Prevalence of restless legs syndrome and sleep problems in Korean children and adolescents with attention deficit hyperactivity disorder: a single institution study
Article information
Abstract
Purpose
Attention deficit hyperactivity disorder (ADHD) is a common disorder in school-aged children. Patients with restless legs syndrome (RLS) often present with ADHD symptoms and vice versa. This study was the first to attempt to identify the prevalence of RLS and sleep problems in children with ADHD in Korea.
Methods
Patients diagnosed with ADHD were asked to complete a sleep questionnaire. The sleep questionnaire included items to help identify the presence of four typical symptoms that are used as diagnostic criteria for RLS.
Results
A total of 56 patients, including 51 boys and 5 girls (mean age, 10.7 years old) participated. Of these, 24 complained of pain, discomfort, or an unpleasant sensation in the legs. Based on the RLS diagnostic criteria, 2 patients were diagnosed with definite RLS and 4 with probable RLS. There were no significant differences in age, medication dosage, or neuropsychological test scores between the patients with and without RLS symptoms.
Conclusion
Approximately 42.9% of patients with ADHD presented with RLS symptoms and 7.1% of these were diagnosed with RLS. Patients with ADHD also experienced various other sleep disorders. Thus, appropriate assessment and treatment for sleep disorders in patients with ADHD is essential.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a common neurobehavioral and psychiatric disorder present in 4% to 12% of school-aged children1,2). ADHD affects children of all ages, and it persists throughout adolescence3). Many patients with ADHD have comorbid disorders such as conduct disorders, anxiety disorders, mood disorders, learning disorders and sleep disorders4). Previous studies have shown that various sleep problems were reported by patients with ADHD5,6). The sleep problems most commonly reported are excessive daytime sleepiness and difficulties initiating and maintaining sleep7). Regarding sleep disorders, several studies have found a higher rate of specific sleep disorders including restless legs syndrome (RLS), periodic limb movement disorder and sleep apnea8,9,10). Meticulous attention is required in the assessment of ADHD patients because RLS patients can be misunderstood as ADHD patients, and ADHD can also be accompanied with RLS11). Since Picchietti et al.10) reported the association between ADHD and RLS in 1998, a number of studies have been conducted about the relationship. However, none have been reported in Korea. Therefore, this study was aimed to investigate the evidence on the association between ADHD and RLS and sleep problems in Korean children and adolescents with ADHD.
Materials and methods
The cross sectional study was carried out in the pediatric and Department of Psychiatry, Kyungpook National University Medical Center in South Korea between April to September, 2012. A sleep questionnaire administered in the Korean language was given to the children and adolescents with ADHD and their parents in the out-patient clinic.
1. Diagnosis of ADHD
Fourth edition, test revision of Diagnostic and Statistical Manual of Mental Disorders was used in diagnosis of ADHD.
2. Sleep questionnaire
Sleep questionnaire and RLS criteria for the subjects are shown in Table 1.
