis is a major cause of neonatal morbidity and mortality. Early diagnosis is a major problem because of the lack of specific clinical signs. Therefore, a reliable diagnostic marker is needed to guide the use of antimicrobial agents. The objective of our study was to assess the value of proadrenomedullin (pro-ADM) in establishing the diagnosis and evaluating the prognosis of neonatal sepsis.
Methods
This study enrolled 60 newborn infants with sepsis proven with positive blood cultures and 30 healthy neonates. Complete blood count, C-reactive protein levels, and pro-ADM levels were obtained from all neonates.
Results
The pro-ADM levels were significantly higher (14.39±0.75 nmol/L) in the sepsis group than in the control group (3.12±0.23 nmol/L). The optimal cutoff value for pro-ADM was 4.3 nmol/L, with a sensitivity of 93.3% and a specificity of 86.7%. The pro-ADM levels were also higher in nonsurvivors (P=0.001).
Conclusion
Pro-ADM can be used as a reliable biomarker for neonatal sepsis. High pro-ADM levels were associated with mortality and could be an early indicator of disease outcome.
Introduction
Sepsis is one of the major causes of death during neonatal period. Despite recent advances in treatment of neonatal infection, mortality and comorbidities remain high.1)
Early and accurate diagnosis of neonatal sepsis represent important challenge for neonatologists as clinical signs are difficult to differentiate from other noninfective neonatal conditions. Although blood culture is the gold standard for diagnosis, its result takes too long time.2) False negative results are common because of low-level bacteremia, and the small volume of blood sample. Moreover, the early administration of antibiotic before withdrawn of blood culture significantly reduce its diagnostic accuracy.3)
Early diagnosis of neonatal sepsis is crucial to avoid clinical deterioration, reduce mortality and prevent unnecessary use of antimicrobial agents. Also, accurate diagnosis will decrease the incidence of antibiotic resistance and reduce treatment-related cost.4)
Adrenomedullin (ADM) consists of 52-amino acid and possesses vasodilator and natriuretic properties. ADM could be used as a biomarker for cardiovascular diseases and infection.5)
However, reliable measurement of ADM in the circulation is very difficult because of its very short plasma half-life (about 22 minutes). Midregional pro-ADM (MR-proADM) is a fragment of ADM precursor (amino acids 45 to 92) and is more stable than the rapidly cleared ADM. MR-proADM is easy to measure and reliably reflects the amount of released ADM.6)
The aim of our study was to assess the value of pro-ADM in establishing the diagnosis and evaluating the prognosis of neonatal sepsis.
Materials and methods
This prospective study was conducted at the Neonatal Intensive Care Unit of Beni Suef University Hospital in the period between May 2016 and January 2017. Sixty neonates fulfilling the criteria for diagnosis of septicemia were included in our study (sepsis group). The control group included 30 healthy neonates, they were recruited from follow-up clinic for healthy neonate.
Patients with cardiac failure, maternal preeclampsia, or intracranial hemorrhage (Conditions in which plasma pro-ADM have been reported to be elevated) were excluded from the study.
Sepsis was defined as a positive blood culture in infants with clinical and laboratory findings of infection. Manifestations of sepsis include poor suckling, sleepiness, respiratory distress, apnea, poor perfusion, cyanosis, bradycardia, fever or hypothermia, feeding intolerance, and neurological signs (as seizures).7)
Routine sepsis evaluations included complete blood count, C-reactive protein, and blood culture. Blood was drawn from all neonates for Pro-ADM assay.
1. Sample collection and Pro-ADM assay
Blood samples were taken from septic neonates after confirmation by positive blood culture. Blood samples were collected under standardized conditions in plasma collection tubes containing ethylenediaminetetraacetic acid. Then, samples were centrifuged at 1,000×g (2℃–8℃) for 15 minutes within half an hour of collection then plasma samples are stored at −20℃. Samples are centrifuged again after thawing before the assay.
The assay applies the quantitative sandwich enzyme immunoassay technique using Human Pro-ADM ELISA Kit (Cusabio Biotech Co., Ltd., Wuhan, China).
The study protocol was approved by Beni Suef University Hospital ethical committee (approval number: 187-16), and written informed consent was obtained from caregivers.
2. Statistical analysis
Data management and analysis were performed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA).
Data were described as mean±standard deviation or frequencies and percentages when appropriate. Comparisons between cases and controls were done using the t tests. We used Mann-Whitney test to compare 2 unrelated samples. To measure the strength of the association between pro-ADM and other parameter, Pearson correlation coefficients were used. The Receiver operator characteristic (ROC) curve was used to demonstrate the relationship between sensitivity and specificity.
Results
Our study included 90 neonates (60 septic neonates and 30 healthy controls). Their clinical and laboratory characteristics are summarized in Table 1. Septic neonates had a lower weight compared with neonates in the control group. Pro-ADM concentrations were significantly higher (P<0.001) in the septic group (14.39±0.75 nmol/L) compared with control group (3.12±0.23 nmol/L).

