Reference values for respiratory system impedance using impulse oscillometry in healthy preschool children
Article information
Abstract
Purpose
The normal values for lung resistance and lung capacity of children, as determined by impulse oscillometry (IOS), are different for children of different ethnicities. However, reference values there is no available reference value for Korean preschool children have yet to be determined. The aim of the present study was to determine the normal ranges of IOS parameters in Korean preschool children.
Methods
A total of 133 healthy Korean preschool children were selected from 639 children (aged 3 to 6 years) who attended kindergarten in Seongnam, Gyeonggi province, Korea. Healthy children were defined according to the European Respiratory Society (ERS) criteria. All subjects underwent lung function tests using IOS. The relationships between IOS value (respiratory resistance (Rrs) and reactance (Xrs) at 5 and 10 Hz and resonance frequency (RF)) and age, height, and weight were analyzed by simple linear and multiple linear regression analyses.
Results
The IOS success rate was 89.5%, yielding data on 119 children. Linear regression identified height as the best predictor of Rrs and Xrs. Using stepwise multiple linear regressions based on age, height, and weight, we determined regression equations and coefficients of determination (R2) for boys (Rrs5=1.934-0.009×Height, R2=12.1%; Xrs5=0.774+0.006×Height-0.002×Age, R2=20.2% and for girls (Rrs5=2.201-0.012×Height, R2=18.2%; Xrs5=-0.674+0.004×Height, R2=10.5%).
Conclusion
This study provides reference values for IOS measurements of normal Korean preschool children. These provide a basis for the diagnosis and monitoring of preschool children with a variety of respiratory diseases.
Introduction
Pulmonary function tests (PFTs) are important for the evaluation of respiratory problems in children. In particular, these tests allow measurement of respiratory status by monitoring changes in lung function of children with chronic lung diseases, such as asthma. In addition, PFTs can be used to help to diagnosis children with chronic lung diseases1). For the diagnosis and management of respiratory disease, reference data of healthy children are needed to establish baseline PFT results2).
Spirometric determination of forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) are widely used to evaluate airway obstruction, to diagnose and monitor various respiratory diseases3). However, spirometry is difficult to perform in young children due to their short attention span and limited cooperation3-5). Thus, respiratory resistance obtained by the forced oscillation technique (FOT) is commonly used in young children6, 7). The impulse oscillation system (IOS) is a commercial device used to measure oscillatory resistance at multiple frequencies3). This technique requires little patient cooperation because only tidal volume breaths are required and children as young as 2 years can be readily examined8). Thus, measurement of pulmonary resistance in preschool children can be used to diagnose and manage respiratory diseases6, 9).
IOS is widely used by pediatric caregivers for the diagnosis and management of respiratory and allergic diseases. Like other pulmonary function values, IOS parameters have different normal reference levels from different races and age groups2, 10-12). Several reports have identified normal reference levels in Korean school-aged children13, 14). However, there are no reports on reference values for preschool children, thus making it difficult to diagnose and monitor respiratory diseases in these children using IOS.
The aim of the present study was to determine reference values of IOS measurements for Korean preschool children so that clinicians can more readily diagnose and manage respiratory disease in this group of patients.
Materials and methods
1. Subjects
This was a cross-sectional study of preschool children aged 3-6 yrs. All subjects were attending one of five kindergartens in Seongnam from May to July of 2009. Based on guidelines of the American Thoracic Society (ATS)3) and European Respiratory Society (ERS)15), subjects with the following characteristics were excluded: (i) personal or family history of wheezing or asthma; (ii) personal history of allergic rhinitis or atopic dermatitis; (iii) premature birth, low birth weight, or history of ventilation or bronchopulmonary dysplasia; (vi) exposure to passive smoking in the family; (v) obesity (body mass index >95% of predicted or ≥ 25 kg/m2 16); (vii) recent upper respiratory tract infection; and (viii) severe respiratory disease with dyspnea. This study was approved by the ethics committee of CHA University and written informed consent was obtained from the parents of all participating children.