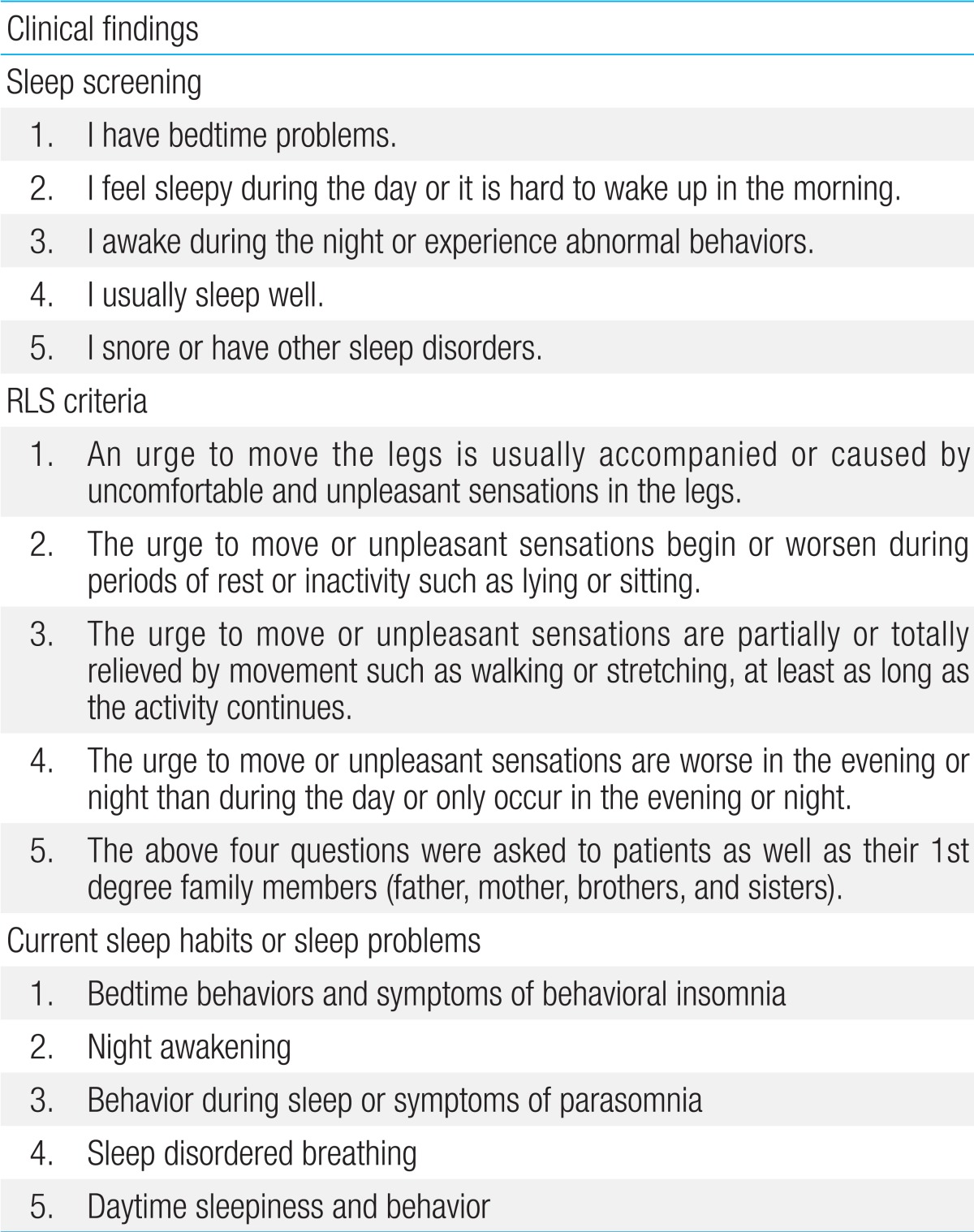
Sleep questionnaire items and RLS diagnostic criteria used for screening of participants
3. Case finding and data collection
We reviewed the respondents of the questionnaire and medical data of the patients. The medical records of the patients were reviewed focusing on the psychological test and treatment of ADHD.
4. Diagnosis of RLS
According to the diagnostic criteria of the International Restless Legs Syndrome Study Group12), when a child meets all the essential adult criteria and two additional criteria (a first degree family history of definite RLS, sleep disturbance for age) who is aged 12 and under was diagnosed to be "definite RLS". Another supportive criterion (periodic limb movements index ≥5 by polysomnography) was not applied for this study, because polysomnogram was not done in any patients. Adult diagnostic criteria were used for patients older than 13 years old. If a patient meets all the essential criteria except the criterion "The urge to move or unpleasant sensations are worse in the evening or night than during the day or only occur in the evening or night," and has a family history of definite RLS was diagnosed as "probable RLS".
5. Statistical analysis
Statistical analysis was performed using PASW Statistics 18.0 (SPSS Inc., Chicago, IL, USA). The average values of the two groups classified according to the presence of RLS symptoms were compared using the Mann-Whitey U test or t test.
6. Ethics statement
This study was approved by the Institutional Review Board for clinical research at Kyungpook National University Medical Center (2012-04-007). The aim of this study was explained in the first page of the sleep questionnaire and a formal consent was obtained from the patients and parents.
