Impact of lifestyle factors on trends in lipid profiles among Korean adolescents: the Korea National Health and Nutrition Examination Surveys study, 1998 and 2010
Article information
Abstract
Purpose
Only a few studies have explored nationwide trends in lipid profiles among Asian adolescents. We aimed to assess trends in lipid profiles and the associated lifestyle factors among Korean children.
Methods
We analyzed data for 2,094 adolescents who were aged 10–18 years and had participated in the Korea National Health and Nutrition Examination Surveys in 1998 and 2010.
Results
During 1998–2010, the prevalence of obesity significantly increased in boys, but no changes were observed in girls. Over this period, there was a small but significant decrease in the mean low-density lipoprotein (LDL)-cholesterol level in boys (1998, 87.5 mg/dL; 2010, 83.6 mg/dL; P=0.019) and mean triglyceride levels in girls (1998, 90.8 mg/dL; 2010, 85.8 mg/dL; P=0.020). There were no significant changes in the prevalence of dyslipidemia in boys, but a modest decrease was noted in girls (1998, 25.1%; 2010, 18.3%; P=0.052). During the study period, the prevalence of breakfast skipping decreased, whereas that of regular exercise increased in both groups. Daily total energy intake did not change between these years. In multivariable logistic regression analyses, breakfast skipping was associated with increased risk of hyper-LDL-cholesterolemia in boys (odds ratio [OR], 5.77) and hypertriglyceridemia (OR, 2.27) in girls. Regular exercise was associated with decreased risk of hypo-HDL-cholesterolemia (OR, 0.40) in boys.
Conclusion
Although the prevalence of obesity in boys increased, favorable or constant trends in lipid profiles were observed among Korean adolescents during 1998–2010. Decrease in breakfast skipping and increase in regular exercise may have contributed to these trends.
Introduction
The prevalence of obesity in children and adolescents has increased dramatically worldwide in the past three decades. The Fels Longitudinal Study showed that obesity indices, including body mass index (BMI), waist circumference/height, and percent body fat, are significantly higher in adolescents born in the 1990s than in those born in previous decades in the United States (US)1). With the rapid economic growth in Korea, the prevalence of childhood obesity has increased from 2% in the 1980s to 9.7% in 20052).
Growing evidence indicates that obesity in early life is one of the strongest risk factors for dyslipidemia, which increases the risks for cardiovascular disease in adulthood3). As the adolescent and childhood obesity epidemics increase the health burden, trends in blood lipid levels and dyslipidemia in teenagers are drawing public attention. A large-scale study in the US reported that the prevalence of dyslipidemia among adolescents was 24% between 1999 and 20044). Recently, though, decreases in low-density lipoprotein (LDL) cholesterol and triglycerides among US adolescents were observed over a 10-year period (1999–2008)5). Other recent studies in the United Kingdom6) and Russia7) also reported favourable trends in the lipid profiles of adolescents. In contrast, studies of Canadian8) and Iranian adolescents9) showed unfavourable trends in lipid profile components. In a recent study of Japanese adolescents, no secular changes were observed in blood lipid levels between 1993 and 200810).
Although the prevalence of dyslipidemia in adolescents and its associated risk factors have been investigated in several countries5810) very little is known about nationwide trends in lipid profiles and associated factors in Korean adolescents. Using data from the Korea National Health and Nutrition Examination Surveys (KNHANES), our study provides current and comprehensive information on the trends in lipid profiles and associated risk factors (BMI, obesity, diet, exercise, smoking, and alcohol consumption) among Korean adolescents aged 10–18 years, from 1998 to 2010.
