Evaluation of new American Academy of Pediatrics guideline for febrile urinary tract infection
Article information
Abstract
Purpose
To evaluate the practical applications of the diagnosis algorithms recommended by the American Academy of Pediatrics urinary tract infection (UTI) guideline.
Methods
We retrospectively reviewed the medical records of febrile UTI patients aged between 2 and 24 months. The patients were divided into 3 groups: group I (patients with positive urine culture and urinalysis findings), group II (those with positive urine culture but negative urinalysis findings), and group III (those with negative urine culture but positive urinalysis findings). Clinical, laboratory, and imaging results were analyzed and compared between the groups.
Results
A total of 300 children were enrolled. The serum C-reactive protein level was lower in children in group II than in those in groups I and III (P<0.05). Children in group I showed a higher frequency of hydronephrosis than those in groups II and III (P<0.05). However, the frequencies of acute pyelonephritis (APN), vesicoureteral reflux (VUR), renal scar, and UTI recurrence were not different between the groups. In group I, recurrence of UTI and presence of APN were associated with the incidence of VUR (recurrence vs. no recurrence: 40% vs.11.4%; APN vs. no APN: 23.3% vs. 9.2%; P<0.05). The incidence of VUR and APN was not related to the presence of hydronephrosis.
Conclusion
UTI in febrile children cannot be ruled out solely on the basis of positive urinalysis or urine culture findings. Recurrence of UTI and presence of APN may be reasonable indicators of the presence of VUR.
Introduction
Urinary tract infection (UTI) is a common bacterial disease in children. Early diagnosis and prompt treatment of UTI in febrile children is important for preventing potential renal insufficiency1). Several imaging studies for urinary tract malformation and renal damage have been recommended in children diagnosed with UTIs234). However, this trend has changed to downgrading the study levels in relation to the patient's age and severity of clinical symptoms3). Recently, the American Academy of Pediatrics (AAP) established the practice guideline for febrile UTI patients aged between 2 and 24 months. According to the guideline, findings of pyuria or bacteriuria on urine analysis and a positive urine culture showing pure bacterial growth higher than 50,000/CFUs (colony forming units) are sufficient for confirming the diagnosis of UTI. With regard to imaging studies, it has been proposed that the renal-bladder ultrasonography (RBUS) be performed in all patients and voiding cystourethrography (VCUG), in specific cases only. The criteria for performing the VCUG study are (1) abnormal results on the RBUS, (2) recurrent infection, and (3) atypical clinical course4). In this study, we aimed to evaluate the practical application of the diagnosis algorithms of the new AAP UTI guideline and compared it with that of our protocol.
Materials and methods
1. Patients
We retrospectively reviewed the medical records of children aged between 2 and 24 months, who were admitted to our institution for their first febrile UTI from January 2010 to December 2012. According to our protocol, all tests (RBUS, technetium-99m-labeled dimercaptosuccinic acid [DMSA] scanning and VCUG) are performed in the patients aged between 2 and 24 months with positive findings on urinalysis or urine culture or both, who have fever without clear cause. Febrile patients with a temperature above 37.8℃ and positive findings on urinalysis or urine culture or both were included in the study. We excluded patients who had symptoms or signs implicating other infection source to rule out asymptomatic bacteriuria accompanied with other infections. We set the criteria for positive urinalysis as pyuria (≥5 white blood cells [WBCs]/high power field) or a finding of more than 1+ of nitrite5). A positive urine culture was defined as pure growth of >104 organisms/mL on a catheter or suprapubic urine specimen1). RBUS and DMSA scanning for renal scars were performed within a week from the first day of admission. The patients with urologic abnormalities were excluded, except those with vesicoureteral reflux (VUR). VCUG was performed within 1 month of onset of UTI. Abnormal RBUS result was defined as hydronephrosis according to the Society for Fetal Urology classification6), and acute pyelonephritis (APN) was confirmed when the DMSA scan showed a focal or multifocal parenchymal defect or a diffuse decrease or absence of uptake7). For patients with APN, DMSA scanning was conducted between 4 and 6 months after the primary encounter at which a UTI was diagnosed, to check for the presence of renal scars. Renal scar was defined as a cortical defect that remained for more than 6 months. VUR was classified from grade I to V according to the international system of radiographic grading of VUR8). The recurrence of UTI was also defined according to the same criteria stated above including voided urine culture for clinically UTI suspected patients. All patients with UTI were followed up for at least more than 6 months. We obtained institutional board permission to review the electronic medical records of children.
