




Graphical abstract
Introduction
The field of pediatrics is dedicated to all aspects of the care and well-being of infants, children, and adolescents. Because children cannot advocate for themselves, pediatricians and government policymakers must be concerned with specific diseases as well as the environmental, psychosocial, cultural, and political influences that affect the health of children and their families [1]. Among these factors, managing nutrition is important to helping infants, children, and adolescents maintain a healthy weight and supporting their normal growth and development [2]. Their dietary intake must meet their energy requirements and provide the essential macro- and micronutrients required to sustain their vital processes. Nutrient deficiencies can limit growth and impair immune function and neurodevelopment. Nutrition and dietary intake patterns can also determine adult body composition, affecting the risk of chronic disease development [3].
Food consumption and dietary practices have recently changed in Asian countries [4]. National nutrition and health surveys with various periods and items have been conducted by governmental agencies in 15 Asian countries [5]. In Korea, several national cross-sectional nutrition surveys monitor children’s health data and environmental factors to discern their diet, nutritional status, and chronic disease burden [6]. A continuous dedicated national nutritional surveillance system could identify nutritional and health issues, help establish public health policies, and inform the development of nutritional recommendations.
To achieve a comprehensive understanding of the current nutritional research findings, this review focuses on the nutrition and dietary items in the Korea National Health and Nutrition Examination Survey (KNHANES) and the Korean Youth Risk Behavior Web-based Survey (KYRBS). We reviewed articles published in the last 5 years that reference survey data regarding nutritional status, dietary intake, and the association between diet and chronic diseases in infants, children, and adolescents. Our results will help pediatricians and other health care providers in monitoring children’s growth and development and providing consultation to children and their caregivers.
National surveys in Korea
1. Korea National Health and Nutrition Examination Survey
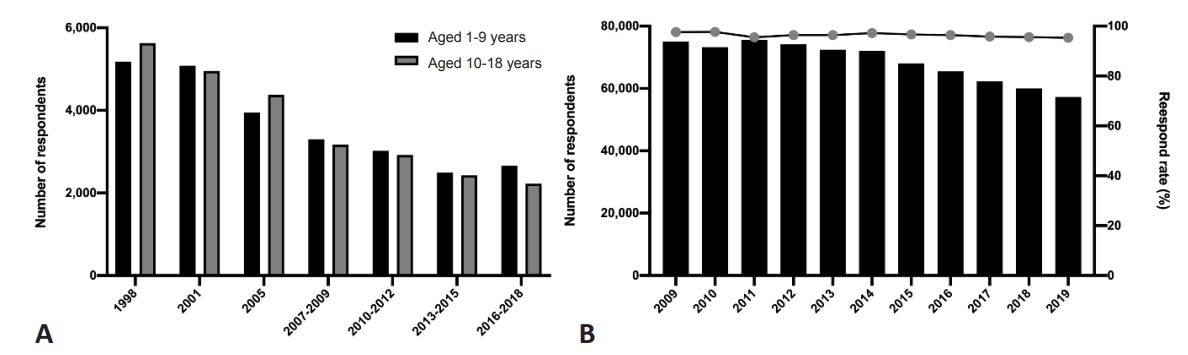
The KNHANES is a national survey that has monitored the health and nutritional status of adults and children in Korea since 1998 [7]. Its objective is to provide reliable nationally representative data on the health status, health behaviors, and food and nutrient intake of Koreans, thereby establishing a foundation for comprehensive national health promotion plans and programs [8]. The KNHANES was conducted every 3 years from the first period (1998) to the third period (2005) and has since become an annual survey system that has been conducted from the fourth period (2007–2009) to the present (Fig. 1A). This national survey was approved by the Research Ethics Review Committee of the Korea Centers for Disease Control and Prevention (KCDC). Stratified multistage cluster sampling and the rollingsampling method are used to ensure that each annual survey is representative of the overall Korean population [9]. The primary sample units (PSUs) are chosen from a sampling frame for all census or resident registration addresses. Each PSU consists of 50–60 households. After PSU selection, all housing units in the PSU were identified, and 20 households were selected for household screening by field surveys. In each household, all members older than 1 year were selected to participate in the final selection stage [9]. The KCDC publishes Korea health statistics annually, and the data are publicly accessible on the KNHANES website (http://knhanes.cdc.go.kr). Because the survey items differ among age groups, this review summarizes only the items for children and adolescents (Table 1). In addition, Table 2 shows the survey items (KNAHES VII [2016–2018]) [10] related to nutrition for children and adolescents.