Material and methods
1. Study subjects
Data were obtained from the KNHANES, a nationally representative, cross-sectional survey of the health and nutritional status of Korean civilians, conducted in 1998 and 2010, by the Korean Ministry of Health and Welfare. Details of the design of the KNHANES are available on the KNHANES website (http://knhanes.cdc.go.kr). Briefly, noninstitutionalised Korean civilians were selected by a stratified, multistage probability sampling design. In the 1998 and 2010 surveys, up to 90% of participants completed a standardized face-to-face interview by trained interviewers, which covered demographic, socioeconomic, dietary, and medical history, and a health examination was conducted. This study analysed the data of participants aged 10–18 years who attended an interview regarding dietary intake, alcohol consumption, smoking, and physical activity. The participants underwent a health examination that included anthropometric measurements and blood analyses. We excluded individuals who did not have blood samples for lipid profiling and those whose fasting time prior to blood sampling was insufficient (less than 10 hours). The sample for the cross-sectional analyses comprised a total of 1,104 boys (661 from 1998 and 443 from 2010) and 987 girls (617 from 1998 and 370 from 2010). The institutional review board at the Korea Centers for Disease Control and Prevention approved the study protocol, and all the subjects in this survey signed informed consent forms.
2. Anthropometric and biochemical indices
Experienced examiners performed anthropometric measurements. Height was measured to the nearest 0.1 cm on a stadiometer (Seriter, Holtain Ltd., Crymych, UK, in 1998; SECA 225, SECA Deutschland, Hamburg, Germany, in 2010). Body weight was measured to the nearest 0.1 kg on a balance beam scale (Giant 150N, HANA, Seoul, Korea), with the subject wearing light clothing and no shoes. BMI was calculated as the body weight divided by the square of the height (kg/m2). Waist circumference, defined as the narrowest point between the lower borders of the rib cage and the iliac crest, was measured to the nearest 0.1 cm following the end of a normal expiration. Obesity level was categorized according to the age and sex specific percentiles for BMI of national reference standards11). Normal weight, overweight, and obese were defined as a BMI percentile of <85th, ≥85th but <95th, and ≥95th respectively.
Dietary assessment of daily energy intake was performed in subjects through a 24-hour recall interview. Breakfast skipping was defined as regularly not eating breakfast more than 5 times per week. Alcohol consumption was categorized as "Yes" when the subjects reported a consumption of alcohol more than once per month in the 1-year period preceding the interview. Smoking was categorized as "Yes" when the subjects reported smoking more than once per month in the 1-year period preceding the interview. Physical activity was self-reported using the International Physical Activity Questionnaire. Regular exercise was categorized as "Yes" when the subjects reported moderate physical activity for more than 20 minutes at a time and more than 3 times per week. Moderate physical activity was defined as physical activity that causes a slight increase in breathing or heart rate, and includes activities such as carrying light loads, bicycling at a regular pace, or playing doubles tennis.
3. Laboratory analysis
Fasting blood samples were obtained from the antecubital vein following a 10-hour overnight fast. In 1998, the fasting plasma concentrations of total cholesterol, LDL-cholesterol, triglycerides, and high-density lipoprotein (HDL) cholesterol were measured enzymatically using a 747 Chemistry analyser (Hitachi, Tokyo, Japan). In 2010, the fasting plasma concentrations of total cholesterol, triglycerides, and HDL cholesterol were measured enzymatically using a Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan). Most of the LDL-cholesterol levels in 2010 were calculated with the Friedewald equation (total cholesterol – [HDL-cholesterol + triglycerides/5]). Only for the samples with triglycerides greater than 400 mg/dL, LDL-cholesterol were measured using a Hitachi Automatic Analyzer 7600 (Hitachi). The diagnostic cutoff points for adolescent dyslipidemia were based on guidelines from the American Heart Association12) and the National Cholesterol Education Program (NCEP)13).
Hypercholesterolemia was defined as total cholesterol levels>200 mg/dL, hypo-HDL-cholesterolemia was defined as HDL-cholesterol levels<40 mg/dL, and hypertriglyceridemia was defined as triglyceride levels>150 mg/dL. Hyper-LDL-cholesterolemia was defined as LDL-cholesterol levels>130 mg/dL. Dyslipidemia was diagnosed when subjects have at least one of hypercholesterolemia, hypertriglyceridemia, hyper-LDL-cholesterolemia, and hypo-HDL-cholesterolemia.
