

Introduction
Transcatheter closure is widely considered as treatment of choice for patients diagnosed with patent ductus arteriosus (PDA). Since the first experience of the transcatheter occlusion of PDA by Porstmann et al. in 19671), technical improvements over the years have increased the proportion of patients who undergo successful transcatheter closure2, 3). Despite the advancement in the procedure, there are limitations in transcatheter closure of PDA in small children. There is the difficulty in advancing the tighter curves through the right heart with a large tubular sheath in small children4). Left pulmonary artery stenosis due to protrusion of device into the left pulmonary artery has been detected with the greater frequency in the smaller children5-7). The procedure was generally recommended only for children weighing over 7 to 8 kg because the size of the patients' femoral vessel was relatively smaller than the size of the required delivery system. In the past when a larger device was used, the procedure was only recommended for patients weighing over 10 to 12 kg8). We reviewed our experience to determine the efficacy and safety of transcatheter PDA closure in infants weighing less than 10 kg, with regard to rates of success and complications.
Materials and methods
1. Subjects
A total of 314 patients underwent transcatheter occlusion of PDA at Severance Cardiovascular Hospital from January, 2003 to December, 2009. Among them, 115 (37%) patients (male 49, female 66), weighing less than 10 kg, were enrolled in this study. We retrospectively analyzed medical records, echocardiographic findings, angiographic findings, hemodynamic data and follow-up results of these patients.
2. Echocardiographic and cardiac catheterization parameters
After confirming left to right shunting through the PDA, the size of PDA was measured on color Doppler echocardiography. The left ventricular end-diastolic dimension (LVEDD) was measured in each patient on M-mode echocardiogram. Hemodynamic studies were performed, and the ratio of pulmonary blood flow to systemic flow (Qp/Qs ratio) was obtained in each patient during cardiac catheterization. Aortograms were obtained in the right anterior oblique 30 degree and lateral view. The maximum diameter of the narrowest portion of the ductus was measured on frozen image and balloon occlusion sizing was performed, if needed. The residual shunt was identified by aortogram, 10 to 15 minutes after the implantation of the device.
3. Follow-up protocol
Chest X-ray and transthoracic echocardiography were conducted at 24 hours after the procedure to evaluate the shape and position of the device. The patients underwent clinical evaluation and echocardiography at 1 week, 1, 3, 6 and 12 months after the procedure and then annually thereafter. All patients were followed according to this protocol. Major complications investigated during the research included failure of device implantation, embolization of device, residual shunt, significant obstruction of aortic arch or left pulmonary artery, infective endocarditis and massive blood loss. Mild narrowing (peak velocity under the 1.5 m/sec) of left pulmonary artery or aorta and transient weak arterial pulse were regarded as minor complications. A peak velocity over the 1.5 m/sec of the left pulmonary artery or descending aorta was considered as acquired stenosis. The difference in the LVEDD before and after PDA closure was evaluated.
Results
1. Characteristics of subjects
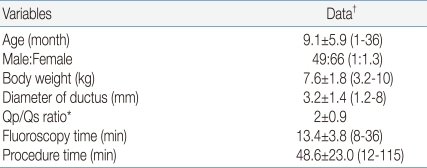
The patients' mean age was 9.1±5.9 months (range: 1-36 months), 49 were male and 66 were female, the mean weight was 7.6±1.8 kg (range: 3.2-10 kg). The mean diameter of PDA was 3.2±1.4 mm (range: 1.2 to 8 mm), the mean pulmonary blood flow to systemic flow (Qp/Qs) ratio was 2.0±0.9, and the mean fluoroscopic time was 13.4±3.8 minutes. The mean procedure time was 48.6±23.0 minutes (range: 12 to 115 minutes) (Table 1). The patients who were performed concomitant procedure such as percutaneous transluminal angioplasty (PTA) or percutaneous pulmonary valve angioplasty (PPV) have also been included in the study. PDA was presented as an isolated lesion in 75 (63%) patients, associated heart lesions were as follows: ventricular septal defect (VSD, n=13), atrial septal defect (ASD, n=11), coarctation of aorta (CoA, n=9), congenital aortic valve stenosis (AS, n=3), hypoplastic left pulmonary artery (n=3) and endocardial cushion defect (n=1). Some patients had one or more comorbidities (Table 2). Four patients had Down syndrome.