Demographic and laboratory data of case and control groups
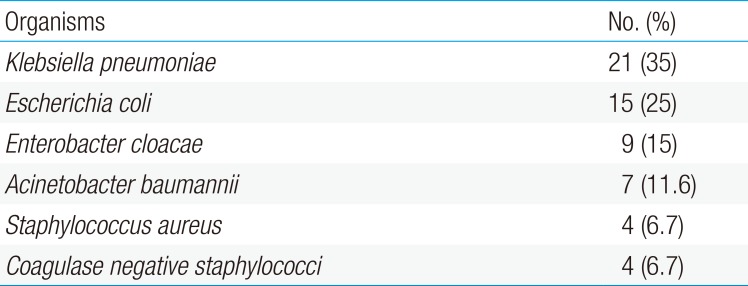
The pathogens detected in blood cultures of septic neonates are listed in Table 2. Klebsiella pneumoniae was the most frequent organism isolated.

Distribution of pathogens isolated from neonates with sepsis
Eleven neonates (18.3%) received mechanical ventilation, 8 neonates (13.3%) received continuous positive airway pressure, total parenteral nutrition was given to 12 septic neonates (20%) and central venous catheters were required in 14 neonates (23.3%).
Of the 60 septic infants that were included in the study, 12 neonates (20%) died while 48 neonates (80%) recovered and discharged. The mean pro-ADM levels in survivors and nonsurvivors were 14.21±0.72 nmol/L and 15.08±0.27 nmol/L, respectively (Fig. 1). Pro-ADM levels were significantly higher in patients who died with a P value=0.001.

Proadrenomedullin (Pro-ADM) levels in survivors and nonsurvivors. Pro-ADM levels were significantly higher in nonsurvivors (15.08±0.27 nmol/L) than in survivors (14.21±0.72 nmol/L). P=0.001.
The area under the receiver-operating curve for pro-ADM was 0.923 (95% confidence interval [CI], 0.85–0.97) (Fig. 2). A pro-ADM value of 4.3 nmol/L was established as a cutoff value with 93.3% (95% CI, 78–99) sensitivity and 86.7% (95% CI, 59–98) specificity. The positive and negative predictive values were 93.3% (95% CI, 85–97) and 86.6% (95% CI, 71–94), respectively.
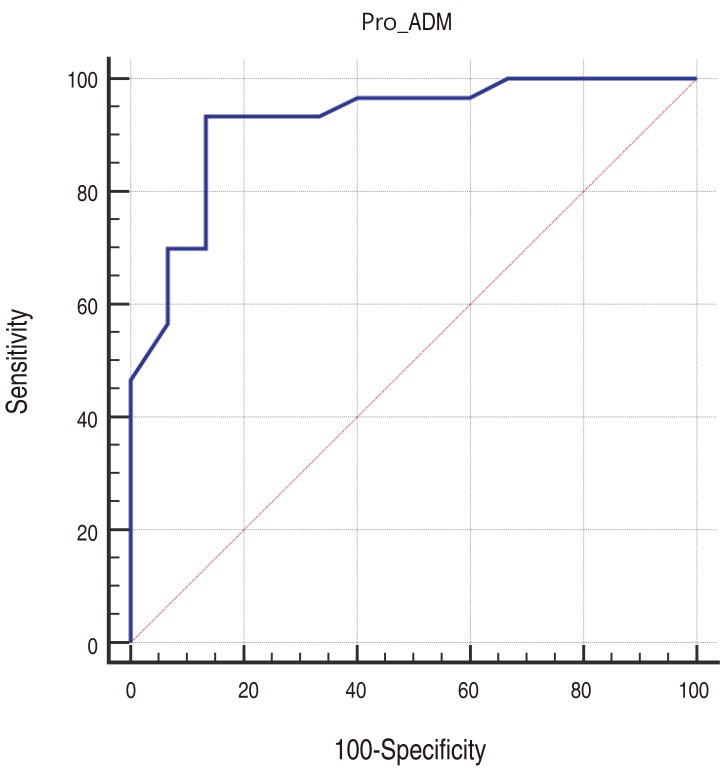
Receiver operating characteristic curve for proadrenomedullin (pro-ADM) at a cutoff value of 4.3 nmol/L. The area under the curve was 0.923 (95% confidence interval, 0.85–0.97). The sensitivity, specificity, positive predictive value, and negative predictive value were 93.3%, 86.7%, 93.3%, and 86.6%, respectively.