Results
1. Clinical characteristics of the subjects
Table 2 shows the clinical demographics of study subjects. The mean age of the patients was 10.7±2.7 years, and the mean treatment for the duration of medication for ADHD was 27.9±22.1 months.
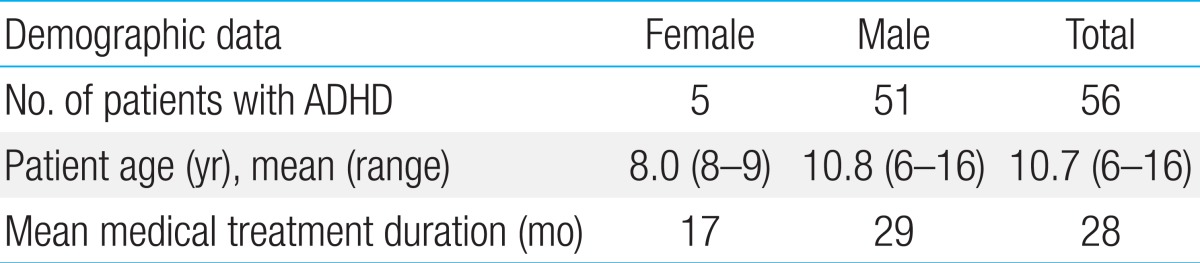
Demographic features of study participants
2. Prevalence of RLS of the subjects
Seven patients had a family history of RLS (12.5%) and 24 patients (42.9%) showed symptoms of RLS. The highest responses were made to the statement "An urge to move the legs, usually accompanied or caused by uncomfortable and unpleasant sensation in the legs", with 11 answers (19.6%), followed by "The urge to move or unpleasant sensations are partially or totally relieved by movement" which 10 patients (17.9%) answered to. There were 6 patients (10.7%) who answered to "The urge to move or unpleasant sensations begin or worsen during periods of rest or inactivity" and 6 patients (10.7%) who answered to "The urge to move or unpleasant sensations are worse in the evening or night than during the day or only occur in the evening or night" (Fig. 1). Assessing the subjects based on the sleep questionnaire, 2 patients (3.6%) were diagnosed with "definite RLS" and another 2 patients (3.6%) were diagnosed with "probable RLS".
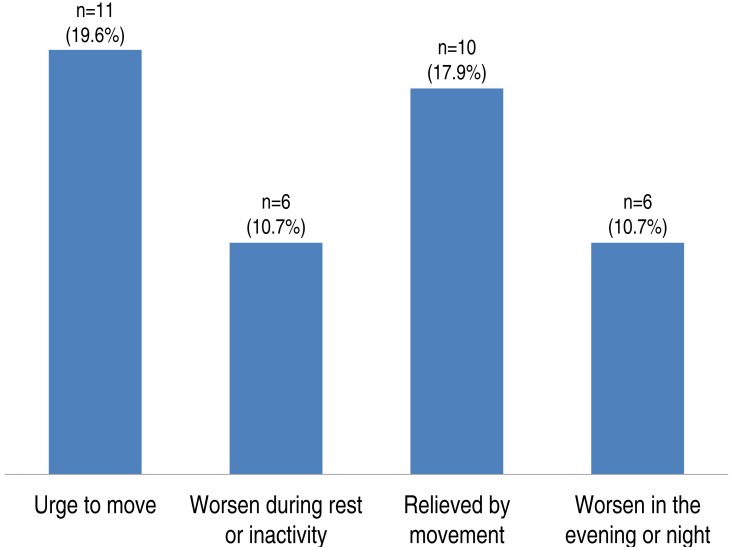
Prevalence of restless legs syndrome (RLS)-related symptoms in study patients. Twenty-four patients had symptoms of RLS. The symptoms "an urge to move the legs" and "relief by movement" were most common, followed by "worsening during rest" and "worsening in the evening or night."
3. Comparison of psychological results, treatment, sleep characteristics between patients with RLS symptoms and without RLS symptoms
There were no significant differences in intelligence quotient, ADHD scale, medication dosage and treatment duration between the groups. Regarding sleep characteristics such as sleep problems, sleep latency and total sleep time, we did not find any significant differences between two groups (Table 3).
