Urosepsis and postrenal acute renal failure in a neonate following circumcision with Plastibell device
Article information
Abstract
Plastibell is one of the three most common devices used for neonatal circumcision in the United States, with a complication rate as low as 1.8%. The Plastibell circumcision device is commonly used under local anesthesia for religious circumcision in male neonates, because of cosmetic reasons and ease of use. Occasionally, instead of falling off, the device may get buried under the skin along the shaft of the penis, thereby obstructing the normal flow of urine. Furthermore, the foreskin of neonates is highly vascularized, and hence, hemorrhage and infection are possible when the skin is cut. Necrosis of penile skin, followed by urethral obstruction and renal failure, is a serious surgical mishap requiring immediate corrective surgery and medical attention. We report a case of fulminant urosepsis, acute renal failure, and pyelonephritis in a 4-day-old male neonate secondary to impaction of a Plastibell circumcision device. Immediate medical management was initiated with fluid resuscitation and mechanical ventilation; thereby correcting life threatening complications. Pediatricians and Emergency Department physicians should be cognizant of the complications from Plastibell circumcision device in order to institute appropriate and timely management in neonates.
Introduction
Plastibell device is widely used in neonates and infants as it is easy to use and circumcision can be safely performed even by trained nurses and in developing countries with low complication rates. Plastibell device is a clear plastic ring with a deep groove running circumferentially designed for circumcising male neonates. The Plastibell is placed onto the head of the penis during a short surgical procedure. This procedure can be performed by an experienced physician using adequate anesthesia and appropriate size Plastibell device (Fig. 1). The device functions with the principle of severing blood supply to part of foreskin tissue which dies and sloughs off by itself about 3-7 days after circumcision. The major advantage with its use lies in the quickness of the procedure, and easy monitoring of the child. However, acute renal failure has been reported after circumcision in neonates and infants who had ritual or surgical excision of the foreskin1,2). We report for the first time to our knowledge a case of fulminant urosepsis and postrenal acute renal failure in a neonate after circumcision using Plastibell.

Photograph of the Plastibell circumcision device, in two different sizes.
Case report
A 4-day-old male neonate presented to our Emergency Department (ED) with two days history of irritability, progressive abdominal distention, decreased urine output, and decreased oral intake. Patient did not have fever, congestion, cough, vomiting, diarrhea, or rash. Patient was delivered at term gestational age (birth weight, 2.670 kg) and did not have any complications after birth. He was circumcised on the second day of life with Plastibell device (Hollister, Libertyville, IL, USA) and discharged to home. On presentation to the ED, patient's weight was 2.83 kg, rectal temperature 37.83℃, heart rate 162 beats/min, respiratory rate 88 breaths/min, and pulse oximetry 97% on room air. He had a weak cry, scleral and cutaneous icterus, and marked abdominal distention with bilateral palpable renal masses. The Plastibell device was adherent to a very edematous glans penis with visible membrane occlusion of the urethra, and the penile skin above the device was necrotic. Complete blood count revealed white blood cell count of 2,700/µL with 33% segmented neutrophils, 1% bands, 39% lymphocytes, 19% monocytes, and 7% eosinophils. His hemoglobin was 16.7 g/dL, and platelet count was 44,000/µL. His sodium was 117 mmol/L, potassium 7.7 mmol/L, chloride 86 mmol/L, bicarbonate 16 mmol/L, blood urea nitrogen 19 mg/dL, creatinine 1.71 mg/dL, glucose 64 mg/dL, total bilirubin 11 mg/dL, and direct bilirubin 2 mg/dL. His urine analysis revealed specific gravity 1.008 with 3+ leukocyte esterase, red blood cells 118 per high power field (HPF), and WBCs 195/HPF. Blood, urine, and cerebrospinal fluid cultures were done.
Ultrasound of the abdomen showed bilateral hydronephrosis with the right kidney measuring 5.6 cm×3.1 cm×2.9 cm, and the left kidney measuring 5.8 cm×3.5 cm×3.2 cm and urinary bladder was distended to 60 mL with multiple foci of increased echogenicity consistent with bladder obstruction (Figs. 2, 3). Penile block was performed using 1% lidocaine and the Plastibell device was removed. Urinary catheterization was done and urine was purulent. After immediate output of 80 mL, patient remained polyuric with urine output as high as 19.5 mL/kg/hr. Patient received a fluid bolus of 20 mL/kg of normal saline, 2 mEq/kg of sodium bicarbonate, and urine output replacements with fluid containing 77 mEq of sodium as sodium bicarbonate initially and then sodium chloride after correction of acidosis. Patient was started on ampicillin and cefotaxime. Patient had significant respiratory distress and became bradypneic and hence was intubated and placed on mechanical ventilation. Blood and urine cultures grew Escherichia coli within 24 hours of sampling. Patient remained thrombocytopenic and was transfused with platelets when the count decreased to 15,000/µL. His hemoglobin decreased to 7.4 g/dL after hydration and blood loss following central venous line and arterial line catheterization. He received packed red blood cell transfusion. Patient was extubated on the third day of hospitalization and at this time urine output decreased to 3 mL/kg/hr and creatinine was 0.38 mg/dL. On the seventh day of hospitalization, patient was febrile and grew E. coli from the blood again after a previous negative blood culture. The glans penis by this time appeared well healed. Renal ultrasound at this time showed a slight decrease in the size of the kidneys, with the right kidney measuring 4.5 cm×2.7 cm×2.3 cm, and the left kidney measuring 5.0 cm×2.1 cm×1.9 cm. Increased echogenicity was noted in the upper pole of the right kidney, and there was echogenic nonshadowing debris in the collecting system of the left kidney with increased collecting system dilatation since the previous examination. These findings possibly represented pyelonephritis, and papillary necrosis. Based on sensitivities of the E. coli, cefotaxime was continued and gentamicin was added. Ampicillin was discontinued and patient remained afebrile for the remainder of hospitalization. Voiding cystourethrogram did not show vesicouretral reflux or obstruction. He was discharged 11 days after hospitalization and was on cephalexin for one week following discharge. Patient was noted to be thriving well without any complications on follow-up examinations.