4. Statistical analysis
All data analyses were conducted using SAS ver. 9.2 (SAS Institute Inc., Cary, NC, USA). Survey design parameters, including clusters, stratums, and weights, were utilized in all statistical analyses. Information of nonparticipants was included in weighting of the statistical weighting. Therefore, the means and prevalence estimated in this study represented the overall estimates for the total Korean population aged 10–18 years. PROC SURVEYMEANS and PROC SURVEYFREQ were used to estimate means and prevalence, respectively. PROC SURVEYREG and PROC SURVEYFREQ were used to assess the differences in continuous and categorical variables, respectively, between genders and between the 1998 and 2010 populations. Multivariable logistic regression analyses, using PROC SURVEYLOGISTIC, were conducted to assess the associations of dyslipidemia with obesity level, central obesity, breakfast skipping, alcohol consumption, smoking, and regular exercise. For all analyses, P values were 2-tailed and <0.05 was considered statistically significant.
Results
The age and anthropometric measurements of the participants are presented in Table 1. In boys, the mean height, BMI, and waist circumference increased across the study years. Prevalence of overweight (from 8.4% to 12.5%) and obesity (from 3.9% to 7.3%) also increased significantly. In contrast, no significant changes were observed in mean BMI and the prevalence of overweight or obesity in girls.

Anthropometric measurements of the participants according to sex and study year
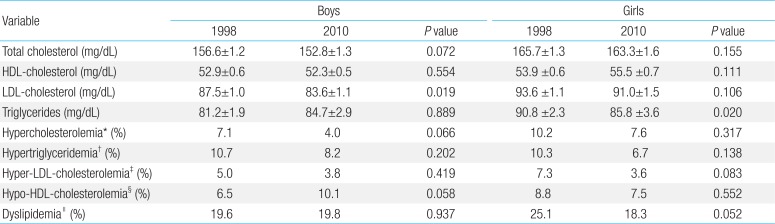
The trends in the blood lipid profile and prevalence of dyslipidemia are presented in Table 2. Between 1998 and 2010, mean LDL-cholesterol levels decreased from 87.5 mg/dL to 84.7 mg/dL in boys (P=0.0189), whereas mean triglyceride levels decreased from 90.8 mg/dL to 85.8 mg/dL in girls (P=0.020). There was no significant change in total cholesterol and HDL-cholesterol levels in either boys or girls. There were no significant changes observed in the prevalence of dyslipidemia in boys, whereas a modest decrease was noted in girls (25.1% in 1998, 18.3% in 2010; P=0.052).

Lipid profile of the participants according to sex and study year
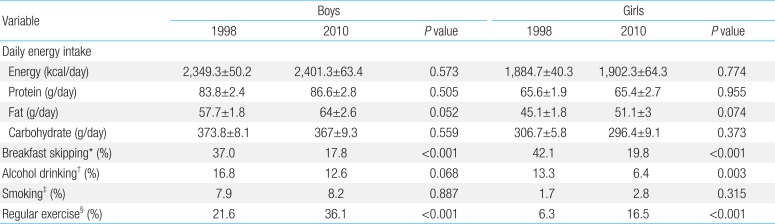
Lifestyle characteristics of the participants are presented in Table 3. There were no changes in total energy, protein, or carbohydrate intake in boys and girls; however, fat intake was marginally increased in both genders. The prevalence of breakfast skipping markedly decreased in both genders (P<0.001). The prevalence of alcohol consumption also decreased in both genders, although a significant difference in consumption was observed only in girls (P=0.003). Although the prevalence of regular exercise significantly increased from 1998 to 2010, the prevalence of smoking did not change in either gender.