2. Results of the procedures
Of the 115 patients, the device was successfully deployed in 114 patients (99%). COOK Detachable Coil® (COOK Medical Inc, Bloomington, IN, USA) (n=2, 2%), Nit-Occlud® (PFM AG, Cologne, Germany) (n=60, 52%) and Amplatzer duct occluder® (ADO, AGA Medical Corp., Plymouth, MN, USA) (n=53, 46%) were used (Fig. 1). Coils were favored in cases of a rather small ductus, and in cases of moderate to large ductus, ADO was used.
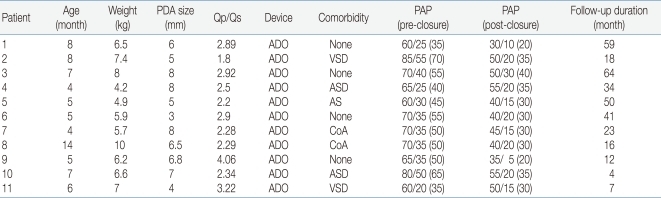
Sixty patients (52%) had increased LVEDD and 41 patients showed normalization at 1-week echocardiographic follow-up. The LVEDD had decreased from a mean of 31.2±4.7 to 28.8±4.6 mm at 1-month follow-up. The mean systolic pulmonary artery pressure was 34.6±1.4 mmHg (range: 15 to 85 mmHg). Pulmonary hypertension, evaluated during cardiac catheterization, was defined as pulmonary artery systolic pressure more than 40 mmHg9). Thirty-four patients had pulmonary hypertension. Pulmonary hypertension, evaluated using TR jet pressure and septal configuration on echocardiography, regressed in all 34 patients during follow-up. Among them, 11 patients had severe pulmonary hypertension with pulmonary artery systolic pressure of more than 60 mmHg. The clinical characteristics and treatment results of these patients are summarizes in Table 3. Most of them presented with large PDA, and seven patients had associated heart lesions; 2 had VSD, 2 had ASD, 1 had CoA and 1 had AS. Immediately after the procedure, 5 patients showed normalization of pulmonary artery pressure. Five patients showed normalization of pulmonary artery pressure at 1-month echocardiographic follow-up and the remaining patient showed normalization at 3-month follow-up.
3. Failure
Failure occurred in a 3-month-old infant weighting 5.8 kg with 4 mm ductus. The patient was also diagnosed as atrial septal defect and coarctation of aorta. Initially, the 6/4 ADO device was successfully deployed in this patient and was observed in the intensive care unit. However, position of device was unstable on follow-up echocardiography after one day. As a result, the patient was then referred for surgery.
4. Complication
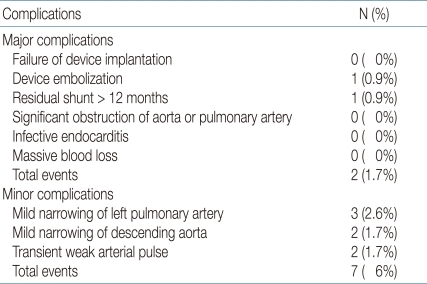
The mean follow-up duration was 21.0±19.6 months (range: 3 to 82 months). Of the 114 patients with successful deployment of a device, residual shunt was noted in one patient at 3-year echocardiographic follow-up. The patient was a 3-month-old infant weighing 7.7 kg with 3 mm ductus. The PDA was closed using 6×5 mm Nit-Occlud®(pfm AG, Köln, Germany). There still remained a very small residual shunt of PDA at his last echocardiographic follow-up, 3 years after the procedure. There were no complications related to vascular access, hemolysis and massive blood loss in any of the patient. However, in two patients, after the implantation of the ADO, mild narrowing of descending aorta was noted. One of the patients, 1 month-old boy, weighing 3.2 kg, underwent transcatheter closure using 6/4 mm ADO. A peak velocity on Doppler echocardiography after the procedure was 1.5 m/sec, but the echocardiography revealed progressive narrowing of the aorta, resulting in a peak velocity ranging from 3.0 to 3.8 m/sec during follow-up at 2 months. PTA was performed for narrowing of the aorta 3 months after the initial intervention. Aortogram showed a significant decrease in peak velocity of aorta from 3.8 m/sec to 1.5 m/sec. The other patient was a 4 month-old girl, weighing 4.2 kg with an 8mm duct and the PDA was closed using 6/4 mm ADO. After the procedure, on the echocardiography, a peak velocity of 2.0 m/sec was seen. On the follow-up echocardiography after 12 months, a peak velocity of 1.9 m/sec was seen. These patients are under close observation at outpatient clinic without further intervention so far. Three patients showed mild narrowing of left pulmonary artery, but their peak velocity on left pulmonary artery only slightly increased (range: 1.3 m/sec to 1.5 m/sec). After the procedure, 2 patients had transient weak pulse on femoral artery, which was managed by continuous infusion of heparin, and they all recovered their femoral artery pulse tension the next day (Table 4).