2. Korean Youth Risk Behavior Web-based Survey
The KYRBS was established by the Korean Ministry of Education, Ministry of Health and Welfare, and the KCDC in 2005 (Fig. 1B) [11]. This annual school-based national cross-sectional survey monitors health-risk behaviors associated with noncommunicable diseases and unintentional injuries among Korean adolescents [12]. The KYRBS aims to provide data for the development of school health policies in Korea. A stratified multistage cluster sampling design was used to ensure a nationally representative sample of middle- and high-school students. The questionnaire contains 16 items about health-risk-related behaviors: dietary patterns, socioeconomic status, obesity and weight control efforts, mental health, oral health, personal hygiene, physical activity, injuries and safety awareness, violence, drinking, tobacco use, sexual behavior, drug use, allergic diseases (atopic dermatitis [AD] and asthma), internet addiction, and subjective health status (Table 1). The survey items related to nutrition consisted of dietary behaviors, nutritional education, and intake frequency of fruits, soda, highly caffeine beverages, sugary beverages, fast foods, vegetables, white or processed milk, dairy products (yogurt, cheese), and meals obtained at convenience stores (Table 2). Survey data are available to the public on the website (https://www.cdc.go.kr/yhs/).
Dietary behaviors
1. Feeding practices in infants
Proper feeding practices during infancy are necessary for infants and children to achieve adequate nutrition, well-being, and growth [13-15]. Infant feeding practices vary among locations, socioeconomic levels, and age groups [16-18], and few studies have cited scientific evidence [19]. Thus, it is necessary to review various guidelines and national survey studies to determine the optimal infant feeding practices in Korea.
Infant feeding practices consist of breastmilk, formula, and complementary feeding (CF). The Korean Academy of Pediatrics, American Academy of Pediatrics (AAP), World Health Organization (WHO), and United Nation’s International Children’s Emergency Fund strongly recommended exclusive breastfeeding (EBF) for the first 6 months of life and continued breastfeeding up to 24 months of age or beyond [20-23]. A positional paper published by the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) suggested that EBF be promoted until the baby is at least 4 months of age [24]. According to a study using KNHANES data from 2013–2015, mixed formula and breastmilk were the most common feeding practices in Korea for children aged 1–3 years [25]. Compared with previous KNHANES studies of children aged 1–3 years, the EBF rate decreased, and the rate of mixed feeding increased [26].
Offering CF during the weaning period is important because it must meet the appropriate nutritional requirements and allow children to experience foods with various flavors and textures. Recommendations for when to introduce CF differ among guidelines according to the expected health outcomes. The AAP and WHO recommend nutritionally adequate and safe CF (solids and liquids other than breastmilk or infant formula) starting from of 6 months age [27,28]. The introduction of CF before 6 months could increase the risk of obesity and diabetes in adulthood, reduce breastmilk consumption, increase the risk of choking and allergic reactions, and negatively influence the child’s behavioral and cognitive development [29-31]. On the other hand, an ESPGHAN committee suggested that CF not be introduced before 4 months or delayed beyond 6 months; in other words, ESPGHAN recommends starting CF at 17–26 weeks of age [32]. Because gastrointestinal and renal functions are adequately mature by approximately 4 months, full-term infants with normal neurodevelopment could begin CF sooner than 6 months. Recent studies suggest that introducing CF with breastfeeding at 4 months could have beneficial effects on iron storage [33-35]. In addition, prolonged EBF can lead to iron deficiency (ID), so CF should not be delayed beyond 6 months [36,37]. The introduction of allergenic foods is described below in the “Allergic diseases” section.
Using KNHANES data, Yon et al. [38] found that a delayed introduction of CF was associated with a risk of early childhood caries. A systematic review in the United States reported that age at the introduction of CF was not associated with weight, body circumference, or length among healthy infants [39]. A survey study reported that 25% of Koreans introduced CF at 4–5 months of age, while 64.3% of Koreans introduced CF at 6–7 months of age [40]. Only 0.4% started CF earlier than 4 months of age, a figure that was significantly lower than the 20.6% reported in 1993 [41]. Kim et al. [25] reported that the mean starting time for CF was 6.2 months of age. Further studies are needed to establish optimal feeding practice guidelines for infants and children in Korea and individually apply appropriate feeding practices as determined by various related factors.
2. Breakfast
Breakfast consumption is important to ensuring adequate total daily dietary intake and good health [42,43]. A recent US analysis of National Health and Nutrition Examination Survey 2005–2012 data reported that skipping breakfast is associated with low diet quality in young children (2–12 years) [44]. Those researchers found that overall diet quality scores as well as the subscale scores for fruit, whole fruit, whole grains, dairy, and empty calories were significantly better in children who ate breakfast; those who skipped breakfast consumed nearly 40% of their caloric intake from snacks [44]. In addition, several studies reported positive associations between measures of adiposity and cardiometabolic risk factors (e.g., glucose, insulin, triglycerides [TG], total cholesterol, low-density lipoprotein cholesterol) and skipping breakfast in children [45-47]. In Korea, the prevalence of skipping breakfast has increased over the past decade. According to KNHANES data, 11.1% of 6–11-year-olds and 27.0% of 12–18-year-olds skipped breakfast in 2008, while 15.0% of 6–11-year-olds and 37.4% of 12–18-year-olds skipped breakfast in 2018 [48]. Recent studies of KNHANES [49-52] and KYRBS [53] data reported that breakfast consumption is associated with dietary environment, adequacy of nutrient intake, and dietary habits (Table 3). Yu and Yang [50] reported that the frequency of eating breakfast among elementary school students (6–11 years) correlated with the dietary lifestyle factors of their parents (e.g., parents’ breakfast consumption frequency, dietary condition), and the group that skipped breakfast had a higher rate of a daily intake below the estimated average requirement (EAR) for iron than the group that ate breakfast. Associations between breakfast consumption and overall dietary habits and dietary intake adequacy were also reported in adolescents (12–18 years) [49,51-53]. Furthermore, consuming breakfast as a family is positively correlated with the nutritional quality of breakfast among Korean school-aged children and adolescents [49,53]. Further studies are needed to investigate the impact of breakfast consumption on overall daily dietary quality and nutritional status among Korean children and adolescents, and continued nutritional education efforts should reinforce the importance of eating a balanced breakfast.
