Clinical features of Bednar's aphthae in infants
Article information
Abstract
Purpose
Although Bednar's aphthae are common and regress spontaneously, these lesions may lead to feeding intolerance and are often misdiagnosed, rendering examinations useless. This study sheds new light on the clinical features of Bednar's aphthae.
Methods
Sixteen neonates and infants were newly diagnosed with Bednar's aphthae via routine health check-ups in an outpatient clinic. Medical records were retrospectively reviewed, and the following parameters were analyzed; sex, gestational age, birth weight, mode of delivery, and perinatal problems. A physical examination was carried out during the next outpatient visit to examine the healing process and check for the existence of scars or complications.
Results
Initial presentation included changes in feeding habits (n=10), longer feeding time, reduced intake, and increased irritability. In 6 patients, Bednar's aphthae were discovered incidentally, without prior symptoms. Feeding posture and method of feeding are important causes of Bednar's aphthae. Eleven patients were fed in a horizontal position, whereas 5 patients were fed in a semiseated position. Fifteen patients were bottle-fed, whereas 1 patient was exclusively breastfed. After correcting the feeding position, the ulcerative lesions disappeared within 1 month of diagnosis. During the follow-up period, lesions did not recur in any of the patients.
Conclusion
This study suggests that Bednar's aphthae are caused by mechanical pressure. A diagnosis of Bednar's aphthae should be considered when lesions are found on the palate of infants and when symptoms seem to be feeding related. Proper education of parents can both treat Bednar's aphthae and easily prevent its recurrence.
Introduction
Although oral mucosal lesions (e.g., candidiasis, stomatitis, aphtha's ulcer, traumatic injury, etc.) are often encountered in children in outpatient clinics, the classification and incidence rates remain unclear. Depending on the study, incidence rates vary considerably from 4.1% to 52.6%123456). The study conducted by Bessa et al.2) revealed that oral mucosal lesions were found 24.9% of 746 infants aged 0 to 4 in the order of geographic tongue (9.9 %), bite injury (4.7%), traumatic lesion (2%), and recurrent aphthous stomatitis (1.5%). The study by Bezerra and Costa3) shows that 2.3% of the infants aged 0 to 5 were observed with oral mucosal lesions, consisting of Bohn's nodule (37%), candidasis (25%), and geographic tongue (21%).
Ulcerative lesions of the oral mucosa show pathologies of either infectious or traumatic origin78). Herpetic gingivostomatitis, herpangina, hand foot mouth disease and candidiasis are lesions caused by infection. Lesions of infectious origin are relatively easy to diagnose due to their distinct form and clinical course such as fever. Traumatic lesions are usually created by orthodontic prostheses or by pacifiers within the oral cavity. Bednar's aphthae are small, shallow ulcers on the edge of newborns' palates and are typically caused by traumatic action of a bottle nipple or even the mother's breast during feeding9).
Usually mucosal lesions are found ranging from the posterior borderline of the hard palate to the soft palate. They are usually symmetrical, located medial to the mucosal plica connecting the maxilla and mandible and typically heal spontaneously within one month without sequelae21011). Although they have a benign course, lesions can affect feeding habits, resulting from discomfort when the neonate sucks. Around 1960, it was believed that Bednar's aphthae were caused by wiping a neonate's mouth or by mechanical impacts such as those from a pacifier or dummy. Some studies have suggested diagnostic criteria of Bednar's aphthae to differentiate them from trauma-induced lesions1213). More recent reports suggest a new hypothesis for the pathogenesis of Bednar's aphthae as an immune process913).
Since Alois Bednar first described aphthae in 1850, most reports concerning the condition were published in the 19th and the beginning of the 20th century. However, in recent literature and textbooks, one can hardly find any clear information. Although Bednar's aphthae are not a rare phenomenon, they often remain undiagnosed or misdiagnosed due to lack of concern. Therefore, the purpose of this study was to investigate the clinical characteristics of Bednar's aphthae in Korean infants.
Materials and methods
Sixteen neonates and infants who had been diagnosed with Bednar's aphthae at the Cheil General Hospital & Women's Healthcare Center, Seoul, Korea between May, 2012 and December, 2013 were enrolled in this study. Bednar's aphthae were diagnosed by physical examination during routine health check-ups in the outpatient clinic. Medical records were retrospectively reviewed and the following parameters were analyzed: sex, gestational age, mode of delivery, birth weight, and perinatal problems. We visualized the palate of the patients using a tongue depressor and documented the characteristics of ulcers such as the number, location, shape, size, hyperemia, exudates, and extension to the uvula. General illnesses such as fever and the presence of other anomalies that could affect the feeding habits, were examined. Feeding habits, feeding method (breast feeding, bottle feeding), type of nutrition (breast milk, formula, or both) and use of pacifier or dummy were recorded from interviews with infants' parents. Nursing time and feeding amount were not quantitative; its changes were based on parent's statements. Parents were also educated on the proper posture of feeding, and a follow-up visit was conducted to track the course of the lesions.
