


Introduction
In epidemiologic studies and clinical practice, atopic sensitization is defined as a positive allergen-specific serum immunoglobulin E (IgE) test or skin prick test to any food or inhalant allergens. It is an important risk factor for the development of asthma and allergic diseases1,2). The pattern of atopic sensitization changes dynamically with age throughout childhood3). It is also well established that allergen exposure in early childhood is an important risk factor for subsequent atopic sensitization4). Although some studies have suggested a possible linear dose.response relationship between early life exposure to allergens and the subsequent development of sensitization5,6), the development of atopic sensitization is the result of a complex interplay of genetic and environmental factors1,2,7). Therefore, our review aimed to (1) describe the prevalence of atopic sensitization in infants and young children, (2) describe the change in patterns of sensitization to common allergens across different age groups, and (3) to discuss the determinants of atopic sensitization in infants and young children.
Prevalence of atopic sensitization in infants and young children
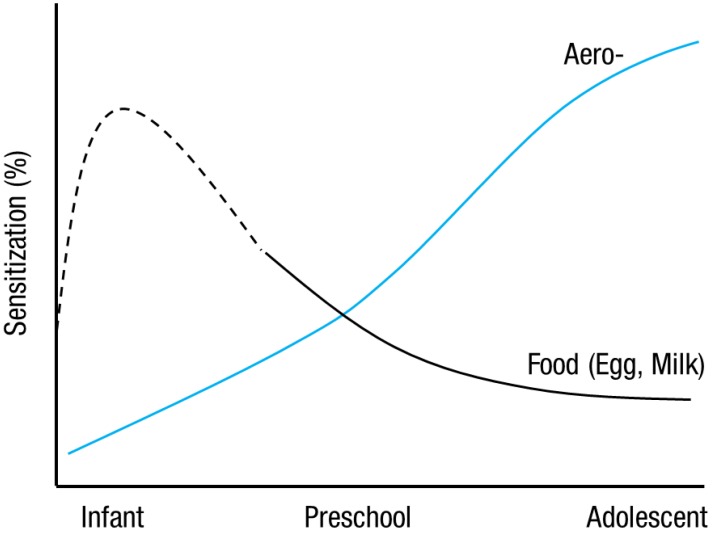
The prevalence of atopic sensitization is steadily increasing in Korea3) and globally. In a prospective German birth cohort study, the prevalence of sensitization to any allergens, as indicated by serum-specific IgE tests, increased from 11% at the age of 1 year to 30% at the age of 6 years. This increase was due to markedly increasing sensitization rates to inhalant allergens (rising from 1.5% to 26%)8). In population-based studies in preschool children aged 3-6 years in Korea, the prevalence of sensitization to aeroallergens increased from 4% to 21%, whereas the prevalence of sensitization to food allergens (e.g., egg, milk, and peanut) using skin prick testing changed from 10% to 2%9). Taken together, it seems that the prevalence of atopic sensitization differs regarding aeroallergens and class I food allergens; there is an increase in sensitization to aeroallergens, and a decrease in sensitization to class I food allergens, with increasing age in young children (Fig. 1). In a nationwide study in Korea, the prevalence of sensitization to aeroallergens was 41.1% in children aged 6-7 years2); these rates are similar to those from westernized countries8,10).
Patterns of sensitization in infants and preschool children
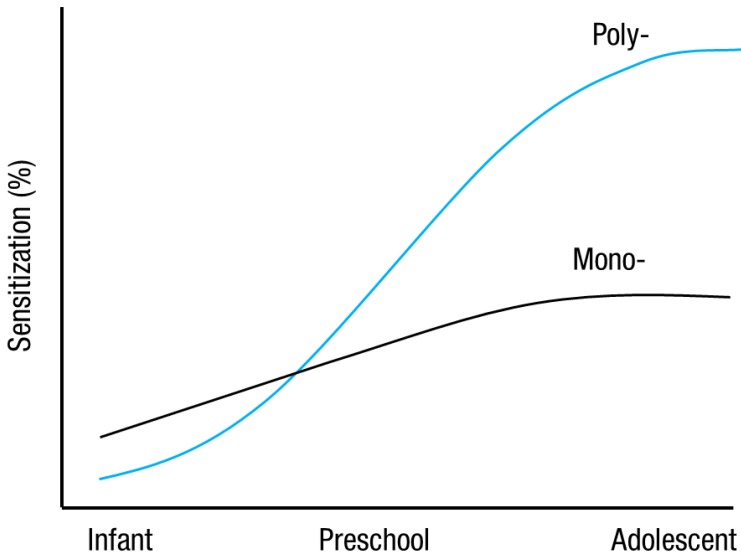
Although sensitization to allergens may develop early in life, sensitization patterns in children change dynamically with age3). Studies have shown that subjects who develop sensitization to food during early infancy tend to become tolerant11,12). On the contrary, a Swedish birth cohort study showed that the prevalence of sensitization among children sensitized to inhalant allergens almost doubled between the age of 4 and 8 years, a finding that suggests the existence of a prominent, dynamic process of sensitization to inhalant allergens in preschool-aged children13). Thus, the incidence of sensitization to food allergens decreases with increasing age in young children, whereas the incidence of sensitization to inhalant allergens increases with age3,8). Interestingly, polysensitization to multiple allergens is also common in atopic children and is associated with more severe allergic diseases2,3). Of note, some monosensitized children are likely to become polysensitized throughout childhood. In an earlier study, Kim et al.3) examined Korean preschool-aged children and found that the proportion of polysensitized children increased gradually with age, from 8.4% at the age of 3 years to 22.4% at the age of 6 years. The results showed that the sensitization to pollen allergens and the prevalence of polysensitization increased with age (Fig. 2). This finding clearly shows that house dust mite sensitization and pollen sensitization play a "triggering" role in the development of polysensitization3,14). These results also suggest that the type and number of allergen sensitizations change dramatically between the age of 3 and 6 years3).