Lifestyle characteristics of the participants according to sex and study years
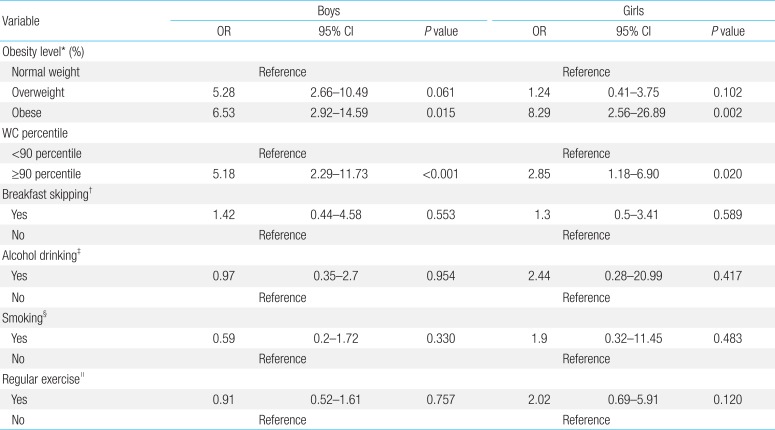
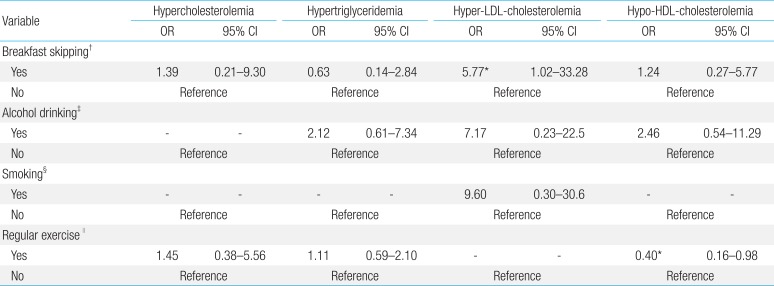
In multivariable logistic regression analyses adjusted for age (Table 4), risk factors for dyslipidemia were obesity stratified by BMI percentile and central obesity (waist circumference≥90th percentile). After adjusting for age, obesity level, daily energy intake, and percent energy from fat (Tables 5 and 6), breakfast skipping was associated with increased risk for hyper-LDL cholesterolemia (odds ratio [OR], 5.77; 95% confidence interval [CI], 1.02–33.28), whereas regular exercise was associated with decreased risk (OR, 0.40; 95% CI, 0.16–0.98) for hypo-HDL-cholesterolemia in boys (Table 5). In girls, breakfast skipping increased the risk of hypertriglyceridemia (OR, 2.27; 95% CI, 1.02–5.31), with no additional lifestyle factors involved in the risk of dyslipidemia.

Age-adjusted odds ratios for dyslipidemia according to multivariable logistic regression analyses

Age, body mass index, daily energy intake, and percent energy from fat adjusted odds ratios for dyslipidemia in boys according to multivariable logistic regression analyses

Age, body mass index, daily energy intake, and percent energy from fat adjusted odds ratios for dyslipidemia in girls according to multivariable logistic regression analyses
Discussion
In this study, we demonstrated favourable or constant trends in lipid profiles among Korean adolescents from 1998 to 2010, despite increased prevalence of obesity in boys. This result is interesting because the association between obesity and unfavourable lipid status has been well established in multiple studies38). A population study of Canadian adolescents8) reported that both mean total cholesterol levels and the prevalence of hypercholesterolemia were increased with increasing obesity prevalence, between 2002 and 2008. Similarly, increases in overweight and abdominal obesity were accompanied by the increased risk of hypertriglyceridemia and hypo-HDL cholesterolemia among Tehranian adolescents between 1999 and 20089). In contrast, a Russian study reported a decreasing trend of dyslipidemia along with decreased prevalence of overweight between 1989 and 20037). A recent study of Japanese adolescents10) reported that increased prevalence of obesity in boys did not affect the lipid profile between 1993 and 2008. Data from a recent large-scale American study5) revealed favourable trends in lipid profile in both boys and girls, despite significant increases in waist circumference and BMI between 1999 and 2008, which is a similar pattern that was observed in this study of Korean adolescents. As the large-scale American study did not include behavioural factors of the participants, it did not investigate possible correlations between behavioural factors and lipid changes. We hypothesized that large-scale epidemiologic studies that include lifestyle factors such as energy intake, physical activity, and alcohol consumption might explain this inconsistency.
