p-Cresyl sulfate and indoxyl sulfate in pediatric patients on chronic dialysis
Article information
Abstract
Purpose
Indoxyl sulfate and p-cresyl sulfate are important protein-bound uremic retention solutes whose levels can be partially reduced by renal replacement therapy. These solutes originate from intestinal bacterial protein fermentation and are associated with cardiovascular outcomes and chronic kidney disease progression. The aims of this study were to investigate the levels of indoxyl sulfate and p-cresyl sulfate as well as the effect of probiotics on reducing the levels of uremic toxins in pediatric patients on dialysis.
Methods
We enrolled 20 pediatric patients undergoing chronic dialysis; 16 patients completed the study. The patients underwent a 12-week regimen of VSL#3, a high-concentration probiotic preparation, and the serum levels of indoxyl sulfate and p-cresyl sulfate were measured before treatment and at 4, 8, and 12 weeks after the regimen by using fluorescence liquid chromatography. To assess the normal range of indoxyl sulfate and p-cresyl sulfate we enrolled the 16 children with normal glomerular filtration rate who had visited an outpatient clinic for asymptomatic microscopic hematuria that had been detected by a school screening in August 2011.
Results
The baseline serum levels of indoxyl sulfate and p-cresyl sulfate in the patients on chronic dialysis were significantly higher than those in the children with microscopic hematuria. The baseline serum levels of p-cresyl sulfate in the peritoneal dialysis group were significantly higher than those in the hemodialysis group. There were no significant changes in the levels of these uremic solutes after 12-week VSL#3 treatment in the patients on chronic dialysis.
Conclusion
The levels of the uremic toxins p-cresyl sulfate and indoxyl sulfate are highly elevated in pediatric patients on dialysis, but there was no significant effect by probiotics on the reduction of uremic toxins in pediatric dialysis patients. Therefore, studies for other medical intervention to reduce uremic toxins are also necessary in pediatric patients on dialysis.
Introduction
Loss of kidney function induces accumulation of a variety of substances that can cause uremia syndrome. These substances are small water-soluble solutes, protein-bound solutes and middle-molecule solutes1,2). Protein-bound solutes, such as indoxyl sulfate and p-cresyl sulfate, are excreted by the kidneys via proximal tubular secretion and they accumulate in the blood of patients with chronic kidney disease (CKD)1,2). The conventional renal replacement therapies can only partially remove these protein-bound solutes as opposed to small water-soluble solutes, because they are bound to albumin3,4). The average levels of p-cresyl sulfate in patients undergoing hemodialysis (HD) are 10 times the normal levels5). p-Cresol, which exists mainly as p-cresyl sulfate in blood, is generated by the partial breakdown of tyrosine and phenylalanine by intestinal obligate or facultative anaerobes, and it is associated with infection, cardiovascular disease, and mortality5,6). This solute depresses the respiratory burst activity of phagocytes and endothelial cell response to inflammatory cytokines. Indoxyl sulfate, an end product of bacterial metabolism of tryptophan, is considered to be a key player in increased glomerular sclerosis and progression of CKD4,7,8). Indoxyl sulfate is known as to be involved in the pathogenesis of atherosclerosis.
The production of these uremic solutes originates from bacterial protein fermentation in the intestine and is influenced by the intestinal environment such as intestinal flora and pH. The bowel environmental differences, including prolonged transit time in the colon, constipation, and abnormal intestinal flora, are usually observed in end-stage renal disease (ESRD) patients because of diet restriction and uremia. The bacterial composition of the intestines in ESRD patients is different from that of the normal population. The proportion of aerobic bacteria such as enterobacteria and enterococci in patients with HD is approximately 100 times the normal level9). Since p-cresyl sulfate and indoxyl sulfate are mainly produced by these aerobes, generation of toxic microbial protein metabolites is increased in ESRD patients9). To reduce the production of toxic metabolites originating from bacterial fermentation, it is important to modulate bacterial growth in the intestine. Probiotics are defined by the World Health Organization as living microorganisms that, when administered in an adequate amount, confer a health benefit on the host. Probiotics can help restore intestinal microflora by reducing proteolytic bacteria and increasing saccharolytic bacteria in addition to improving bowel habits. Finally, probiotics have been known to reduce uremic toxins in the blood by correcting the intestinal microflora7,9).