2. Comparison of clinical findings according to diagnostic criteria
To evaluate the accuracy of a diagnosis of UTI according to the 2011 AAP guideline4), we categorized all patients into 3 groups: group I (patients with positive urine culture and urinalysis findings), group II (patients with positive urine culture but negative urinalysis findings), and group III (patients with negative urine culture but positive urinalysis findings). We included patients who had fever but not other symptoms or signs implicating other infection among the members of groups II and III to exclude asymptomatic bacteriuria or sterile pyuria. Clinical and laboratory findings, namely age; sex; serum C-reactive protein (CRP) level and WBC count; rates of hydronephrosis, APN, VUR, and renal scar; and recurrence of UTI were compared among the groups.
3. Imaging study in group I
To assess the accuracy of the inclusion criteria for VCUG according to the 2011 AAP guideline4), patients in group I (children with UTIs according to the AAP guideline) were subdivided into 2 subgroups according to the presence or absence of hydronephrosis or the recurrence of UTI. The subgroups were compared on the basis of their serum CRP levels, WBC count, and the rates of VUR, APN, and renal scar. We also evaluated the detection rate for VUR and the recurrence of UTI between patients with and without APN on the DMSA renal scans. Because the abnormal clinical course for UTI is not clearly described in the AAP guideline, we did not analyze this aspect.
4. Statistics
The Kruskal-Wallis and Mann-Whitney tests were performed to compare continuous variables, such as age and serum CRP level and WBC count, among the groups. The Fisher exact test or Pearson chi-square test was performed to compare categorical variables including sex, hydronephrosis, APN, VUR, renal scar, and recurrence of UTI among the groups. To adjust for age and sex, multivariate analyses were performed using both the logistic regression model and covariance analysis. Calculations were performed using the IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). Data were presented as median (interquartile range) for continuous variables and proportions for categorical variables. A P value <0.05 was considered statistically significant.
Results
1. Patient characteristics
The medical records of a total of 328 patients diagnosed with febrile UTI were initially reviewed during the study period. Among them, 28 patients were excluded because of insufficient medical information, type of urine collection method, and congenital urologic anomalies. Therefore, the remaining 300 patients with febrile UTI were enrolled in the present study. The median age was 4 months, and 66.3% of the patients were male. The results of imaging studies were as follows: hydronephrosis was observed in 50% of the patients (145 of 290); APN, in 29.4% (85 of 289); VUR, in 13.2% (31 of 234); and renal scar, in 22.5% (9 of 40). Of the children with VUR, 38.7% had high-grade VUR (grades IV and V). Twenty-two children (7.3%) had recurrence of UTI. Monitoring for recurrence was performed from 6 to 42 months. The mean follow-up period was 23.7 months.
2. Comparison of the clinical findings according to diagnostic criteria
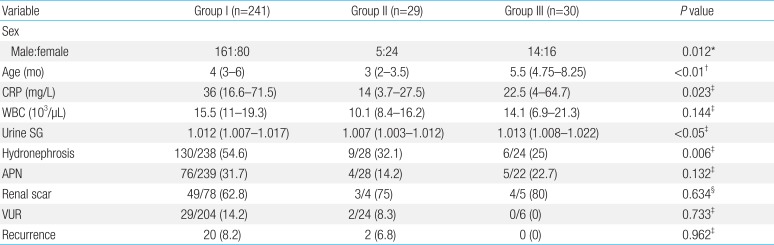
With regard to the study groups, 241 patients were included in group I; 29, in group II; and 30, in group III. The median age was lower and the proportion of boys was higher in group II than in groups I and III (P<0.05). Multivariate analysis adjusted for age and sex showed that the serum CRP level and urine specific gravity (SG) was the lowest in group II (P<0.05); however, it was not different between groups I and III. The leukocyte count was similar among the groups. In addition, group I had a higher rate of hydronephrosis than groups II and III, and there was no difference in the frequency of hydronephrosis between groups II and III (group I vs. II vs. III, 54.6% vs. 32.1% vs. 25%; I vs. II & III, P<0.05). The frequencies of APN, VUR, renal scar, and UTI recurrence were not different among the groups after adjusting for age and sex (Table 1).

