Complete rooming-in care of newborn infants
Article information
Abstract
Purpose
In Kyung Hee East-West Neo Medical Center, Seoul, Korea, efforts to raise rooming-in care success rate have been undertaken since when the hospital was established in 2006. We intended to analyze our experience over the past 3 years of period and to discuss the advantages of rooming-in.
Methods
We analyzed the rooming-in practice rate, failure rate, and the breast feeding rate. Subjects were 860 normal healthy neonates from June 2006 to June 2009.
Results
Among these 860 cases, 83 babies were required separation out of rooming-in in the middle of the course. Among these 83 cases, 70 cases had to stop the course due to poor condition of babies and 13 cases due to maternal condition. 70 cases of infant's causes consist of 68 cases of NICU admission and 2 cases of poor feeding support. The other 13 cases of separation include refusal by maternal condition. Therefore the success rate of rooming-in for the last 3 years was 90.3%, that is 777 cases among the total 860 cases. The percentage of exclusive breast feeding was 64%, that of mixed feeding with breast and formula feeding was 25%, and formula feeding only was 11%.
Conclusion
We experienced successful rooming-in care for the last 3 years. Nursery facilities should educate and encourage the advantages of rooming-in, including the good formation of attachment between mother and infant, emotional stability, protection from infection, and increased breast feeding rate so that rooming-in care can be fully established.
Introduction
Nursery care of normal newborn infants in hospitals nowadays differs place to place. There are three types of nursery care facilities in Korea. First, completely separated nursery room between mother's and baby's. In this circumstance, mothers can spend time with their babies at limited meeting times for several minutes during their hospital stay. The entire course of care is given in the nursery room only. Second, partial rooming-in with mothers. Rooming-in nursery service gives opportunity for babies to spend time with their mothers during their hospital stay, and the partial rooming-in gives not full time but partial time in a day for them because main procedures are taken in the nursery room not mother's room. In the past in Korea, many of nursery facilities adopted completely separated nursery room services, but nowadays partial rooming-in type has become the majority. Last type of care is complete rooming-in care of babies and mothers. This nursery practice gives care for baby in the same room with mother from their time of birth to their discharge from the hospital. Recently in Korea this type of service is emerging but only in a minority of cases (Fig. 1).
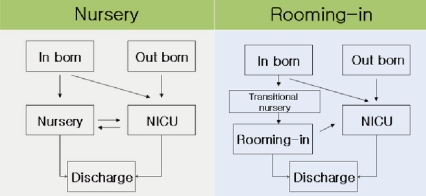
Flow chart of traditional nursery (left), rooming-in (right), and mixed two types (partial rooming-in) after birth in filed of normal infants care.
It is widely accepted that the rooming-in care has many advantages. Direct skin-to-skin contact on mother's chest gives protection from infection, emotional stability, maximized mother to baby interaction with joy. It provides more opportunity for successful breast feeding and opportunity for good acquisition of understanding baby's natural physiology for their mother. Mothers can be more confident when they go back home to raise their own baby. On the other hand, many mothers complain pain and discomfort right after their delivery so, complete rooming-in service is not popular among Korean mothers as of yet.
Kangaroo mother intervention or kangaroo mother care was introduced in 1978 in Colombia, which is characterized by direct skin-to-skin contact (kangaroo position), exclusive or nearly exclusive breastfeeding (kangaroo nutrition), and early discharge (kangaroo discharge policy). Several studies showed that kangaroo mother intervention (KMI) has advantages for the baby's emotional stability, increased successful breast feeding and decreased neonatal morbidity1-7). In this aspect, rooming-in circumstance is very important for successful KMI practice. 'The ten steps for successful breast feeding' from Baby-Friendly Hospital Initiative (BFHI), WHO/UNICEF, recommends early breast feeding within 30 minutes after birth with complete rooming-in care for the first 24 hours8). And also, American Academy of Pediatrics and American College of Obstetricians and Gynecology recommend complete rooming-in.
In Korea, we have assessed items for quality improvement of hospitals especially for maternity and neonate section from 2007 by Korean Hospital Association, which is expressed by efforts of trial in breast feeding, methods and contents of feeding. This is assessed by number of breast feeing trials in each 1, 6, 12, 24 hours after delivery in case of vaginal delivery, and 3, 6, 12, 24 hours in case of cesarean section. The feeding method contains sucking trials of baby, cup or spoon feeding, and additional feeding content such as water or dextrose water. In this aspect, it is essential to establish the rooming-in care service system to improve postnatal care quality. Since opening in 2006, in Kyung Hee University East-West Neo Medical Center, we did not run a separated nursery room for normal babies, we have been taking care of the normal baby in the same room as the mother soon after the observation of baby's vital sign during the first 3 hours in the transitional nursery. During rooming-in stay, routine procedures with pediatrician rounding everyday are given to the baby at each room.
Materials and methods
Subjects were 860 normal neonates delivered at Kyung Hee University East-West Neo Medical Center who were placed in rooming-in service after birth from June 2006 to June 2009. The aim of this study was to report and evaluate the rate of rooming-in practice and breast feeding success rate, and to analyze the reasons behind rooming-in failure, the cause of administration to NICU to better understand the advantages of this system.