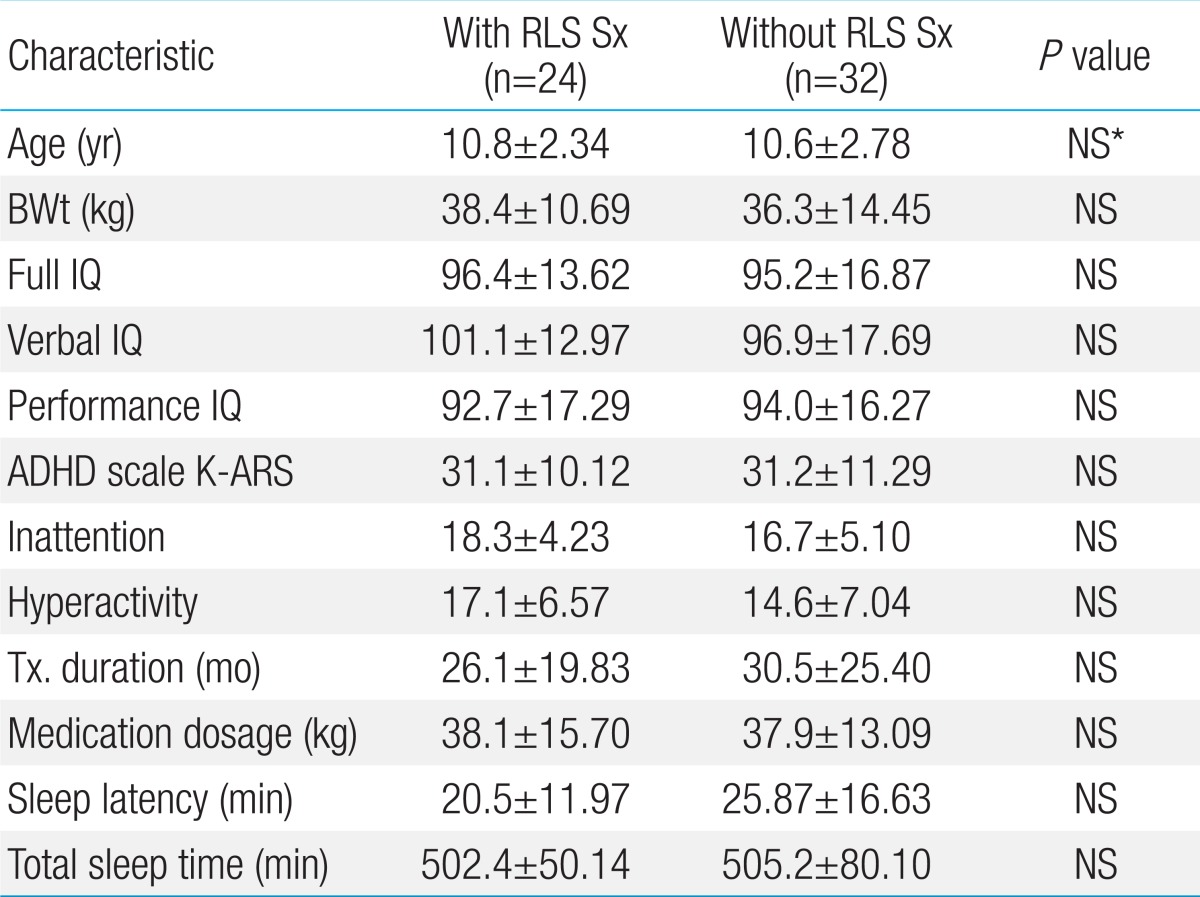
Comparison of sleep-related characteristics between patients with and without RLS
4. Sleep screening questions
Among patients with ADHD, sleep problems were observed in 42 patients (75%); with the highest response 35 patients (62.5%) answered to "Excessive daytime sleepiness"; 17 patients (30.4%) answered to "Bedtime problem"; 11 patients (19.6%) answered to "snoring"; 7 patients (12.5%) answered to "problems in Regularity and duration of sleep"; 4 patients (7.1%) answered to "Awakening during sleep" (Fig. 2).