Discussion
PDA occurs in 5-10% of all congenital heart defects10). Once the diagnosis of the uncomplicated PDA is established, closure is recommended by surgery or catheter occlusion to avoid pulmonary overflow and prevent infective endocarditis10, 11). Transcatheter closure of PDA has been the mainstay of treatment in children and adults12). Fortescue et al. presented retrospective case series of 1808 patients with transcatheter closure of PDA in a report published in 2010. Overall PDA closure rate was 94 percent and major adverse events were 1.5 percent11). There have been only a few minor complications compared with the initial interventional data13, 14). Nevertheless, procedure-associated complications have been still described in different age groups, and they are relatively major in infants4-6). Information is also inadequate regarding safety and feasibility of transcatheter closure in infants15, 16). Few studies have investigated their usefulness in children weighing less than 10 kg17, 18).
Our current study is mainly focused on the clinical results in using either Nit-Occlud®, ADO or COOK Detachable Coil® for the transcatheter closure of PDA in children weighing less than 10 kg. Completely successful closure of PDA was achieved in 98% of the patients19). This confirms the safety of transcatheter closure of PDA in children weighing less than 10 kg. In previous report by Kim et al.2), mean age of 150 patients was 38 months and mean body weight was 15 kg in our center; however, current study focused on younger and smaller patients.
The incidence of PDA is higher in premature infants10). Jung20) reported that incidence in preterm infants with persistent patency of the ductus arteriosus is about 16 times more than full term infants. Delayed closure of the hemodynamically significant patent ductus arteriosus is related to the development of various morbidity in preterm infants21). Transcatheter closure of PDA can be considered as treatment option to avoid the risk of surgical ligation in these patients22).
The important factors for successful procedure are vascular accessibility, morphology of ductus, availability of device, and imaging modality. First of all, the vascular accessibility is an important variable. There is a high potential of thrombosis formation or interruption in femoral vessel related to vascular access, because the diameter of the femoral vessel in infants is small. Also, a more invasive approach such as cut-down of femoral vessel may be necessary during catheterization. Second, in addition to measurement of the diameter, the morphology of the ductus should also be assessed by echocardiography before procedure is performed. With careful regard to anatomic details and cautious planning of device deployment, procedural risks can be minimized and success rates can be maximized. Third, the miniaturization of device is also an important variable. Catheter manipulations within the heart have to be minimized to prevent injury and to avoid causing arrhythmias and hemodynamic instability. There is also the possibility of narrowing of adjacent aorta from protrusion of the aortic retention disc3). Further development in device can potentially improve the scope of catheter closure for ducts in preterm infants. Recently, Amplatzer duct occluder (ADO) II, a new device designed by the AGA Medical (Golden Valley, Minnesota) show successful PDA closure and decrease the risk in small patients23). Finally, the imaging modality is also an important factor. Because it is difficult for very small infants to maintain their vital signs such as body temperature and respiration without assistance, the procedure by the bedside maybe more suitable than at the catheterization laboratory. If portable imaging modality can be used during procedures, the risk of transcatheter closure for PDA will decrease in small infants.
Surgical ligation of PDA remains the treatment of choice in small children. Surgical morbidity, cost, and hospital length of stay have been decreased by the technique of video-assisted thoracoscopic ligation of the PDA24). However, through our current study transcatheter closure for PDA of infants has somewhat established its safety and efficacy. Carefully selected group of infants may be offered transcatheter closure as a treatment option with great caution.
With careful planning and improvement of imaging modality, transcatheter closure for PDA can be successfully accomplished in preterm infants. Furthermore, transcatheter closure of PDA can be accepted as the gold standard of treatment in patients of PDA weighing less than 10 kg in the near future soon.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