Clinical and laboratory data of the study groups
3. Comparison of data between patients with and without hydronephrosis
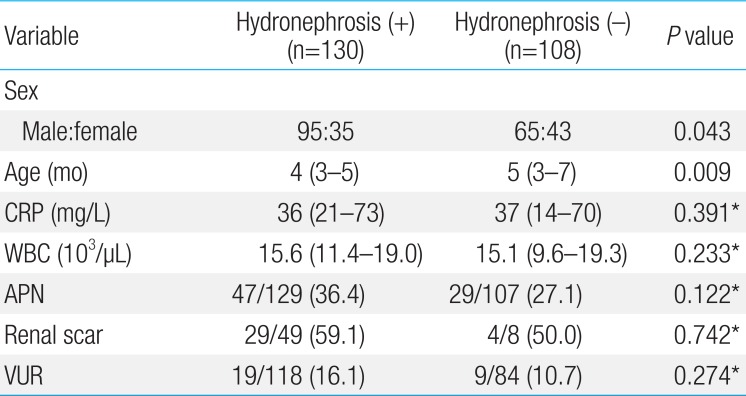
We subdivided group I into 2 subgroups on the basis of the presence (n=130) or absence of hydronephrosis (n=108). Three patients in group I who did not undergo the RBUS were excluded. In the multivariate analysis adjusted for age and sex, there were no differences in the serum levels of CRP and WBCs and frequency of APN, VUR, and renal scar between the 2 subgroups. The detection rate for VUR was only 16% in UTI patients with hydronephrosis, while 11% of the UTI patients without hydronephrosis had VUR; 32% of the patients with VUR (9 of 28) had normal RBUS findings (Table 2).

Comparison of data between patients with and without hydronephrosis in group I
4. Comparison of data between patients with and without the recurrence of UTIs
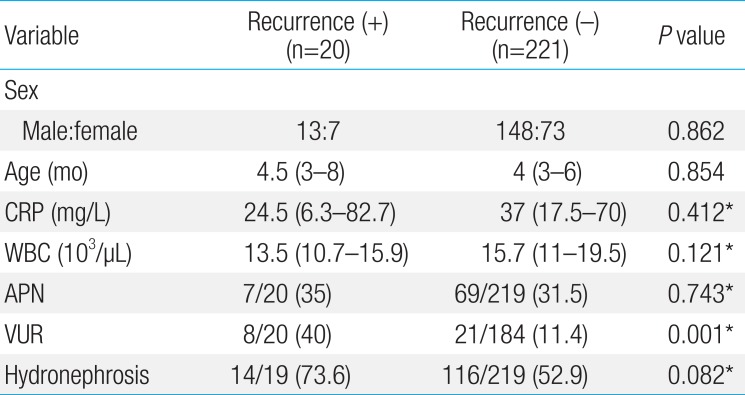
When we subdivided group I into 2 subgroups on the basis of the presence (n=20) or absence of recurrence of UTI (n=221), the rate of VUR was found to be higher in children with recurrence than in those without recurrence, after adjusting for age and sex (40% vs. 11.4%, P<0.05). The multivariate analysis adjusted for age and sex showed that the level of serum CRP and WBCs and the frequencies of hydronephrosis and APN were not different between the 2 subgroups (Table 3).

Comparison of data between patients with and without urinary tract infection recurrence in group I
5. Comparison of data between patients with and without APN
When we subdivided group I into 2 subgroups on the basis of the presence (n=73) or absence of APN (n=130), multivariate analysis adjusted for age and sex revealed that the rate of VUR was higher in the group with APN than in the group without APN (23.3% vs. 9.2%, P<0.05). The recurrence rate was not different between the patients with and without APN (9.2% vs. 8.0%).