In recent studies, probiotics treatment has contributed to reduction of the serum level of protein-bound solutes, such as indoxyl sulfate and p-cresyl sulfate, in adult HD patients8,10). However, there is little data regarding the levels of indoxyl sulfate and p-cresyl sulfate and the effects of probiotics on these uremic retention solutes in pediatric patients on dialysis.
The aims of this study were to investigate 1) the levels of indoxyl sulfate and p-cresyl sulfate in pediatric patients on dialysis and the differences in these uremic toxins levels by dialysis modality, 2) the relationship between indoxyl sulfate and p-cresyl sulfate, 3) the effect of probiotics to reduce uremic toxins and their safety in pediatric patients on dialysis.
Materials and methods
1. Patients
For the study design, a minimal sample size calculation was made based on a statistical power of 80% and a significance level at 0.05 under two-tail analysis. According to the results, we enrolled the 20 pediatric patients on chronic dialysis from one dialysis unit located in Seoul, Republic of Korea, at the initiation of this trial. Finally, 16 patients completed the study during 12 weeks.
Five patients were on HD, and 11 patients were on peritoneal dialysis (PD). This study was conducted from December 2010 to May 2011. The exclusion criteria were: 1) patients who had been on dialysis for less than 3 months; 2) patients who had acute infectious disease, including acute gastroenteritis; 3) patients currently on antibiotic treatment.
As there is no data for the normal range of indoxyl sulfate and p-cresyl sulfate in Korean children, we included 16 children as a control group, who visited the outpatient clinic for asymptomatic microscopic hematuria detected by school screening in August 2011. They showed a normal range of serum urea nitrogen and creatinine.
2. Study design
A single-center, prospective, nonrandomized, open-label study was designed. The 16 patients on chronic dialysis received VLS#3 once daily, 30 minutes after a meal for 12 weeks. VSL#3 is a high-concentration (450 billion viable cells/sachet) probiotic preparation of eight live freeze-dried bacterial species that are normal components of the human gastrointestinal microflora, including four strains of lactobacilli (Lactobacillus casei, Lactobacillus plantarum, Lactobacillus acidophilus, and Lactobacillus Delbrueckii subsp. bulgaricus), three strains of bifidobacteria (Bifidobacterium longum, Bifidobacterium breve, and Bifidobacterium infantis), and Streptococcus salivarius subsp. thermophilus. The dose given to patients is shown in Table 1. The dose was prescribed on the basis of the recommendation on the label and is approved by the Korea Food and Drug Administration. The patients were asked to answer a questionnaire regarding compliance, defecation, change in bowel habits, and adverse events during the study period when they visited the outpatient clinic or dialysis unit. There was no restriction on patients' everyday diet, medication, or daily activities. None of the patients who completed the study used antibiotics during the study period.
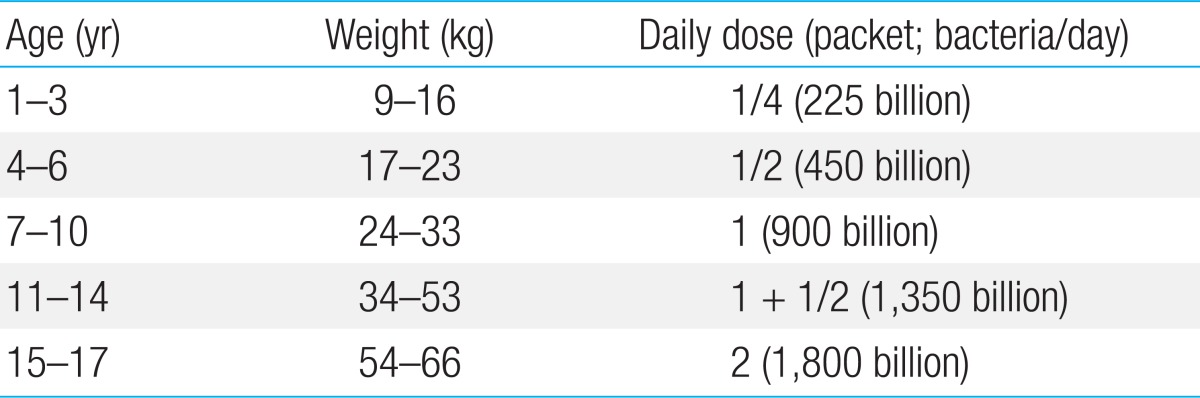
Probiotic treatment doses
This study was approved by the ethics committee of Samsung Medical Center. All participants gave written informed consent.