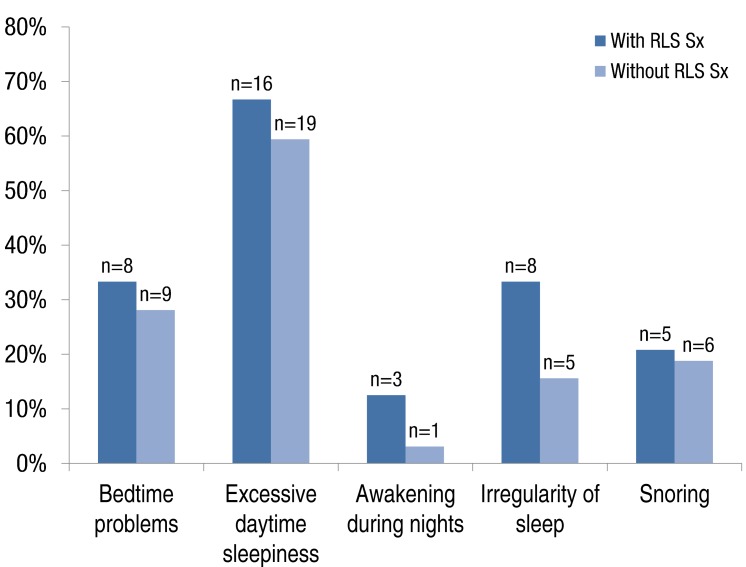
Sleep problems in the study patients. Sleep problems were observed in 42 patients (75%) among the subjects. Excessive daytime sleepiness was the most common symptom, followed by bedtime problems, snoring, irregularity of sleep, and awakening during the night. There were no significant differences between the two groups. RLS Sx, restless legs syndrome symptom.
5. Sleep problems in children and adolescents with ADHD
Twenty-nine patients had symptoms of behavioral insomnia, they complained that they felt afraid of sleeping on their own (n=25, 45%) or they tend to look for their parents when they go to bed. Four children showed night awakening and 27 patients had symptoms of parasomnia, they showed twisting or turning of the body (n=25, 45%), teech grinding (n=17, 30%), kicking legs (n=12, 21%). Thirty subjects had symptoms of sleep disordered breathing, such as mouth breathing (n=27, 48%) or snoring (n=10, 18%). Forty-five patients complained about daytime sleepiness, they showed unrefreshed sleep in the morning (n=43, 77%) or looking tired (n=33, 50%).
Discussion
The most important finding of this study is that considerable numbers of patient with ADHD may have RLS symptoms or be diagnosed with definite RLS. In this study, 42.9% of the subjects (n=24) had RLS symptoms and 7.2% of the subjects (n=4) were diagnosed with probable or definite RLS. Considering the fact that RLS symptoms can be mild and intermittent in children and RLS is usually progressive13,14), it is expected that the numbers of RLS patients will increase during follow-ups. The first study on the comorbidity between ADHD and RLS, conducted with 69 children with ADHD by Picchietti et al.10) in 1998, showed that 11.5% of the patients with ADHD had RLS according to the pediatric version of the diagnostic criteria for RLS. A study of Konofal et al.15) for 43 children with ADHD reported that 44% of the study subjects met RLS diagnostic criteria. Other studies also reported that RLS symptoms were seen in 10.5%-24% of ADHD children11,16,17). Compared to 2%-2.74% of the prevalence in the general population18,19), children with ADHD are more likely to experience RLS. In this study, there were 24 patients who complained of RLS symptoms (42.9%) and 7% of the subjects (n=4) were diagnosed with RLS based on the symptoms which was similar to previous studies.
Although the association between RLS and ADHD are not yet clearly understood, several hypotheses have been suggested. Some maintain that ADHD is resulted from sleep disturbance secondary to RLS. While sleep deprivation in adults causes excessive daytime sleepiness, sleep deprivation in children can lead to inattentiveness and paradoxical overactivity20,21). In our study, 86% of the subjects (n=42) complained of sleep disturbance. Of them, problematic bedtime behaviors and symptoms of insomnia were seen in 52% (n=29) and kicking legs while sleeping was seen in 21% of the subjects (n=12). It is known that adolescents with ADHD experience sleep disturbance 2-3 times more compared to normal healthy children22). It is also reported that sleep disorders should be included in the assessment and treatments of ADHD patients since a prognosis and treatment response of ADHD can be affected by various sleep disorders including RLS7). Comparision between patients with RLS symptoms and without RLS symptoms showed that the former had more sleep problems, however there were no statistical significances (Fig. 2). Polysomnographic studies of RLS reported increased sleep latency23), but in the present study, patients with RLS showed decreased sleep latency. This study was based on sleep questionnaires, so objective examinations such as PSG or actigraphy are needed to verify these results.
