Sudden unexpected cardio-respiratory arrest after venipuncture in children
Article information

Abstract
Purpose
This study aimed to investigate the clinical and socioenvironmental characteristics of sudden cardiorespiratory arrest after venipuncture in children.
Methods
We conducted a retrospective email-based survey of all members of the Korean Pediatric Society. The questionnaire included items on patient demographics, socioenvironmental circumstances of the venipuncture, type of cardiorespiratory arrest, symptoms and signs, treatment, prognosis, and presumed cause of the arrest.
Results
Fourteen patients were identified. Of these, 13 were young children (<2 years old), and 1 was 14 years old. All patients had been previously healthy and had no specific risk factors for sudden cardiorespiratory arrest. Most cases (n=11, 79%) were defined as cardiac or cardiorespiratory arrest, while the remaining cases (n=3, 21%) were defined as respiratory arrest. Aspiration (n=3), acute myocarditis (n=2), and laryngeal chemoreflex (n=1) were presumed as the causes; however, the exact causes were unclear. The overall prognosis was poor (death, n=7; morbidity, n=5; full recovery, n=2). The medical institutions faced severe backlash because of these incidents (out-of-court settlement, n=5; medical lawsuit, n=5; continuous harassment, n=3).
Conclusion
Cardiorespiratory arrest after venipuncture is unpredictable and the probable cause of most cases is a vasovagal reaction. Medical personnel must be aware of the risk of unexpected cardiorespiratory arrest during routine intravenous procedures.
Introduction
Venipuncture is the most common invasive medical procedure performed at hospitals. Although accompanied by minor complications such as minimal pain, bruising, and thrombophlebitis, venipuncture is considered safe and well tolerated. But few studies123456) have reported serious complications after venipuncture, such as sudden cardiac arrest. It is not unheard of that cardiac arrest could occur following venipuncture. In 1966, McKay7) already mentioned cardiac arrest as extremely uncommon hazards of venipuncture. Blood banks also often observe the syncope associated with blood-injury phobia. However, most serious venipuncture complications reported previously were related to transfusion or blood donation,89) and the affected individuals were adults and adolescents.610) Unfortunately, little is known of the cardio-respiratory arrest following venipuncture in children. Here, we investigated the clinical features of sudden cardio-respiratory arrest after venipuncture in children. Sudden unexplained cardiac arrest or death is a rare occurrence in the young, with and incidence between 1.3 and 8.5 per 100,000 patient-years.11) Cardiac causes were most common, but an etiology was less evident in infants in comparison to older children.12) Although the definite causes have not been identified, vasovagal reaction has been suggested as a cause of cardiac arrest following venipuncture, resulting in serious cardiac dysfunction, such as asystole.
Materials and methods
An electronic survey (email) was used to collect data on cardiorespiratory arrest following venipuncture in children from August to September 2015. The survey was sent to all pediatricians among the members of Korean Pediatric Society on line through www.pediatrics.or.kr. The survey questionnaire was designed by the Legislation Board of Korean Pediatric Society and the Korean Society of Sudden Death in Childhood. Members of the Korean Pediatric Society were identified from the 2015 member directory. The questionnaire was sent out twice at a 1-month interval to maximize the response rate. Initially, 11 cases were identified through our survey. While preparing for the paper, further replies were received and 3 cases were newly included. The questionnaire included patient demographics, past medical history, family history, underlying disease, socio-environmental circumstances of venipuncture (purpose, place, time to arrest after venipuncture, performer, fasting time before the procedure, vital signs monitoring, and blood loss volume), type of arrest, symptoms and signs, treatments, prognosis, and presumptive causes of arrest. The data were analyzed using Excel 2013 (Microsoft, Redmond, WA, USA). The study was approved by the Institutional Review Board of Cheil General Hospital & the Women's Healthcare Center (approval number: CGH-IRB-2015-33).
Results
Of the collected data, we present the most well-described case in detail. A 1-month-old boy was admitted to the hospital for a fever. He was born at a gestational age of 39 weeks, with a birth weight of 2.8 kg without perinatal problems. His family history was unremarkable. At presentation, his body weight was 4.2 kg. Before venipuncture, he was alert and his vital signs were stable: his blood pressure was 80/50 mmHg; pulse rate, 144 per minute; and respiratory rate, 44 per minute. It took about 5 minutes to try to insert a peripheral intravenous catheter. Immediately after the procedure, the patient presented sudden cyanosis and became extremely lethargic without spontaneous breathing. The airway was immediately opened, oxygen was supplied, and cardiac massage was initiated, followed by intubation and administration of epinephrine. Seven minutes after the beginning of resuscitation, spontaneous circulation was restored. The patient recovered completely without complications. The cause of arrest could not be deduced from a normal electrocardiogram, but a cardiac echocardiogram showed a small persistent ductus arteriosus.