3. Laboratory evaluation
After the patients provided informed consents, a baseline evaluation was made during the midweek dialysis session in HD patients or during the outpatient clinic visit in PD patients. All blood parameters were measured before the first intake of probiotics and 4, 8, and 12 weeks after taking VSL#3, which include blood urea nitrogen, creatinine, electrolyte, bicarbonate, parathyroid hormone, calcium, phosphate, uric acid, protein, albumin, aspartate aminotransferase, alanine aminotransferase, glucose, insulin, complete blood count, indoxyl sulfate, and p-cresyl sulfate. C-reactive protein and normalized protein catabolic rate (nPCR) were measured in patients on HD. Dialysis adequacy was evaluated by renal Kt/V and total Kt/V in patients on chronic dialysis. The serum levels of indoxyl sulfate and p-cresyl sulfate were measured by fluorescence liquid chromatography.
4. Statistical analysis
The descriptive data were expressed as the median. Laboratory data were expressed as the mean±standard deviation. Differences between patients and control subjects were evaluated using Mann-Whitney U-test. Sperman's rank correlation test was used to analyze the correlation between serum levels of p-cresyl sulfate and indoxyl sulfate. Wilconxon signed-rank sum test was used for comparison of levels before and after probiotic administration in each patient group. P values less than 0.05 were considered statistically significant. All statistical analyses were conducted using the IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA).
Results
1. Study population