2. Health screening questionnaire
We collected patient information through a health screening questionnaire administered to the parents of all participating children. The questionnaire was designed to exclude children with asthma, allergic disorders, or a family history of asthma. Our Korean questionnaire17) was developed using an international asthma and allergy questionnaire18). In addition, the survey assessed age, gender, family smoking history, and any other previous respiratory therapies.
3. Impulse oscillation system
Impulse oscillometry was performed using the Master Screen Spirometry-IOS Digital System (Jaeger Company, Würtzburg, Germany). All IOS measurements were performed according to methods described by the European Respiratory Society (ERS)15) by one experienced operator. We measured the resistance at 5 Hz (Rrs5) and 10 Hz (Rrs10), values routinely used to assess pulmonary resistance, and reactance at 5 Hz (Xrs5) and 10 Hz (Xrs10), values that reflect pulmonary compliance.
4. Statistical analysis
Data are expressed as means and standard deviations. The statical data was calculated as means of three values. Within-test repeatability was estimated by the coefficient of repeatability (CR) and the coefficient of variation (CV)19). The CR was calculated as 2.83×within subject SD (2.83×SD) and CV was calculated as SD/mean20). Linear regression analysis was used to assess the relationship between IOS pulmonary function measures and anthropometric data (height, weight, and age). Data were analyzed separately for boys and girls, using multiple linear regressions and the 'stepwise' method to identify the best predictors of respiratory resistance parameters. When the 'stepwise' method is available, 'enter' method is used for the best fitting equation. Data were analyzed using SPSS software (version 17.0, Chicago, IL, USA). The significance level was 0.05 for all comparisons.
Results
1. Characteristics of children
We initially recruited 639 preschool children. The parents of 630 children (98.6%) were screened using the questionnaire. A total of 497 children were excluded based on our exclusion criteria, and 133 healthy children, aged 3-6 years, were enrolled. The success rate of IOS was 89.9%, so our analysis ultimately considered data of 119 children.
Table 1 shows the characteristics of enrolled children stratified by age. A total of 56% of the patients (n=67) were boys, mean age was 4.9±0.86 years, mean height was 109.1±7.11 cm, and mean weight was 18.7±3.34 kg.

Demographic Characteristics of Enrolled Children
2. Relationships of IOS and anthropometric data
Within-test repeatability of Rrs5 indicated that CR was 0.175 and CV was 6.1%. Linear regression analysis of IOS measures indicated that Rrs5 was significantly associated with height, weight, and age. Log-transformation of the IOS values and height did not improve this relationship. In addition, height had the greatest correlation with Rrs5 (r=0.72). Table 2 shows the results of linear regression models for all IOS variables with height.

Regression Equations for All Variables versus Height
3. IOS predictive equations for boys and girls
Table 3 shows the results of multiple linear regression equations for age, height, and weight. Height was the strongest independent variable for all IOS values. Rrs was negatively correlated with height. For boys, Rrs5=(1.934-0.009×height), with a coefficient of determination (R2) of 12.1%. For girls, Rrs5=(2.201-0.012×height), with an R2 of 18.2%. Xrs was also positively correlated with height. For boys, Xrs5=(-0.774+0.006×height-0.002×age), with R2 of 20.2%. For girls, Xrs5=(-0.674+0.004×height), with R2 of 10.5%. Fig. 1 shows a significant negative correlation between Rrs5 values and height for all children.