Results
1. Practice rate of rooming-in service
Subjects were 860 neonates, who were required to be under rooming-in service and delivered at Kyung Hee University East-West Neo Medical Center from June 2006 to June 2009. We excluded diseased babies administered into NICU since birth. Total subjects were under rooming-in service since birth, and among these 860 cases, 83 babies were required separation out of rooming-in in the middle of the course. Among these 83 cases, 70 cases had to stop the course due to poor condition of babies and 13 cases due to maternal condition. 70 cases of baby's cause consisted of 68 cases of NICU administration and 2 cases of poor feeding support. The other 13 cases of separation included refusal by maternal complaint (n=2), teen-age delivery or adoption (n=2), far distance of mother's VIP ward (n=1) and maternal postpartum disease and poor condition (n=8), so in these conditions rooming-in was not possible. Therefore because of these 13 cases, the rooming-in practice rate during these 3 years was 98.5% (847 cases) among total 860 cases. 777 cases completed the rooming-in service successfully (90.3%) (Table 1).
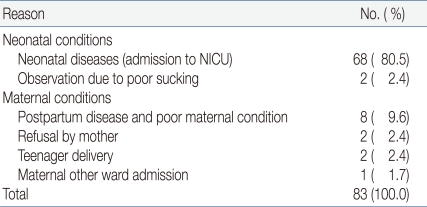
Reasons for Failure of Rooming-in Care
2. Causes of rooming-in failure
Total failure was counted as 83 cases (9.7% of total 860 cases). For the analysis of the failure, rooming-in practice failure was considered as any kind of refusal due to maternal condition (13 cases). This included refusal by maternal complaint (n=2, 2.4%), teen-age delivery or adoption (n=2, 2.4%), far distance of mother's other ward (n=1, 1.7%) and maternal postpartum disease and poor condition (n=8, 9.6%) (Table 1).
Rooming-in completion failure was defined by all kinds of separation from the mother because of baby's poor medical condition. This included transfer to NICU (n=68, 80.5%) and poor feeding support (n=2, 2.4%). In case of transfer to NICU, there were 37 cases of neonatal jaundice, 7 cases of acute viral enteritis, 3 cases of each hypoglycemia and hydronephrosis, 2 cases of each volvulus, nonspecific vomiting, suspicious sepsis, and aspiration pneumonia (Table 2).

Causes of Admission to Neonatal Intensive Care Unit
3. Patterns of breast feeding
The percentage of exclusive breast feeding was 64%, that of mixed feeding with breast and formula feeding was 26%, and formula feeding only was 10%. Comparison of feeding pattern for those 3 years of this study showed increased breast feeding rate in 2009 (Table 3). In mixed feeding group, the frequency of formula feeding was not so high. Formula feeding less than 3 times a day was 78.0% and only one time was 34.0% (Table 4). Therefore it is assumed that breastfeeding was a main pattern even in mixed feeding groups.
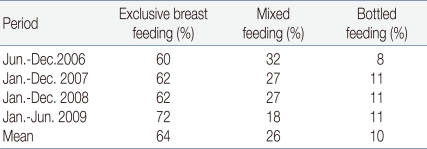
Types of Feeding according to the Annual Period
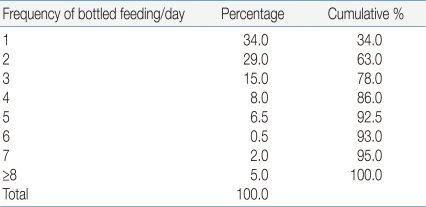
Sub-division of Mixed Feeding
Discussion
Rooming-in care is defined by WHO guideline that baby and mother stay together in the same room at night and day in the hospital, there should not be any limitation of direct contact between two of them8). The recommendation of WHO encourages an entire 24 hours of staying together.
The whole 24 hours is encouraged by the recommendation of WHO as well as by 'The ten steps to successful breastfeeding' from BFHI of WHO/UNICEF. BFHI is one of breast feeding encouraging programs, and it has supported many mothers who want to start breast feeding to be confident. It gives recognition to hospitals which help and support these efforts as a BFH. Also BFHI recommends the ten steps for successful breast feeding to hospitals and support rooming-in care service. A website has been published regularly with the latest renewal of this recommendations in 20098) The American Academy of Pediatrics and American College of Obstetricians and Gynecology favor complete rooming-in over separated nursery room.
The present study described that the rooming-in practice rate of Kyung Hee University East-West Neo Medical Center for the last 3 years was 98.5%, which came from 847 cases besides 13 cases of maternal problem. When 68 cases of completion failure due to neonatal medical problem are excluded, 777 cases were completely rooming-in success without any interruption9, 10).