Patient characteristics are summarized in Table 2. The median duration of dialysis at the time of the study was 30 months in the HD group and 27 months in the PD group. The PD patients were older and heavier than HD patients. There was no significant difference in the level of body mass index between the HD group and PD group. Table 3 summarizes the baseline laboratory findings of the control and patient groups prior to starting the probiotics. There was no significant difference in the level of blood urea nitrogen between the HD group and PD group. Dialysis adequacy seemed to meet the Kidney Disease Outcomes Quality Initiative guideline. The level of nPCR was above 1.0 g/kg/day in HD patients and the protein intake seemed to be adequate. There was no significant difference in the laboratory findings before and after the probiotics treatment in HD and PD patients.
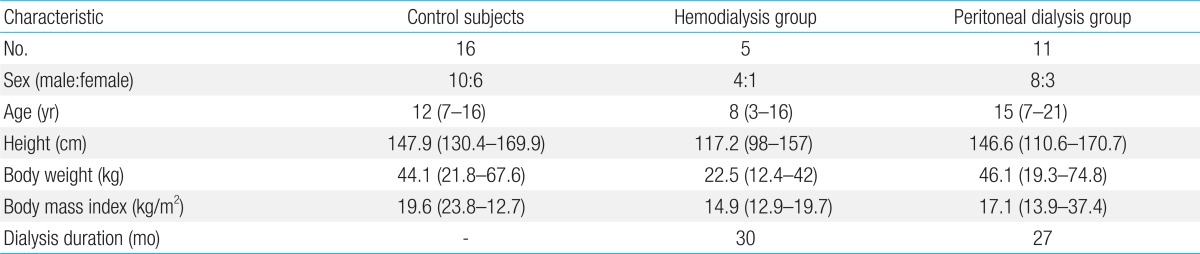
Characteristics of controls and patients
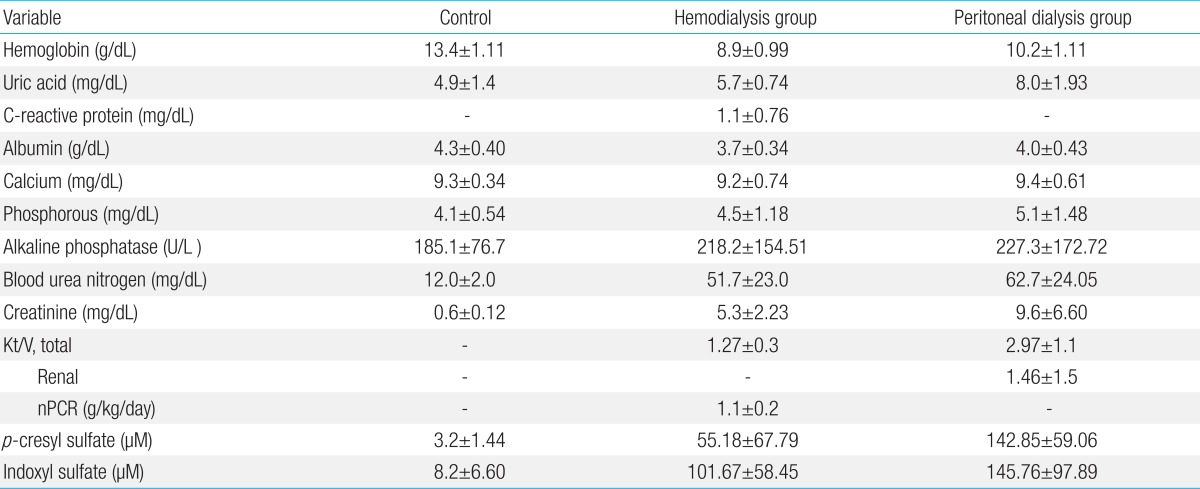
Laboratory findings for the controls and patients before probiotic treatment
2. Serum concentrations of indoxyl sulfate and p-cresyl sulfate before taking VSL#3
Comparisons of baseline levels of p-cresyl sulfate and indoxyl sulfate between the control group and patient group are summarized in Table 4 and depicted in Fig. 1. The serum levels of p-cresyl sulfate and indoxyl sulfate in the patient groups were significantly higher than those in the control group before taking VSL#3. The serum level of p-cresyl sulfate in the PD group was significantly higher than that of the HD group (142.85±59.06 µM vs. 55.18±67.79 µM, P=0.047). There was no significant difference in the serum level of indoxyl sulfate between the HD group and the PD group.
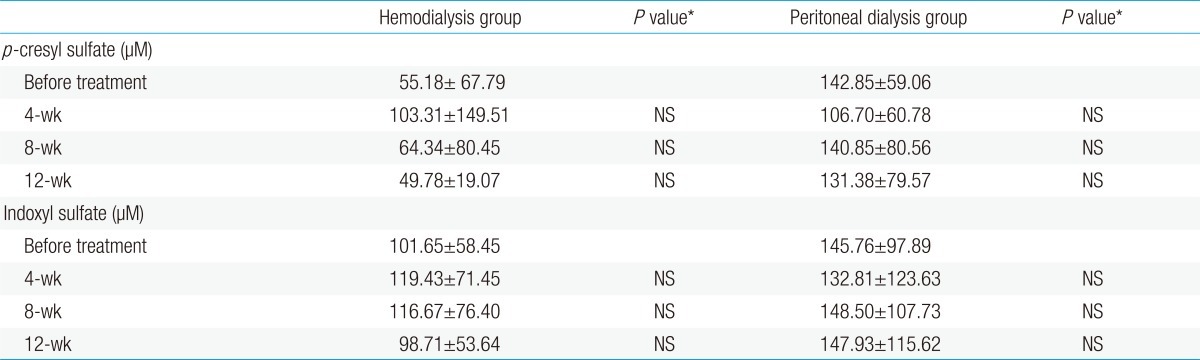
Effects of probiotic treatment on serum levels of uremic toxins
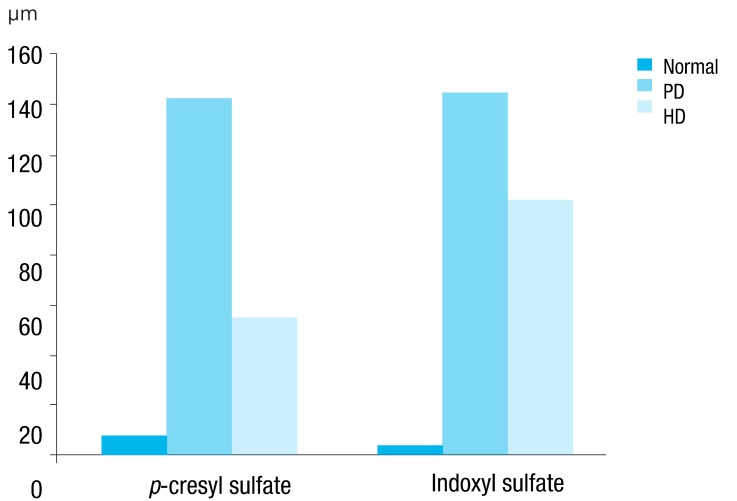
Serum levels of indoxyl sulfate and p-cresyl sulfate in controls and patients. PD, peritoneal dialysis; HD, hemodialysis.