Previous studies have shown that high consumption of energy-dense food increases the risk of childhood obesity. Among American children and adolescents, the total energy intake has increased in the 1990s–2000s as compared to the 1970s; consumption of delivery food or eating out has also increased. This trend has coincided with the increased prevalence of obesity14). However, in our study, no changes in daily energy intake were observed, even though the prevalence of overweight and obesity increased significantly during the study period. Only a marginal increase in fat intake was observed in both genders. Similarly, several studies have failed to report the relationship between energy dense food and childhood obesity, as obese children often underestimate their food intake or attempt to reduce their energy intake to lose weight15). In addition, the single 24-hour food recall that we used to assess dietary intake in this study limits the extrapolation of long-term eating habits. Due to this inconsistency, our results did not show any particular effects of diet on blood lipids. Prospective studies on the relationships between dietary patterns with childhood obesity and lipid profile are needed.
Breakfast is an important meal, as it breaks the overnight fasting period and ensures the supply of glucose and other essential nutrients to the body. Eating a fibre-rich breakfast reduces between-meal hypoglycaemia and reduces appetite and energy intake through the release of gut hormones that act as satiety factors. As a result, skipping breakfast has been reported to be associated with a higher fat and energy intake, resulting in weight gain in children and adolescents16). Despite growing concerns over the importance of breakfast, few studies have evaluated the prevalence of breakfast skipping in the paediatric population using nationwide survey data. Recent studies in adolescents have reported that breakfast skipping is highly prevalent in the United Kingdom17) (30%–43%), the US18) (31%–36%), whereas breakfast skipping is relatively rare in Japan19) (10%–15%). We found that the prevalence of breakfast skipping in Korean adolescents was 37%–42% in 1998, but that the prevalence of breakfast skipping significantly decreased to 18%–20% in 2010. This downward trend is likely in part due to the 'eat breakfast campaign'. In Korea, several attempts have been made to reduce breakfast skipping in school children and include media promotions to spread awareness about the high prevalence of breakfast skipping in children, educational programs for students and parents teaching the importance of eating breakfast, and implementation of "School Breakfast Programs" that provide breakfast skipping students with food at school.
Evidence that skipping breakfast may affect lipid profile in adult populations is emerging in Western countries. In a longitudinal study in Australia, adults who skipped breakfast in both childhood (age, 9–15 years) and adulthood (age, 26– 36 years) had higher total cholesterol and LDL-cholesterol levels than those who ate breakfast at both time points20). A recent large-scale population study in the US also demonstrated the increased risk of dyslipidemia among adults who skipped breakfast21). The main factors that explain the association between breakfast skipping and dyslipidemia appears to be increased appetite and subsequent high-energy intake after fasting. In addition, insulin resistance induced by breakfast skipping may play an important role in dyslipidemia. First, hyperinsulinaemia could increase apolipoprotein B-48 secretion, stimulating the formation of chylomicrons in the small intestine and inducing postprandial hyperlipidaemia21). Second, hyperinsulinaemia decreases clearance of triglycerides through the inhibition of lipoprotein lipase activity, which hydrolyses the core triglycerides of chylomicrons22). Third, hepatic lipase activity, which hydrolyses triglycerides and phospholipids of intermediate density lipoprotein, LDL, and HDL, is increased in insulin-resistant status. Increased hepatic lipase activity leads to decreased HDL-cholesterol and increased artherogenic small, dense LDL particles23). Evidence on the unfavourable effects of skipping breakfast on the blood lipid profile of adolescents is scarce, particularly in Asia. To date, only one study has demonstrated that the frequency of breakfast eating is negatively associated with triglycerides and very LDL cholesterol in Brazilian obese children and adolescents24). In this study, we demonstrated that breakfast skipping increases the risk of hyper-LDL-cholesterolemia in boys and the risk of hypertriglyceridemia in girls, after adjusting for obesity level and dietary energy intake. The decreased prevalence of breakfast skipping could partly explain the trends of LDL-cholesterol and triglycerides and obesity prevalence observed in this study.