Discussion
The major finding of our study is that positive findings on either urine culture or urinalysis could be as important as positive findings on both the tests for the diagnosis of UTI in febrile children. Laboratory findings, except serum CRP level, were similar among the groups, and the findings of imaging studies, except the presence of hydronephrosis, and recurrence rate for UTI were similar among the 3 groups. Additionally, the finding of hydronephrosis was not related to the incidence of VUR, and the recurrence of UTIs and presence of APN on the DMSA scan were associated with the incidence of VUR.
The incidence of UTI was 3%-5% in girls and 1% in boys1). UTI is difficult to diagnose in infancy, since the symptoms are usually not specific, such as fever. Therefore, several evidence-based guidelines have been established for UTI control39). Regarding a diagnosis, our national guideline recommends the evidence of positive urine culture results instead of positive urine analysis findings3). The AAP's diagnostic criteria is based on the proof of infection on both urinalysis and urine culture4). In the present study, we found that UTI could not be ruled out in cases of positive findings on either urinalysis or urine culture in cases of febrile children. While the serum level of CRP in children with only positive urine culture was lower than that in the children from the other 2 groups, it was not different between patients with positive findings on both tests and those with positive urinalysis findings only. The serum WBC count was also not different among the 3 groups. More importantly, the frequency of APN, VUR, renal scar, and UTI recurrence was similar among the groups. Although the rate of hydronephrosis was higher in children with positive results on both urine culture and urinalysis than that in children with positive findings on only one test, it was not related with the severity of other clinical and radiologic findings.
The diagnosis of UTI involves numerous important considerations. The presence of pyuria indicates the presence of infection, but infection can occur in the absence of pyuria. Pyuria might be also absent in the case of urine dilution10). Our results show a lower level of urine SG in patients with only positive urine culture findings than in other two groups even though the mean level of that were within normal range. In addition, false-negative WBC count might be obtained in case of lysis or the absence of inflammatory response in colonized (rather than infected) individuals11). Urine culture findings are the reference standard for the diagnosis of UTI, but negative culture findings are often observed in various clinical settings; partially treated bacterial UTIs, viral infections and UTI in the presence of urinary obstruction1). Although serum levels of CRP and WBCs can help in the diagnosis of UTI, they may be not pathognomonic of UTI. The data regarding their roles on the prediction of renal scar as well as acute positive scintigraphy findings are also conflicting1213). In this study, positive urinalysis findings might be related more with increased serum CRP levels than with urine culture findings of febrile children with UTI because the serum CRP level was lower in patients with only positive urine culture findings than in children with only positive urinalysis findings. This observation is in line with our previous findings that showed a positive linear correlation between the number of WBCs in the urine sample and serum level of CRP in febrile patients with UTI14). Considering that the serum level of leukocytes was similar among the 3 groups, we cannot clearly confirm which group had severe infection. Likewise, in symptomatic infants and children treated for the first episode of UTI, clinical and laboratory findings and the prevalence of pyelonephritis, reflux, and urological malformations were not different between those with high or low bacterial-count UTIs1516). Levtchenko et al.17) stated that 9% of 166 patients had negative or equivocal urine culture findings despite clinical and scintigraphic evidence of APN and, notably, among them, 60% had VUR. Another study on children diagnosed with APN on the basis of DMSA scan findings and negative urine culture findings showed that 65.4% of the patients had VUR18). In the present study, the frequencies of APN, VUR, renal scar, and recurrence of UTI were similar among the groups, although children with positive findings on both tests showed a higher frequency of hydronephrosis. However, hydronephrosis was not related with other clinical, laboratory, and radiologic findings. Other reports have shown that hydronephrosis is not associated with renal scar formation, severity of the inflammatory process, or volume of kidney injured1920). The management of UTI is also not usually altered by the identification of hydronephrosis21). This means that, despite the difference in the frequency of hydronephrosis, in the presence of a positive finding on only 1 of the 2 tests, i.e., urine culture or urinalysis, the possibility of UTI cannot be excluded.