Determinants of atopic sensitization
1. The role of genetics in the development of atopy
Atopic sensitization is an adverse immune reaction involving the IgE system1,7). Previous studies on twins and families suggest that atopy has a genetic component15). Recently, genetic association studies have shown that many genomic regions have linkage with atopic phenotypes16,17,18). Furthermore, Chang et al.18) found that IgE production in preschool-aged children was associated with MHC class II antigen genes such as HLA-DPA1 and HLA-DQA1. These results suggest that altered immune remodeling in infancy and toddlerhood may prime infants for atopic sensitization in childhood, depending on HLA genotypes. Moreover, evidence shows that several genes are associated with elevated cord blood IgE (CB IgE) levels, and that gene-gene interactions for IgE production begin at a prenatal stage16,17). Previous studies also suggest that there are significant associations between elevated CB IgE levels and cytotoxic T-lymphocyte-associated protein 4 +49A allele17) and interleukin (IL) 13, chemokine ligand 17, and C-X-C motif chemokine 10 gene interactions16). Taken together, these studies suggest that different genes may play an important role in IgE production both before and after birth19).
2. The role of environmental factors in the development of sensitization
1) Allergen exposure
There is increasing evidence that cord blood mononuclear cells (CBMC) show different responses when stimulated by mitogens and a variety of allergens, suggesting that maternal exposure to antigens may affect the developing immune response of offspring through direct exposure of the fetus to the same antigens as they cross the placental barrier20). However, it must be emphasized that the occurrence of lymphoproliferative responses of the fetus does not necessarily imply that atopic sensitization has developed in utero. Smillie et al.21) found no relationship between CBMC immunoproliferative responses to dust mite extract and immunopurified Der p 1 and the level of maternal mite allergen exposure during pregnancy. Similarly, several recent studies found no relationship between maternal inhalant allergen exposure and specific CBMC proliferative responses21,22). Thus, CBMC proliferative responses are not related to maternal exposure to inhalant allergens and thus do not predict subsequent sensitization. In general, the evidence for atopic sensitization or priming during fetal life remains ambiguous.
There is a close relationship between maternal exposure to indoor allergens and the risk of subsequent sensitization to these allergens during the first years of life6,21,23). Several studies have confirmed a simple dose-response relationship between mite allergen exposure and specific sensitization in infants and children6,24). A recent study by Finn et al.23) reported that early postnatal environmental exposure to inhalant allergens affects later proliferative responses of peripheral blood mononuclear cells in children at risk of atopy. These results suggest that early postnatal exposure to inhalant allergens is important. Therefore, early infancy has been suggested as a critical period for primary sensitization to inhalant allergens.
2) Environmental tobacco smoke
Recently, some studies have reported a positive association between environmental tobacco smoke (ETS) exposure and atopic sensitization25,26,27,28). The German Multicentre Allergy Study found a significantly higher risk of sensitization to food allergens in infancy among children who had been exposed to prenatal or postnatal smoking26). Similarly, a prospective birth cohort study in Sweden indicated that ETS exposure in early infancy increased the risk of sensitization to food as well as to indoor inhalant allergens at the age of 4 years25). Thus, prenatal and postnatal ETS was associated with an increased risk of early atopic sensitization. An experimental study in mice showed that exposure to ETS not only induced a significant increase in ovalbumin (OVA)-specific IgE levels but also a distinct eosinophil-rich pulmonary inflammatory reaction29). They suggested that ETS directly disrupts the normal tolerogenic immune responses against harmless allergens such as OVA, thereby inducing primary atopic sensitization. Although not acting as allergens, prenatal or postnatal exposure to ETS has an adjuvant effect on atopic sensitization26). Furthermore, ETS seems to have a significant effect on atopic sensitization at a very early stage, even beginning during pregnancy30).