Many studies report that physical activity has beneficial effects on the lipid profile of adults. While few studies have suggested that regular exercise can reduce LDL-cholesterol25), most have not found a significant relationship between physical activity and LDL-cholesterol2627). Nutrient intake, exercise intensity, and exercise induced weight loss may have been confounding factors in these studies. A few studies that have controlled for these confounding factors suggested that the exercise training is beneficial for reducing the cardiovascular risk, as it increases the LDL particle size and reduces the number of artherogenic small LDL particles, without affecting the total LDL-cholesterol level2627). Most studies agree that exercise training decreases triglyceride and increases HDL-cholesterol levels in overweight and normal-weight adults252627). The results of our study, which showed favourable or constant trends in lipid profile and increasing trends in regular exercise levels, agree with previously published studies.
The effects of alcohol on LDL-cholesterol appear to vary by types and patterns of alcohol intake, population, and sex. Alcohol consumption was associated with decreased LDL-cholesterol levels in Chinese28) and Japanese29) studies. In contrast, recent studies of Italians30) and Turks31) reported that alcohol intake increased LDL-cholesterol concentrations. A relationship between alcohol consumption and HDL-cholesterol also has been suggested, although the underlying mechanism has yet to be determined. Small and moderate levels of alcohol consumption increase HDL-cholesterol levels32), but heavy drinking does not appear to be related to increased HDL-cholesterol levels33). The relationship between alcohol intake and triglyceride levels appears to vary by race and sex. A multiethnic study in the US reported that alcohol consumption was associated with increased triglyceride concentration only in African-Americans34). A separate study noted that alcohol intake increased triglyceride concentration in men, but decreased the concentration in women32). In this study, the prevalence of alcohol consumption among Korean adolescents decreased marginally; however, alcohol consumption was not associated with the risk of dyslipidemia. Further research is required to establish the effect of alcohol consumption on lipid metabolism.
It is noteworthy that breakfast skipping and regular exercise, important determinants of lipid profile, were significantly associated with socio-economic status in the present study (data not shown). For instance, breakfast skipping rates were significantly higher in subjects in the lowest household income quartile than those in the highest quartile. In contrary, regular exercise rates were lower in subjects in the lowest household income quartile than those in the highest quartile. Therefore, lifestyle modifications to prevent adverse lipid metabolism should be emphasized particularly in children and adolescents in low socio-economic status.
There are some limitations to this study. First, while LDL-cholesterol levels were directly measured in 1998, they were calculated with Friedewald formula in 2010, therefore there is some possibility of underestimation of LDL-cholesterol levels in 2010. A recent study among Korean adults demonstrated that the Friedewald formula has shown to underestimate LDL-cholesterol levels when triglyceride levels are greater than 298 mg/dL, and it accurately estimates directly-measured LDL-cholesterol levels when triglyceride levels are between 36 and 298 mg/dL35). In this study, there was no significant differences in the prevalence of hypertriglyceridemia greater than 298 mg (data not shown) between 1998 and 2010 in both genders. Therefore, we think that the methodological difference in estimation of the concentrations of LDL-cholesterol may not significantly influence the results of this study. Second, the study was cross-sectional; therefore, causality cannot be inferred. Third, sexual maturation was not analysed in the KNHANES; therefore, we could not assess or adjust for the effects of puberty. Fourth, we did not assess dietary patterns, such as consumption of high calorie foods or vegetables, which could influence the lipid profile. Nonetheless, this is the first study to examine trends in the lipid profile and the risk of dyslipidemia among Korean adolescents using the most recent, nationally representative data.
In conclusion, favourable or constant trends of LDL-cholesterol levels in boys and triglyceride levels in girls were observed, despite the increased prevalence of obesity in boys. Improvements in the prevention of breakfast skipping and in the levels of regular exercise may contribute to favourable trends observed in the lipid profile of adolescents. We suggest that policies, surveys, and education aimed at improving childhood health and preventing cardiovascular disease in adulthood need to focus on both nutrition and exercise for the greatest impact.
Acknowledgments
We thank the Korea Centers for Disease Control and Prevention for providing the data.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.