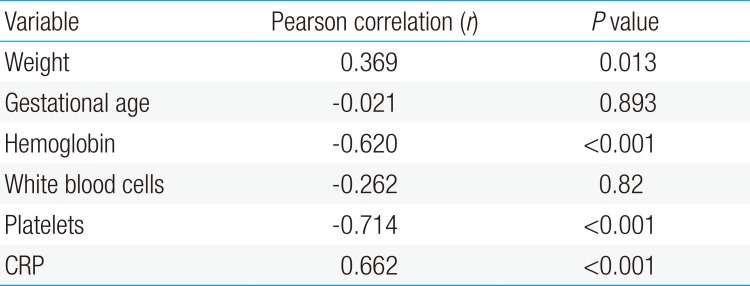
As shown in Table 3, the levels of pro-ADM were positively correlated with weight (r=0.36, P=0.013) and CRP (r=0.662, P<0. 001). However, pro-ADM levels tended to correlate negatively with platelets count (r=−0.714, P<0.001) and hemoglobin (r=−0.62, P<0.001).

Correlation between pro-ADM and other parameters in the sepsis group
Discussion
Neonatal sepsis is a major health challenge in neonatal intensive care units and has a fulminant and fatal course if treatment is not initiated rapidly. The identification of reliable and accurate biomarkers for sepsis could guide treatment, reduce overuse of antimicrobial agents, and possibly improve prognosis.8)
In sepsis, the release of bacterial toxin triggers a series of events that stimulate intracellular pathways to produce inflammatory mediators. One of these mediators is ADM which has an important role in vascular tone regulation in infection and cardiovascular disease.9)
ADM has a potent vasodilator property. Its stable midregional pro-hormone fragment, pro-ADM, is used as a biomarker of sepsis and cardiovascular diseases in adults.10) Many adult studies investigated the relationship between infection and pro-ADM. In a study of 101 adult patients, authors found a significant increase in pro-ADM levels in septic patients as compared with healthy controls and critically ill patients without infections.6) Moreover, Angeletti et al.11) investigated the pro-ADM levels of adult patients with bacterial infection, and they showed that pro-ADM levels are significantly increased in patients suffering from localized bacterial infections.
The results of the present study showed that serum pro-ADM levels were significantly higher among septic infants compared with healthy ones. This finding comes in agreement with previous studies suggesting increased levels of pro-ADM in neonates with bacterial infection.1213)
Our study revealed that nonsurviving patients had significantly elevated pro-ADM levels when compared to the survivors (15.08±0.28 nmol/L vs. 14.21±0.73 nmol/L, P=0.001). This observation is similar to that of a recent study by Abd Elmouttaleb et al.14), in which pro-ADM levels were significantly higher in nonsurviving septic neonates. Wang and Kang15) studied the value of pro-ADM as a prognostic marker in septic adults. Their study revealed that pro-ADM levels were significantly elevated in nonsurvivors, and that pro-ADM was valuable marker for predicting sepsis severity and outcome.
We used the ROC curve analysis to select the best cutoff value for pro-ADM. The ideal cutoff value for pro-ADM is the level capable to discover nearly all true cases (high sensitivity) with a little probability of false positives (high specificity). For neonatal sepsis, it is more valuable to have the highest level of sensitivity than the highest level of specificity.16)
In our study, pro-ADM (using a cutoff value of 4.3 nmol/L) had a sensitivity of 93.3% and specificity of 86.7% with a positive predictive value of 93.3 % and negative predictive value of 86.6%. In a study using pro-ADM to discern sepsis in neonates, Oncel et al.12) reported sensitivity comparable with ours (93.5% for a cutoff value 3.9 nmol/L) but higher specificity (100%). Another study by Cao et al.13) is similar to ours, but their sensitivity is much lower (51.53%). However, the number of patients with culture-proven sepsis in the above-mentioned studies is smaller than in our study, and none of them evaluate pro-ADM as prognostic marker.
Debiane et al.17) evaluated pro-ADM as a marker of sepsis in adult patients with malignancy. They reported 67% sensitivity and 68% specificity for pro-ADM at a cutoff value 2.2 nmol/L.
We found a positive correlation between pro-ADM and C-reactive protein (r=0.662, P<0.001). Similar finding has been reported in previous study.12) On the other hand, pro-ADM were negatively correlated with platelets count (r=−0.714, P<0.001) in our patients. Comparable finding has been reported in previous adult study.18)
The main strength of this study is that we have included only patients with blood culture-proven sepsis.
Our study has some limitations. First, the sample size was relatively small. Second, no comparison was made between pro-ADM and other inflammatory markers (as erythrocyte sedimentation rate and procalcitonin). Third, single measurement of pro-ADM levels was done, so serial measurement of pro-ADM might be more useful.
In conclusion, our study highlights the role of pro-ADM in neonatal sepsis. Pro-ADM may be considered a reliable marker for neonatal sepsis that could help in identifying septic neonates. A value higher than 4.3 nmol/L should raise the suspicion of sepsis. High pro-ADM concentration was associated with mortality and could be an early indicator of disease outcome.
Acknowledgments
We gratefully acknowledge the valuable cooperation provided by our colleagues in the NICU, Beni Suef University Hospital.
Notes
Conflicts of interest: No potential conflict of interest relevant to this article was reported.