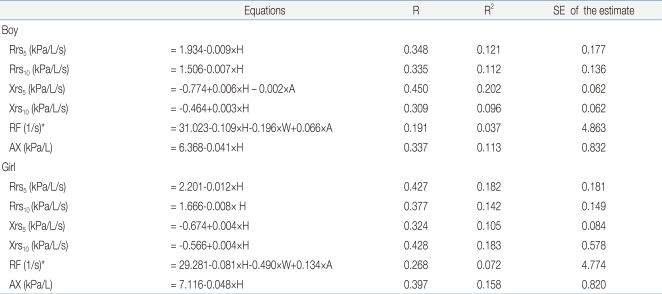
Impulse Oscillation System Predictive Equations for Boys and Girls
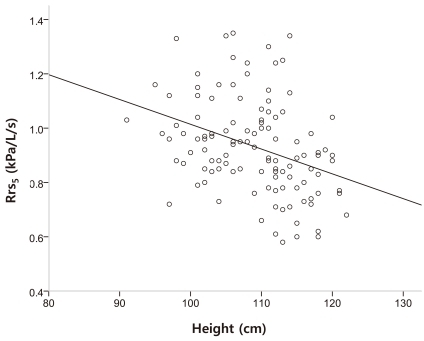
Correlation between height and respiratory resistance at 5 Hz (Rrs5). The regression equation was Rrs5 (kPa/L/s) = 1.934-0.009 × Height (cm); the coefficient of determination was 12.1%.
Discussion
In this study, we determined IOS values for healthy preschool Korean children, in whom spirometry is difficult to perform. We obtained valid IOS measurements for 89.9% of the enrolled children, a higher success rate than reported in previous studies12, 21). This discrepancy may be due to differences in inclusion and exclusion criteria, differences in IOS techniques, and/or our use of one experienced operator for all measurements. The European Respiratory Society (ERS) and the American Thoracic Society (ATS) recommend the selection of a normal population for reference values of respiration measurements, with healthy children selected by a questionnaire that screens for history of asthma and allergies and family history of allergies. Our results indicate that it is relatively easy to perform IOS in healthy children less than 6 years of age.
A description of the normal variability of IOS values is required to define clinically relevant alterations. In this study, we reported within-test variability as CR and CV. Our reported CR and CV values were similar to values reported in previous studies9, 22-24). In addition, our calculations of Rrs, Xrs, Fr, and AX using a regression equation indicated that height was the only significant predictor, also consistent with previous studies12, 23). Similar to previous studies, we found that Rrs was negatively correlated with height and Xrs was positively correlated with height6, 15, 23, 25). Interestingly, our regression coefficients of Rrs with height are strikingly similar to those published by Hellinckx et al.26), Frei et al.6) and Klug et al.24), but different from those published by Ducharme et al.12) and Malberg et al.23). In particular, our study indicated lower resistance values than several previous studies. Table 4 shows the comparison of reference equations of Rrs5 between the present study and previous studies on healthy preschool children. This difference may be caused by differences in age distribution, and/or racial differences. A limitation of our study is that the R2 was less than 20%, which is poorer than that reported in several other previous studies. This may be due to our small number of studied subjects. Comparing to previous school-aged children in Korea, Korean school studies13, 14), our regression equations at multiple frequencies were similar to their reference values, especially about the Rrs5.

Overview of the Regression Equations of Rrs at 5 Hz in Healthy Preschool Children
In line with other studies, we confirmed that IOS is an effective and easily performed noninvasive technique that is well suited for lung function measurements in young children. Reference values for IOS are important for the interpretation of pulmonary function test measures, and are needed for the diagnosis and management of respiratory diseases1). The measurement of respiratory input impedance using IOS has significant clinical value in children with a variety of respiratory disorders27). This study is the first to provide IOS data for healthy Korean preschool children and can be used as a basis for the diagnosis and assessment of prognosis of pulmonary function in children with chronic pulmonary disorders and asthma.
In conclusion, we have determined reference values of IOS measurements generated from a group of healthy Korean preschool children. Our IOS reference values are different from those for preschool children of other ethnic groups, and are essential for the diagnosis and treatment of various respiratory diseases. We suggest that future studies be performed with larger populations of Korean preschool children to confirm our findings.
Acknowledgment
The questionnaire used, the Korean version of ISAAC, was provided by the Korean Academy of Pediatric Allergy and Respiratory Diseases.