Fourteen cases were identified through our survey. The clinical characteristics of the patients are given in Table 1. Most patients were younger than 2 years (n=13, 93%) at the time of the event; 11 were 1–11 months old, 2 were 1–5 years old, and 1 was older than 12 years. The time interval between the arrest and venipuncture was less than 30 minutes in most cases (n= 11, 79%). In 4 cases (cases 2, 3, 7, and 9), the arrest occurred immediately after the venipuncture. The number of venipuncture attempts was not available, except in one case (case 1): in case 1, venipuncture was attempted 3 times and arrest occurred 30–60 minutes later. The most common initial manifestations of arrest were cyanosis (n=13, 93%), lethargy (n=9, 64%), pale appearance (n=6, 43%), pulseless (n=3, 21%), and seizure (n=2, 14%). None of the patients had a previous medical history that could explain the sudden cardio-respiratory arrest, such as syncope, congenital or acquired heart disease, arrhythmia, chronic lung disease, asthma, epilepsy, and central nervous system diseases. In addition, none of them had a family history of cardiac disease, syncope, or sudden death. Blood loss during venipuncture was not so high as to cause hypovolemia in any case. Over 75% of the cases (n=11, 79%) were of cardiac or cardio-respiratory arrest, while the rest (n=3, 21%) were of respiratory arrest. The causes of arrest could not be ascertained in any case. The presumptive cause was aspiration during the procedure in three patients (cases 4, 12, and 13) and prior acute myocarditis (cases 5 and 8) in 2 patients, in whom cardiac enzyme levels were elevated but not enough to conclude that the myocarditis was a direct cause of the arrest. In case 6, laryngeal chemoreflex was the presumptive cause of arrest. An autopsy was conducted in 2 patients (cases 1 and 14), but the cause of arrest was not identified.

Clinical characteristics of the patients (n=14)
During resuscitation, epinephrine (n=11, 79%) or atropine (n=3, 21%) was administered. The prognosis was poor despite resuscitation. Two patients recovered completely to the premorbid state. Five patients survived but developed serious sequelae, while 7 died. The socioenvironmental characteristics of the venipuncture are described in Table 2.

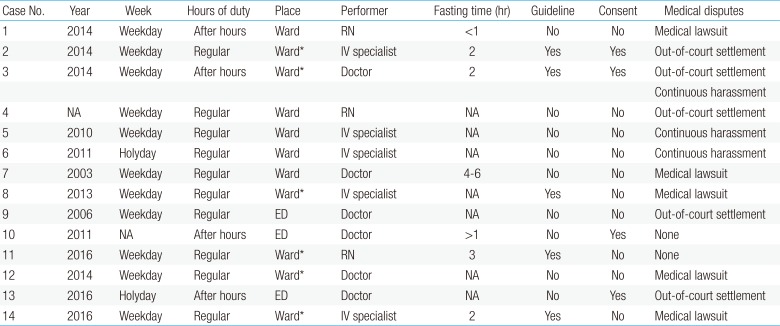
Socioenvironmental characteristics of the venipuncture (n=14)
The doctors and medical institutions responsible for these events had to agree to out-of-court settlements (n=5, 36%), faced medical lawsuits (n=5, 36%), or were continuously harassed (n=3, 21%).
The accidents occurred more frequently during weekdays (n=11, 79%) than holidays (n=2, 14%). Further, they occurred more frequently during regular working hours (n=10, 71%) than after hours (n=4, 29%). Venipuncture was performed by doctors, registered nurses, and intravenous specialists. The fasting time before venipuncture varied and was not available in 7 cases. In 4 cases, the adverse effects of venipuncture were explained to the parents prior to the procedure, but the risk of cardio-respiratory arrest was not included.
Discussion
Although cardio-respiratory arrest after venipuncture is extremely rare in children, it does happen and is an unpredictable event in apparently healthy children. These events have devastating impact both on the families and medical institutions. Although the exact mechanisms for the development of the cardio-respiratory arrest after venipuncture have not been clearly elucidated, a vasovagal reaction triggered by emotional stress (painful or noxious stimuli or fear of bodily injury) may play a significant role. All patients except one were younger than 2 years. They could not understand the procedure, so may have experienced profound stress and been frightened.