According to the AAP UTI guideline, VCUG is not recommended routinely after the first UTI. VCUG is indicated in one of the following 3 scenarios: (1) abnormal RBUS results, (2) recurrence of febrile UTI, or (3) abnormal clinical course. Abnormal RBUS finding is defined as hydronephrosis, scarring, or other findings that suggest either high-grade VUR or obstructive uropathy4). We defined abnormal RBUS as the presence of hydronephrosis in this study and found no association between the presence of hydronephrosis and VUR. The detection rate of VUR was only 16% in children with UTI and hydronephrosis; of note, 84% of the patients with hydronephrosis showed normal VCUG findings. Further, 11% of the children without hydronephrosis had VUR and 31% of the patients with VUR showed normal RBUS findings. Owing to these findings, RBUS was not regarded an appropriate test for ruling out VUR. Blane et al.22) showed that of the kidneys with VUR, 74% showed normal sonographic findings, and 28% of the missed refluxing kidneys had grade III or higher reflux. Therefore, it may be not reasonable to set the standard of VCUG trials in reference to the presence of hydronephrosis. In addition, hydronephrosis was not predictive of APN on the DMSA scan, consistent with other studies2324).
With regard to the recurrence of febrile UTI, a significant association was observed between the presence of VUR and UTI recurrence in this study. In line with our findings, a study involving 307 UTI patients showed that the recurrence was related to reflux25). Another study involving children aged <6 years showed a correlation between UTI recurrence and VUR grades 4 and 526). However, the reasons behind the relationship were not fully explained. Because a UTI occurs when urothelial cell receptors allow bacterial attachment, VUR alone might not affect UTI occurrence27). However, it is also plausible that VUR itself can predispose an individual to renal infection by raising the level of residual urine and facilitating the transport of bacteria from the bladder to the upper urinary tract28). In this study, the recurrence of febrile UTI was not associated with other laboratory and radiologic findings, although the frequency of hydronephrosis tended to be higher in children who experienced recurrence than in those who did not.
Notably, VUR was more frequently found in patients with APN on the DMSA renal scan than in those without APN. Further, 23% of the children with APN had VUR, similar to the findings in other reports2930). The AAP does not recommend DMSA scanning as part of routine evaluation of infants with their first febrile UTI because the findings on nuclear scans rarely affect acute clinical management and the radiation dose from DMSA scanning is additive to that of VCUG when both imaging studies are performed4). Some researchers also recommend performing the DMSA scanning not during the acute phase but 6 to 12 months after an acute infection to detect renal scarring, which would require follow-up1931). However, considering our results, ultrasonography alone may not be a selective method for identifying patients at risk of VUR. DMSA renal scan performed during the acute stage of a UTI, followed by VCUG if the scintigraphy suggests pyelonephritis, may reduce the number of cystourethrographies required2132). Performing the VCUG 3-6 weeks after the diagnosis of UTI, as done conventionally, might also be helpful in decreasing unnecessary exposure to ionizing radiation.
Our study has some limitations. First, positive urine culture was defined as the presence of any bacterium at a level higher than 10,000 CFUs/mL, but below 50,000 CFUs/mL, as indicated by the AAP guideline. However, a child was considered as having a UTI if there were 10,000 colonies of a single bacterium and the child was symptomatic1). Secondly, positive urinalysis result was determined according to the presence of pyuria or nitrite; however, it did not include the findings of leukocyte esterase or bacteria on microscopic analysis which mentioned by the AAP guideline. Thirdly, abnormal RBUS result was defined as the presence of hydronephrosis only. Because the sonographic findings could have shown wide variations according to the investigators, we tried to objectively measure the results, as per the Society for Fetal Urology classification6). Finally, this study involved a retrospective review of the patients from 1 hospital, and the number of subjects was relatively small to comparatively analyze several parameters.
In conclusion, our findings imply that positive findings on either urinalysis or urine culture are important in the diagnosis of febrile UTI in children aged from 2 to 24 months. Clinicians should make an interpretation of the results of urine test attentively considering several causes of false-negative urinalysis or urine culture in cases with clinically suspected UTI. Hydronephrosis may not be a good indicator of the presence of VUR, but the recurrence of UTI and APN on the DMSA scan can be associated with the presence of VUR in febrile young children. DMSA renal scan may be a better method than ultrasonography for identifying patients at risk of VUR. Therefore, it may be time to reevaluate the clinical practices that follow the AAP UTI Guideline. Further studies involving a large population are required to confirm the potential application of our findings for diagnosing and managing febrile UTI in children.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.