3) Air pollution
Some epidemiologic studies show a positive association between exposure to air pollution and allergic diseases in children31,32,33). However, the role of exposure to air pollution in the development of atopic sensitization remains elusive in young children. Previous studies found no association between sensitization and air pollution exposure34,35). One cohort study from Norway showed no association between lifetime air pollution exposure and sensitization to any allergen at the age of 9-10 years36). Recently, a meta-analysis based on health data available from five European birth cohorts assessed the effect of ambient air pollution on the development of allergic sensitization in children during the first 10 years of life and found that air pollution exposure was generally not associated with sensitization to common allergens37). These results indicate no overall association between exposure to the investigated traffic-related air pollution components and allergic sensitization in children.
4) Pet ownership
The effect of pet ownership in early life on the subsequent development of sensitization and atopic disease is uncertain38). Some studies found that exposure to cats and dogs in early infancy was associated with atopic sensitization and allergic diseases later in childhood6,39). In contrast, other studies found no association between Fel d 1 levels and cat dander sensitization40) or Can f 1 levels and dog dander sensitization41). A high-risk birth cohort study from Sweden found that there was no association between peak Fel d 1 exposure and sensitization to cat allergen at the age of 5 years, but that high-risk children may become sensitized to cat allergen with very low peak domestic exposure to cat allergen42). Thus, the effect of exposure to pets may be different in different relative risk groups, based on parental allergy. Furthermore, it has been shown that low levels of cat allergen exposure are associated with a higher risk of sensitization, and the dose-response relationship between cat allergen exposure and sensitization may not be linear38,42). Interestingly, recent studies have reported that many children who are exposed to a high level of cat allergen yield a modified T-helper type 2 response, characterized by the presence of IgG4 antibody to cat proteins without IgE response, which could be regarded as a form of tolerance38,43). These results indicate that the dose-response relationship between allergen exposure and sensitization may differ between allergens (e.g., a linear relationship for house dust mite and a bell-shaped relationship for cat)5,6,44). While some data indicate an association between exposure to dog allergen and sensitization to dog dander, there is little evidence to suggest that keeping a dog increases the risk of sensitization to dog allergens45). In addition, the effect of exposure to pets is likely to be different among children with genetic predispositions, based on parental history.
5) Sex
Boys are more likely to have atopic diseases in early childhood, including atopic sensitization, atopic dermatitis, and wheezing2,4,46). However, this sex difference is less pronounced after puberty as girls become more likely to have asthma and atopy throughout the reproductive years4). The hormonal changes accompanying puberty have been implicated in the decrease in the male/female ratio of hypersensitivity reactions47). In general, sex hormones have different effects on immunomodulators. Estrogens have a proinflammatory effect and may increase the susceptibility to atopy, whereas androgens appear to have an immunosuppressive effect and are likely to be protective against atopy47). Thus, the differences in sex hormones between boys and girls could theoretically explain variations in susceptibility to atopy in the timing of the onset of puberty4). However, sex hormone levels and patterns of secretion do not appear to differ by sex during infancy48). Therefore, these mechanisms cannot explain the finding of a male predominance for sensitization in infants. Although the exact pathophysiologic mechanisms of sex differences in atopy remain unclear, boys are likely to have a higher prevalence of sensitization than girls in early childhood2,4). In one study that examined peanut-specific IgE levels in patients with a history of nut sensitivity from England, there was no difference in sensitivity with age or sex, but males seemed to develop immediate hypersensitivity at an earlier age (median age, 5.8 years) compared with females (median age, 8.8 years)49). A recent study found that boys show an enhanced interferon-╬│, IL-5, and IL-13 response during the first three years of life compared with girls. Boys also showed increased rates of sensitization at the age of 1 year, and increased peripheral eosinophil counts at the age of 3 years50). Therefore, the differential expression of atopic sensitization between boys and girls in early childhood is accompanied by sex-specific differences in immune response profiles.
6) Month of birth
The first few months of life are considered a critical period in the development of atopic sensitization and diseases. Specifically, the season of birth is considered important because exposure to certain allergens or conditions (e.g., vitamin D status)51) in a particular season may affect the subsequent development of allergic diseases in children with a propensity to atopic manifestations52). Earlier studies have shown a positive association between sensitization to pollen and birth month between January and May53). Other studies have identified a trend towards an increased risk of developing grass pollen allergy in children born in the grass pollen season (May to June)54,55). Thus, close correlations exist between certain birth months and sensitization to inhalant allergens. These results suggest that early exposure to high quantities of allergens during a particular season of birth has an important effect on the development of atopic sensitization52).
Conclusions
Early childhood is considered an important period for immune development regarding expression of atopy. Atopic sensitization develops early in life and sensitization patterns in young children change dynamically with age. Although genetic factors remain an important risk factor for the development of atopy in children, atopy is the result of a complex gene-environment interaction. The environmental factors that play a role in the development of atopic sensitization can be identified, with a potential for intervention in infants and young children. Thus, caregivers for young children should be aware of the risk factors for the development of atopic sensitization and the role of gene-environment interactions. In addition, early identification of these determinants and environmental control during early life may reduce the risk of subsequent atopic sensitization in high-risk children based on parental allergy.
 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