The Institutional Review Board of Cheil General Hospital & Women's Healthcare Center approved the study (IRB number: CGH-IRB-201602).
Results
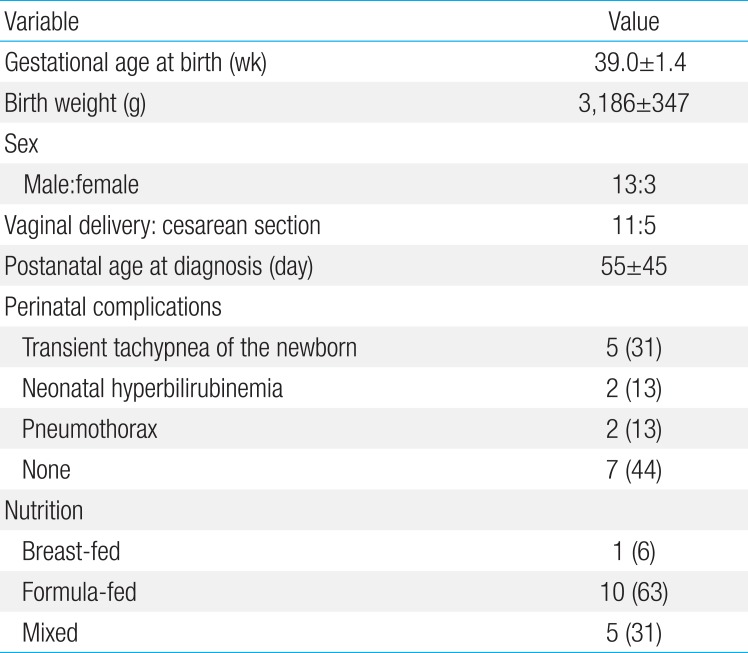
The demographics of the subjects are shown in Table 1. All patients were full-term babies, and no low birth-weight infants were included in the study. Some subjects experienced perinatal problems such as transient tachypnea as newborns, neonatal hyperbilirubinemia, and pneumothorax, but none of the subjects suffered from severe illnesses or immunological diseases.

Patient demographics
Most of the initial symptoms were related to changes in feeding habits; longer feeding time (n=8), reduced intake (n=8), and increased irritability during feeding (n=2). Six patients were asymptomatic and were discovered accidentally.
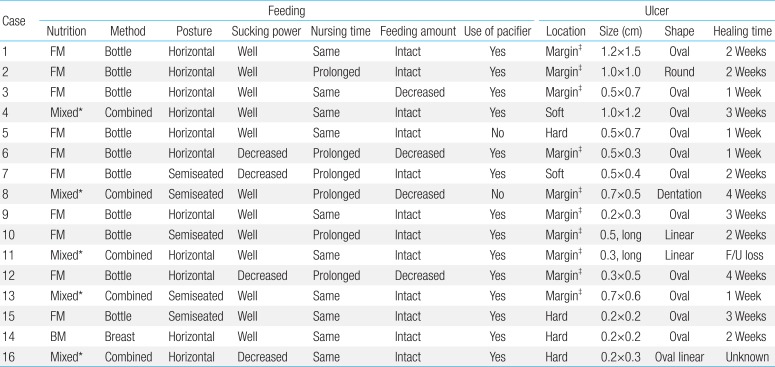
Characteristics of oral lesions are listed in Table 2. Physical examinations revealed lesions situated along the border of the hard palate and soft palate, and most were distributed symmetrically and were oval or round in shape and centered on the midline (Fig. 1). Three patients had linear lesions extending to the uvula. The largest lesion was 1.5 cm in length, and the surface was whitish in color with clear margins. Most of the lesions occurred on the surface of the skin, so their depth could not be determined. No exudate or hyperemia was observed; neither was bleeding. Oral thrush was not discovered in other areas of the oral cavity such as the gingiva or tongue. Oral abnormalities such as cleft lip, cleft palate, high arched palate, uvula bifida, ankyloglossia, and other structural deformities of the chin were not observed.

Feeding and ulcer characteristics

View of Bednar's aphthae on diagnosis with a midline lesion positioned on the border of the hard palate (case 13).
Fifteen patients were formula-fed, while one patients was completely breastfed. Out of fifteen patients, five of them started formula feeding or combined feeding 1 or 2 weeks before diagnosis was done. Eleven patients were fed in horizontal position whereas 5 patients were fed in semiseated position. Five patients used various nipple or recently changed the nipple hole size. Changes of body weight were not recorded. Laboratory blood test and culture of pharyngeal secretion were not carried out.
Mothers were trained to change into semiseated position instead of horizontal position, and the nipple hole sizes were promptly replaced with bigger ones. No antibiotics were used for treatment. No one needed further treatment such as admission, hydration, and oral ointment. All patients showed satisfactory progress, in which their lesions either spontaneously healed or disappeared altogether. There were no complications such as conspicuous scarring. Typically, the lesions disappeared between one or two weeks. One patient (patient 8) took the 4 weeks to heal but additional damage caused a burn is suspected. During the follow-up period, there was no recurrence of the lesions in any of the patients.