In the correlation analysis, there was no correlation between serum indoxyl sulfate and p-cresyl sulfate in pediatric patients on dialysis.
3. Efficacy evaluation
The adherence to the study was excellent, and no patient discontinued probiotics treatment during the study period, except 4 patients, who were excluded from the study because of kidney transplantation or taking antibiotics. The results of the questionnaires during the outpatient clinic showed that the prescribed dose was well tolerated, and there were no serious adverse effects during VSL#3 therapy. Intention to treat analysis of changes in serum indoxyl sulfate and p-cresyl sulfate at 12 weeks demonstrated that there were no significant changes in the level of p-cresyl sulfate and indoxyl sulfate in patients on HD and PD during VSL#3 treatment (Table 4).
Discussion
In this study, we found that the serum levels of protein-bound solutes, such as p-cresyl sulfate and indoxyl sulfate, in pediatric patients on chronic dialysis were much higher than those of unbound solutes such as urea. Whereas the average levels of serum urea were about 5 times the levels in the control group, the average levels of serum p-cresyl sulfate in our HD group were about 17 times the levels in the control group. Previously reported serum concentrations of p-cresyl sulfate in adult patients on HD were about 10 to 12 times the levels in healthy volunteers5,11). This result possibly suggests that the clearance of protein bound solutes was much lower in pediatric patients than that in adult patients. It is possible that the age or body size also might affect the serum levels of p-cresyl sulfate in addition to the dialysis modality. We suspect that the high protein diet, the bowel environment, and dialysis adequacy in pediatric patients could be related to the higher protein-bound uremic toxin levels compared to those of adult patients. The serum levels of these two toxins can be evaluated by various kinds of liquid chromatography and the parallel investigation by the same method is needed in adults and pediatric patients to evaluate the difference of the serum levels of p-cresyl sulfate regarding to age3,4,6,8).
In our results, the serum p-cresyl sulfate level of PD group was higher than HD group. It has been known that the clearance of protein-bound solutes is lower for PD than for HD12,13). The clearance of protein-bound solutes during HD can maximize the gradient by high dialysate flow. However, the clearance of protein-bound protein in PD cannot easily be increased, and the volume of dialysate and membrane mass transfer area coefficient are much lower for PD than for HD14,15). Previous studies found that residual renal function plays a more important role in the clearance of protein-bound protein than in the clearance of water-soluble molecules in PD patients, and residual renal function contributed to more than two-thirds of p-cresyl sulfate clearance16,17). In recent years, it has been shown that serum indoxyl sulfate and p-cresyl sulfate might be involved in vascular damage and cardiovascular mortality in CKD18). In addition to cardiovascular disease, it has been known that serum indoxyl sulfate and p-cresyl sulfate levels might predict the risk of renal progression in patients having different stages of CKD18). Because the pediatric ESRD patients tend to receive PD instead of HD, the clinical outcomes by protein bound solutes should be evaluated regarding the dialysis modality in pediatric patients.
In our study, there was no correlation between serum indoxyl sulfate and p-cresyl sulfate in pediatric patients on dialysis. Although indoxyl sulfate and p-cresyl sulfate share some characteristics, such as the albumin-binding site and low clearance by dialysis, it is known that indoxyl sulfate and p-cresyl sulfate serum concentrations are not associated, and our results were compatible with the previous report6).