Another hypothesis is that the manifestations of RLS could be misclassified as ADHD symptoms10). Children with RLS can be mistaken as ADHD patients because they move about without being able to stay still due to an urge to move and present with a lack of attentiveness secondary to leg discomfort24). A study conducted with adults with RLS also showed that RLS patients increased inattention and hyperactivity25). Since separate treatments for RLS is required if a patients is accompanied with RLS, RLS screening should be included in assessment of ADHD. With recent increasing interests in ADHD, the condition has been recognized as a public health problem. Therefore, clinicians should also be aware of the significance of RLS. Others suggest that either RLS is comorbid with ADHD or RLS and hyperactivity have a common central nervous system pathophysiology. Several studies have shown decreased dopaminergic function in patients with ADHD26,27) or iron deficiency in children with ADHD28). According to these theories, administration of iron supplements and dopamine agonists should be considered in addition to methylphenidate. Therefore it is needed to evaluate the iron status for iron deficiency in ADHD patients with RLS symptoms and consider iron therapy for them. And we need to check whether RLS symptoms improved or not after iron supplementation. Whereas previous studies have reported that ADHD symptoms are more severe when patients with ADHD have both conditions29,30) and are absent of RLS symptoms31), there was no statistically significant difference in this study.
In our study, it was difficult to identify whether ADHD symptoms are resulted from RLS or RLS symptoms are caused by ADHD or RLS and ADHD were concurrent in patients with RLS symptoms and patients diagnosed with RLS. Therefore, further evaluation and managements for RLS will be required to clarify these.
It is shown that children and adolescents with ADHD are more likely to experience sleep disorders compared to the normal healthy population with the same age22). This has been proven both in subjective evaluation and objective examination32,33).
The subjects of this study also complained of various sleep problems such as bedtime resistance, sleep onset difficulties, difficulties with morning awakening, daytime sleepiness. Moderate and severe sleep problems lower the quality of living for ADHD patients as well as other members of the family6,34). Thus, adequate treatments will be essential. This research was a cross-sectional observational study, we didn't try any treatment for the sleep problems. However, education or teaching good sleep hygiene help the children with sleep problems, so we need to consider behavioral therapy for sleep disorders.
It is practical to assess sleep problems prior to the commencement of drug therapy in patients with ADHD because it is tricky to differentiate whether sleep problems are primarily associated with ADHD or are associated with drug therapy when ADHD patients on medication complain of sleep problems.
Compared to an increasing interest in ADHD, sleep disorders and RLS in children are much less acknowledged, which make it difficult to diagnose and provide appropriate treatments.
This study is the first study concerning the relationship between sleep problems and RLS in children and adolescents with ADHD conducted in Korea. However, there were some limitations which need to be addressed. First of all, the influence of drug therapy was not excluded. In addition, objective tests such as PSG or iron workup were not performed for the subjects. The study sample was also small and there was an absence of a control to compare. Nonetheless, it was acknowledged that sleep problems should be assessed and identified prior to the diagnosis and treatment of ADHD because a considerable number of ADHD patients were suffered from RLS symptoms and were actually diagnosed with RLS. In this study, there were no significant differences in the medication dosage and neuropsychological test between patients with RLS symptoms and patients without RLS symptoms, which were thought to be stemmed from the small sample size. Therefore, larger studies will be required in the future to validate this result.
Acknowledgments
This study was performed at Kyungpook National University Medical Center, Daegu, Korea. The authors are grateful to all patients and their parents for completion of questionnaire. The authors are also grateful to Ms. Hyungi Kwon for her work in questionnaire preparation.
Notes
No potential conflict of interest relevant to this article was reported.