In a review of a report by Cho et al. in 199911) the rooming-in practice rate was only 25%, and separated rooming was 75% high. Compared with this study, that of the present study (98.5%) was very high. We speculate that it is because we closed any kind of normal nursery room and provided only rooming-in service in cases of normal healthy babies, educated the expectant mothers before delivery as well as staffs of our hospital. The advantages WHO mentioned are that it is cost effective, less instruments are required, there is no need of additional man power, low rate of infection, support of breast feeding and encourages the attachment between mother and baby8). There is a report that rooming-in care significantly decreased morbidity of otitis media, diarrheal disease for the next 6 years as well as neonatal sepsis and meningitis12).
Ahn et al. reported in the study of the effect of rooming-in care on the emotional stability of newborn infants, that neonates who experienced rooming-in care, showed more early recovery from external irritating stimulus13). Song et al.14) described that attachment between mother and baby should be enhanced in order to encourage the participation in rooming-in care. Kim and Park15) examined the maternal attitude and confidence for infant care, and reported that rooming-in facilities provided primipara with more positive maternal attitude and greater self confidence for infant care and increased the rate of breast feeding.
Cochrane database has summated and analyzed KMI data. In their several reviews, they reported in 2003 that rooming-in care had clinical advantages especially in breast feeding and baby's crying from early skin-to-skin contact, and there was no short term negative influence4). Also in 2007, they reported that rooming-in care showed advantages in breastfeeding, early attachment formation, baby's crying and cardiopulmonary stability and there was no short and long term negative influence5). In aspect of low birth weight infant, rooming-in provided decreased morbidity in their 2006, 2007 reports6, 7).
Charpak et al. explained that KMI contributed to growth stimulation and decreased morbidity2). In the latest study, Bystrova et al reported that early skin-to-skin contact with early sucking influenced positive mother-infant interaction during 1 year of follow-up period3).
In spite of numerous advantages of rooming-in care, some postpartum mothers complain of the burden of caring the infant and fatigue and avoiding rooming-in. This explains almost all failures of rooming-in in Korea. But, Song16) explained that there was no significant difference in degree of physical and emotional fatigue between rooming-in group and non rooming-in group of normal vaginal delivery mothers. It appeared that there was an prejudice against rooming-in practice when postpartum mothers made the decision. And the author suggested data to help correcting this prejudice and insisted the importance of rooming-in care.
In our study, separated care in the middle of rooming-in was required in 83 cases (9.7%). Among these, 68 infants were administrated in NICU because of their medical problems. There were 37 cases of neonatal jaundice, 7 cases of acute viral enteritis, 3 cases of each hypoglycemia and hydronephrosis, 2 cases of each volvulus, nonspecific vomiting, suspicious sepsis, and aspiration pneumonia. In speculation of neonatal jaundice which was a major cause of rooming-in interruption, we suggest the introduction of rooming-in phototherapy such as fiber-optic pad or blanket type. With such efforts, we can expect an improvement in both successful rooming-in and participation rate.
There are numerous research supporting that rooming-in increases breastfeeding rate. Infants in the same room with mother's have more chances of breastfeeding. Yamauchi et al. demonstrated higher breast feeding rate in rooming-in group compared with non rooming-in group in 199017). There are similar reports such as a systemic review by Fairbank et al. in 200018), report in cesarean section birth by Merten et al. in 200719), and a study about informative support by Grochans et al20). They recommended KMI and rooming-in care. WHO/UNICEF recommends breast feeding in first 30 minutes of life with rooming-in care. It is widely believed that BFHI which was designed by WHO/UNICEF has contributed increased breastfeeding rate for last 25 years21, 22). It was started from 1992 in Korea, 48 hospitals have been titled as baby friendly hospital by 2008. Kim et al. compared breastfeeding rate between BFHI and non-BFHI in the year of 10 years of BFHI movement in Korea, and reported higher rate of breastfeeding in BFHI hospitals23).
We reported in this study that the percentage of exclusive breastfeeding was 64%, that of mixed feeding with breast and formula feeding was 26%, and formula feeding only was 10%. Nearly exclusive breastfeeding was main pattern even in mixed feeding cases, in which bottled formula feeds were only 1 to 3 times a day. Therefore if only some more intervention can be provided, breastfeeding rate will be increased. In fact, as our analysis showed, the success rate increased in 2009, and it is assumed that this increase was due to active intervention efforts. The exclusive breast feeding rate of rooming-in circumstance in our study (64%) was much higher than that of the period from 1993 to 1995 in Korea, which was reported as 57.4% by Lee et al24). They compared breast feeding rate between rooming-in group and non rooming-in group, which were 57.4% and 39.1% each. In the same way Kim et al.25) reported 42.4% and 36.1% each in 2003. Wang and Kim26) researched the effect of rooming-in on breast feeding rate especially in case of primipara. They revealed that rooming-in was most important factor which influenced breast feeding of primipara. On the other hand, Grasso et al.27) demonstrated that rooming-in had significant influence that increased efficacy of neonatal hearing loss screening.
In conclusion, we experienced successful rooming-in care for the last 3 years. Nursery facilities should educate and encourage the advantages of rooming-in such as good formation of attachment between mother and infant, emotional stability, protection from infection, and increased breastfeeding rate so that rooming-in care can be established completely.