Ultrasound image of the urinary bladder. The urinary bladder (between crosshairs) was distended to 60 mL, which was the estimated maximal capacity for a neonate, and which contained multiple foci of increased echogenicity (white arrows) representing retained debris, findings consistent with obstruction.
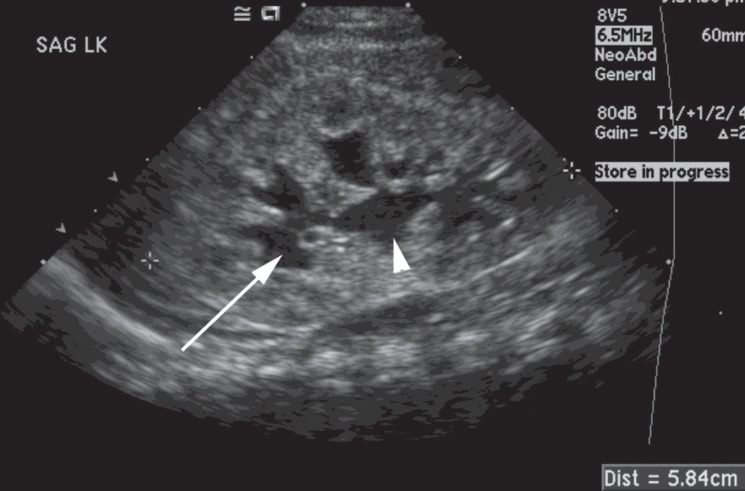
Ultrasound image of the left kidney. Bilateral hydronephrosis (representative left kidney shown) with dilatation of the renal calyces (white arrow) and renal pelvis (white arrowhead) with increased renal size was observed. Findings were consistent with obstruction.
Discussion
We report for the first time to our knowledge a case of a neonate with fulminant urosepsis, acute renal failure and pyelonephritis following circumcision with a Plastibell device. The ring was impacted and caused the glans to become extremely edematous, leading to almost complete obstruction of the urethra.
Circumcision is believed to be the oldest planned operation and may have originated in Egypt more than 6,000 years ago3). While there is scientific evidence demonstrating potential medical benefits of male circumcision in the newborn period, the American Academy of Pediatrics determined that there is not sufficient data to recommend routine neonatal circumcision4). When the decision to circumcise has been made, the procedure can be done by surgical excision or with devices such as the Plastibell device, Gomco clamp, or Mogen clamp5).
Plastibell device was invented by Hollister Inc. in 1950 and has been reported to be in use since 1953. Plastibell is used in nearly 60% of all routine circumcisions in the United States. The device is a clear plastic ring with a handle. It comes in 6 different sizes, 1.1-1.7 cm and the size to be used is correlated to the size of the glans penis. An appropriate size bell which snugly fits 2/3 of the glans should be used along with the thread that is tight enough to cause ischemia of the foreskin. Smaller bell sizes will result in tissue necrosis and larger bell can migrate and get impacted. After adequate analgesia, the foreskin is cut longitudinally and the glans is exposed. Appropriate size device is placed over the glans, the foreskin is pulled over the ring and a ligature is tied around the foreskin. The bell of the device is removed and the end ring will fall off within 3-7 days. The ring may separate earlier in neonates because of the thin prepuce and easier sloughing6).
Complication rates for Plastibell device ranging from as low as 1.8% to as high as 20% have been reported by various investigators7,8). Complications are lower in neonates compared to infants and older children. Impaction of the device as seen in our patient has been reported as the most frequent complication in a large study with a rate of 2.3% in patients less than 3 months of age and 26.9% in those greater than 5 years of age6). Bleeding and infection have been reported as the most common complications by various authors1,7). Other rare but serious complications reported includes necrotizing fasciitis, retention of urine secondary to glandular prolapse, acute venous stasis secondary to distended bladder causing vena caval obstruction and acute urinary obstruction with ruptured bladder2,9,10,11,12).
Acute renal failure has been reported after circumcision in neonates and infants performed in the community and application of tight dressing on the penis13,14). These patients had ritual or surgical excision of the foreskin and was not related to a device as seen in our patient. E. coli sepsis has been reported in a patient after ritual circumcision secondary to urinary obstruction15). We did not find any report in the literature of fulminant sepsis and acute renal failure in a neonate after circumcision using Plastibell.
Our patient developed urethral obstruction and subsequently hydronephrosis, acute renal failure, fulminant E.coli sepsis with disseminated intravascular coagulation and respiratory failure that required mechanical ventilation and aggressive fluid resuscitation in less than 48 hours from impaction of the Plastibell device. Furthermore, the acute and rapid onset of urosepsis led to pyelonephritis in our patient. Such complications could be fatal in a 4 day old neonate.
Pediatricians and ED physicians should be cognizant of such life threatening complications from Plastibell device in order to institute appropriate and timely management in neonates who might undergo circumcision with Plastibell device.
Acknowledgment
Authors would like to thank GP Supplies Limited, UK for providing plastibell device image for publication.
Notes
No potential conflict of interest relevant to this article was reported.