The main pathophysiology of a vasovagal reaction is thought to be a cardioinhibitory response resulting from either increased parasympathetic activation, vasodepressor response due to inhibition of sympathetic activity, or, more often, a combination of the two.131415) The cardioinhibitory response may be manifested by any or all of the following: sinus bradycardia, asystole, PR interval prolongation, and advanced atrioventricular block. The vasodepressor response can lead to symptomatic hypotension even in the absence of severe bradycardia.1516) In one report, the final trigger for symptomatic hypotension appeared to be the abrupt disappearance of muscle sympathetic nerve activity.14) Reduced cardiopulmonary baroreceptor sensitivity may be a contributing factor.17) Emotional or somatic factors trigger an intense parasympathetic state. Increased parasympathetic tone causes vasodilatation, reduces venous return, and depresses cardiac function, leading to profound bradycardia or hypotension. Usually vasovagal syncope is spontaneously reversible. However severe vasovagal reaction to emotional distress occasionally results in death.181920)
It is unethical and dangerous to check recurrent asystole following venipuncture. Since there is no accurate diagnostic tool to indicate that the vasovagal reaction is directly attributable to the sudden arrest, it is reasonable to exclude other cause. Our findings show that cardio-respiratory arrest after venipuncture is unpredictable. None of the patients reported here had serious risks for cardio-respiratory arrest. In the present study, this complication of venipuncture occurred more frequently during regular working hours than after hours. Since our study is a retrospective study, we could not evaluate the technical competence of the individuals who performed the venipuncture and the extent of the children's fear during venipuncture. Arrest occurred even though venipuncture was performed by skilled IV specialists, in some cases. Rapid and precise venipuncture could decrease pain, but it may not prevent events such as cardio-respiratory arrest. Thus, these events may not result from lack of manpower or carelessness.
Although not identified in this study, cardiac dysfunction, such as acute myocarditis, can be considered as a possible cause in unusually ill patients. In a coroner's review of 126 sudden deaths before the age of 2 years, 10% were associated with congenital cardiac lesions, and 6 percent with myocarditis.21) In one single center study, the etiology for sudden cardiac arrest was identified in 57% of the cases, mostly in those above 1 year of age and among these the majority of had a cardiac etiology (50%) while 7% had rupture of an arteriovenous malformation.12) Acute myocarditis is a disease with a variable natural history and is difficult to diagnose. Often, the symptoms of acute myocarditis are initially flu like, either of the upper respiratory or gastrointestinal tract, before any cardiac symptoms appear. Any patient who develops bradycardia or asystole or requires cardiopulmonary resuscitation should undergo a complete evaluation to exclude a cardiac cause.1222)
Not all sudden cardiac arrests can be foreseen, even in the best of circumstances. No screening protocol has yet proven to be effective in this role or validated as highly effective.23)
In adults, the incidence of a vasovagal reaction after blood donation has been reported to be about 1%.2425) The World Health Organization provided the following practical guidelines to limit the vasovagal reaction, syncope, and fainting during phlebotomy: (1) hydrate the patient and record postural blood pressure if dehydrated, (2) reduce anxiety, (3) have the patient lie down if they express concern, and (4) provide audio-visual distraction.26)
Various medical treatments may be indicated to prevent cardiorespiratory arrest after venipuncture. Lidocaine cream can decrease the pain during venipuncture as a topical anesthetic, but it is ineffective in suppressing a blood injury phobia itself.27) Although anticholinergic drugs, such as atropine sulfate, are often the first line of treatment for bradycardia, they may not be the best single agents if the bradycardia is accompanied by vasodilation.28) Hypotension during vasovagal syncope may persist after the bradycardia is relieved by atropine. Sympathomimetic drugs, in contrast, counteract the vasodilation in both arterial and venous circulations. Commonly used sympathomimetics are epinephrine and various selective α-agonists. In case of suspected cardiac arrest caused by vasovagal reaction following venipuncture, epinephrine will be more effective than atropine.
The minimum fasting time prior to venipuncture remains controversial, and no established guidelines are available on this matter. Additionally, it is unrealistic to apply preoperative fasting guidelines to venipuncture. For example, immediate IV access is needed in severely dehydrated patients, and delaying venipuncture in order to ensure adequate fasting time could worsen the patient's condition.
Rather, the Academy of Breastfeeding Medicine Clinical protocol recommends avoiding unnecessary fasts. It suggests that minor painless procedures without sedation or general anesthesia such as placement of peripheral intravenous lines and drawing blood do not require fasting and breastfeeding while receiving a venipuncture can be an effective means of pain relief.29)
The limitations of this study were the relatively small sample size due to the low response rate, difficulties in remembering the experience to complete the questionnaire, and the lack of precise medical evaluation in individual cases for the cause of the sudden arrest. Nonetheless, our study is the first to explore the medical and socio-environmental characteristics of unexpected sudden arrest associated with venipuncture. To our knowledge, our study is the first report of cardio-respiratory arrest following venipuncture in neonate and young infant. Except one patient, the rest of the patients were under the age of two. The youngest ever reported age was 11 years old.3)
In conclusion, cardio-respiratory arrest after venipuncture is unpredictable, and a vasovagal reaction may be the cause. The pathogenic mechanism of this event must be clarified in order to prevent this tragic complication in the future.
Acknowledgments
The authors thank the Korean Pediatric Society, its Legislation Board, and the Korean Society of Sudden Death in Childhood for preparing the survey report and collecting data.
Notes
Conflicts of interest: No potential conflict of interest relevant to this article was reported.