Time to pay attention to anemia in female adolescents
Article information

Anemia is a relatively common disease. According to the World Health Organization, between 1993 and 2005, about a quarter of the world’s population had anemia, and it was more prevalent among preschool children and women [1].
In anemia, oxygen transport is impaired owing to a decrease in circulating red blood cells and, consequently, hemoglobin levels. Causes of anemia include hereditary hemolytic anemia, infection, and deficiencies in nutrients such as iron, vitamin B12, and folate.
In the 2000s, the worldwide prevalence of anemia decreased. This study investigated the change in the patterns of anemia in Korean adolescents from 1998 to 2018 using data from the Korea National Health and Nutrition Examination Survey. They found that the incidence of anemia in children 10–18 years of age in Korea is decreasing. Interestingly, among these adolescents with anemia, there were 9 times more females than males. In particular, the prevalence of anemia in women after menarche was 3.6-fold greater than that in women before menarche. In addition, their study confirmed that the prevalence of anemia slightly decreased with increasing body mass index and household income.
According to a Japanese study, the prevalence of anemia among healthy women <50 years old was 22.3%, of which 25.2% had severe anemia [2]. This suggested there is a need for increased interest in women’s health.
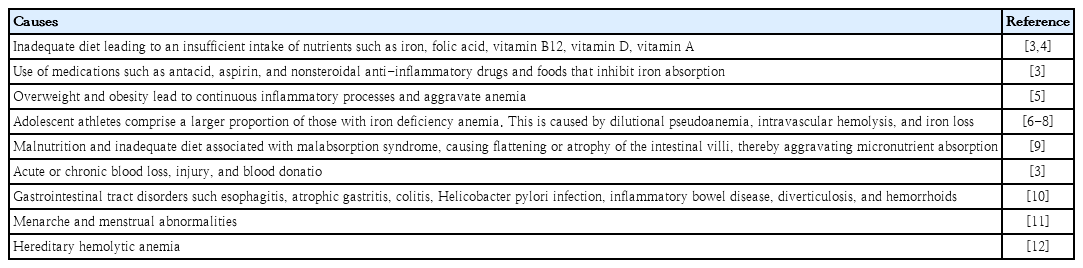
The major causes of anemia in adolescents are summarized in Table 1. Nutritional insufficiency, chronic blood loss, gastrointestinal disorder such as gastritis, infection, inflammatory bowel disease, and gynecological problem can cause anemia. Hemolysis due to red blood cell membranopathy, hemoglobinopathy, or enzymopathy can also cause anemia. Iron deficiency is the most important of the various causes of anemia. Menstruation is an important cause of blood loss, especially in adolescent females, and although iron intake is important, it is easy to overlook. Nutritional counseling and health management are crucial for school-age children. Campaigns or educational materials may be helpful in fulfilling these goals. In addition, if anemia persists, a pediatric hematologist should be consulted.
Factors contributing to anemia in adolescents
Notes
No potential conflict of interest relevant to this article was reported.