Discussion
Although Bednar's aphthae are not rare lesions, they often remain undiagnosed or misdiagnosed due to lack of concern. Bednar's aphthae are seldom reported in recent literature. Studies on these subjects are rare because the incidence rate of Bednar's aphthae declined after the development of orthodontic bottles and nipples. Nevertheless, prospective study of Nebgen et al.9) in 2010 recorded and incidence rate of 15% (236 of the 1,494 neonates), which suggests that Bednar's aphthae incidence is still quite steady. Among the infants that were born spontaneous vaginal delivery and fed formula, Bednar's aphthae observed in 29.8%. Whereas the neonates that were born by cesarean section and breast-fed showed in 11.8%. They concluded that Bednar's aphthae are not a rare phenomenon. They described that most important associated factors were the kind of nutrition and the mode of delivery. They reported hypothesis that there might be an immunological reaction that causes Bednar's aphthae. Neonates born through the vaginal delivery become exposed to vaginal flora, thereby increasing the incidence rate of Bednar's aphthae. This result corresponded with our findings which showed higher incidence of Bednar's aphthae in vaginal delivery than cesarean section.
In this study, Bednar's aphthae were found to be associated with increased irritability and changes in feeding habits. Symmetric lesions were found on infants' palates without other systemic illness. Usually the lesions were oval shaped and had smoothly contoured borders without exudate.
The physiopathologic causes of Bednar's aphthae are still unclear, but they are attributed to traumatic actions of bottle nipples during feeding and probably to feeding in a horizontal position12). This study proves that Bednar's aphthae are caused by mechanical pressure, and despite its undefined statistical significance, Bednar's aphthae are considered to occur more frequently when bottle feeding.
Neonates who demonstrate high fragility of the oral mucosa and infants who are bottle-fed tend to burn easily, even if the temperature of the formula or milk is just slightly high. Burns also leave a relatively wide distribution of lesions14). Coupled with traumatic action on the border of the hard palate, this propensity is recognized to be a negative factor that may trigger occurrences of Bednar's aphthae or impede infants' recovery. In this study, one patient was found to possess a dentated lesion. The patient's history confirmed that the patient was bottle-fed with formula milk that was relatively high in temperature. The feeding went on for a week before the lesion was initially discovered. The lesion's size was 0.7 cm×0.5 cm, which is not particularly large. However, the lesion was relatively deep compared to the dentation, and the healing time was 1 month, which was longer than other cases.
Bednar's aphthae can be diagnosed by distinguishing it from other diseases that require medical tests or treatment71011). The lesion caused by an infection is generally accompanied by fever. Herpetic stomatitis is acutely, accompanied by fever, the presence of small and medium-sized lesion with involvement mainly of the gum and tongue. Lesion caused by the Coxsackie virus is acute installation and usually accompanied by fever, with the presence of large-sized lesion throughout the oral cavity. Hand foot mouth disease is oral lesion concomitant with vesicular lesions on hands and feet. Recurrent aphthous stomatitis, which is one of the oral lesions frequently found in children and youth, is small and circular surrounded by and erythematous halo and they affect the keratinized mucosa of oral cavity. Position of the lesions differs from that Bednar's aphthae, which affects the palate, and therefore, it is much easy to distinguish the two. In addition, Epstein's pearl, which is often found in newborns, is also localized along the border between the hard palate and soft palate, similar to that of Bednar's aphthae. It also centered in the midline, which makes it harder to distinguish from Bednar's aphthae. Therefore the appearance of the cysts has to be monitored for an accurate diagnosis.
The treatment was intended to eliminate factors with the potential to stimulate the mucosa. By enlarging the hole in the nipple of the bottle and by correcting the baby's position while nursing (keeping the infant in a semiseated position), repetitive stimulus on palate was eliminated. Established feeding habits were recovered within 3 to 4 days after changes were made. All sixteen patients demonstrated progress within a month of diagnosis. None of the patients were left with scars.
Extensive histories of feeding habits must be taken prior to making a diagnosis, but diagnoses can be made without any particular tests or treatment. Once diagnosed, an infant's mother must be properly trained in appropriate feeding position, nipple hole size, and use of pacifiers. By tracking patient progress, we can safely assume that Bednar's aphthae will heal spontaneously within one month of diagnosis. However, clinical suspicion is essential for the initial recognition of Bednar's aphthae.
In summary, Bednar's aphthae are seldom reported in the literature, although they are quite common in newborn infants. Bednar's aphthae are a benign disease and do not require any specific treatment. Thus, we should consider Bednar's aphthae when ulcerative oral lesions are observed so that unnecessary procedures can be avoided and simple, but effective solutions can be recommended to parents.
Notes
Conflicts of interest: No potential conflict of interest relevant to this article was reported.