In our study, there were no significant changes in the levels of p-cresyl sulfate and indoxyl sulfate in patients on HD and PD during VSL#3 therapy. The small sample size of 16 patients raised concerns as to its statistical power. More than 21 participants are needed for a statistical power of 80% and a significance level at 0.05 under two-tail analysis. Although we tried to enroll more than 21 pediatric patients on chronic dialysis, a total of 20 patients participated at the initiation of this trial and 4 patients were dropped during 3 months of follow-up. Two patients were dropped due to kidney transplantation and the two other patients were given antibiotics during the trial.
We guess that not only the factors associated with probiotics, but also other factors such as carbohydrate to protein ratio, colonic transit, other medications, dialysis adequacy, or residual renal function could influence uremic toxin levels. Both the form and dosage of probiotics can affect the serum levels of uremic toxins. Since probiotics are more effective in the gastroresistant seamless capsule, the form of probiotics can influence uremic toxin levels. The bacterial components of VSL#3 remain viable in human ileostomy effluent and, in vivo, VSL#3 bacteria are able to survive passage through the ileocecal tract and reach the large bowel19). Analysis of fecal samples obtained from healthy volunteers showed that the main components of VSL#3 persisted in the gastrointestinal tract during treatment and a short period after discontinuation of VSL#320). Recently, synbiotics, which combine probiotics and prebiotics, have been used to improve the intestinal environment and bowel habits and reduce uremic toxins10). Prebiotics include carbohydrate fibers called oligosaccharides, which remain in the digestive tract and stimulate the growth of beneficial bacteria10). Synbiotics treatment is known to be more effective for improving intestinal environments in various medical conditions, including ESRD patients than probiotics only10). Synbiotics treatment is not available for pediatric patient. We used the usual dose of VSL#3, which is recommended on the label. There were no serious adverse effects, and this dosage was well tolerated in our patients. We guess that the effects of VSL#3 can be significant in patients on dialysis if the treatment dose is titrated on the basis of tolerability and stool analysis.
Generation of uremic solutes can be modulated by increasing carbohydrates and reducing protein intake. In our study, nPCR was investigated at baseline, 4 weeks, 8 weeks, and 12 weeks in patients with HD and it seemed that the levels of nPCR decreased during the study from 1 g/kg/day to 0.9 g/kg/day. This finding suggested that the protein intake in HD patients might influence the levels of p-cresyl sulfate and indoxyl sulfate. Colonic transit time may also affect the generation of uremic toxins. Prolonged colonic transit might result in increased generation and absorption of uremic toxins. Most patients reported that their bowel habits improved, but we could not evaluate the change in bowel habits by score. Although we excluded the patients who were taking antibiotics, other drug therapies such as phosphate binders can affect the colonic environment7,21). Although the change was not statistically significant, the serum level of p-cresyl sulfate decreased in the HD and PD group after VSL#3 therapy. The serum level of p-cresyl sulfate increased from the baseline at 4 weeks in patients on HD and it is possible that the dialysis adequacy was insufficient during that period in a few patients. Three patients showed lower levels of total Kt/V below 1.0 at 4 weeks, which recovered to baseline at 8 and 12 weeks and the serum level of p-cresyl sulfate increased in these patients at 4 weeks.
In conclusion, uremic toxins such as p-cresyl sulfate and indoxyl sulfate are highly elevated in pediatric patients on dialysis, and p-cresyl sulfate levels in PD patients were significantly higher than those in HD patients. In this study, there was no significant effect by probiotics on the reduction of uremic toxins in pediatric dialysis patients. Future studies, including more pediatric patients on dialysis, are needed to evaluate the levels and clinical outcomes of p-cresyl sulfate and indoxyl sulfate and compare the difference of these toxins regarding the dialysis modality. It is also known that uremic toxins such as p-cresyl sulfate and indoxyl sulfate can be reduced by the oral charcoal adsorbent AST-120 (Kremezin, Kureha Co., Tokyo, Japan), which has been proven to be capable of absorbing uremic toxins and attenuating the oxidative stress generated by them18). Therefore, studies for other medical intervention such as charcoal adsorbent to reduce uremic toxins are also necessary in pediatric patients on dialysis.
Acknowledgments
This work was supported by a grant from the Korean Society of Pediatric Nephrology in 2011.
Notes
No potential conflict of interest relevant to this article was reported.