3. Fast/processed foods
In recent decades, people’s dietary patterns have transformed to include an increased consumption of fast and processed foods [54,55]. In previous studies based on a US national survey, children and adolescents who ate fast food, compared with those who did not, consumed more total energy, fat, saturated fat, added sugars, and sugar-sweetened beverages; less milk; and fewer fruits and nonstarchy vegetables [56,57]. The rate of fast food consumption (25.5%) more than 3 times a week among adolescents has doubled over the past 10 years, and boys (27.5 %) had a higher consumption rate than girls (23.4%) [58]. In addition, 39.1% of boys and 40.7% of girls replaced meals with convenience store foods, particularly noodles (69.3%), kimbap (55.5%), and beverages (42.1%) [59]. In previous studies of KYRBS data, frequent fast and convenience store food consumption was associated with body mass index (BMI) [60,61] and mental status, including depression and subjective happiness (Table 3) [62,63]. However, no study using national survey data published during the past 5 years has quantitatively evaluated how frequency of fast or convenience store food consumption by Korean children and adolescents affects their nutrient intake. Thus, further studies are needed of the ways in which fast and convenience store food consumption affect the diet quality and health of Korean children and adolescents. Moreover, further research is needed to develop a comprehensive food and nutrient database of fast/processed foods to help studies examine the relationship between their consumption and children and adolescents’ diet quality and health.
4. Sugar-sweetened beverages
Sugar-sweetened beverages, such as soft drinks and sports drinks, and juices that are less than 100% fruit juice, can contribute excess calories and provide little or no key nutrients [64]. A recent systematic review and meta-analysis of prospective cohort studies and randomized controlled trials provided evidence that sugar-sweetened beverage consumption promotes weight gain in children and adults [65]. In addition, a meta-analysis reported that the habitual consumption of sugar-sweetened beverages was associated with the development of metabolic syndrome (MetS) and type 2 diabetes in adults [66].
In Korea, the overall mean daily beverage consumption among children and adolescents increased to 107.8 g and 203.9 g in 2018 from 53.0 g and 91.1 g in 2008, respectively [48]. Recent KYRBS data also showed increasing trends in the consumption of carbonated drinks, sugar-sweetened beverages, and energy drinks by adolescents [59]. A study of KNHANES data reported that carbonated beverages had the highest intake rate and sugar content among beverages consumed by children aged 6–11 years [67]. This study found positive associations between the intake of sugary and carbonated beverages and childhood obesity. In the past 5 years, studies were published on beverage consumption and its influence on adolescents [68,69]. as well as on the associations between beverage consumption and self-rated health status and mental health using KYRBS data (Table 3) [63,70]. Sugar-sweetened beverage consumption among Korean children and adolescents should be monitored, and further studies are warranted to provide scientific evidence of association between the effects of beverage consumption and the quantity and quality of dietary intake among Korean children and adolescents. Examinations of the long-term effects of sugar beverage consumption on health among Korean children and adolescents are also necessary to provide dietary guidelines for the prevention of pediatric obesity.
5. Excess sodium
A high sodium intake is a leading contributor to elevated blood pressure and responsible for a high incidence of cardiovascular events [71]. The WHO recommends a sodium intake of less than 2 g/day (equivalent to less than 5 g/day of salt) in adults to reduce blood pressure and the risk of cardiovascular disease (CVD) [72]. The average sodium intake in Korea is high, with about half the population consuming more than 4 g/day, twice the recommended upper limit [73,74]. To improve the safety of children’s diets including reducing the sodium served in food to children, the Special Act on Safety Management of Children’s Dietary Lifestyle went into effect in 2009 [73,75]. This act limited the selling and advertising of energy-dense, nutrition-poor foods that children commonly eat and required that packaged foods contain nutrition labels that included the sodium content [73,75]. The 2018 KNHANES report indicated that mean sodium intakes were 1,749.0 mg in subjects aged 1–9 years and 3,165.9 mg in subjects aged 10–18 years [48]. Although there was decreasing trend in sodium consumption over 10 years, it was still double the recommended intake. Boys, older adolescents, and those who frequently eat out had higher sodium intakes than their counterparts [76]. Lee et al. [77] reported that adolescents with high sodium excretion levels showed an increased risk of being overweight and having central obesity compared with those with low urinary sodium excretion levels. Similarly, a significant positive association was found between urinary/dietary sodium intake and adiposity in children and adolescents [78]. In addition, sodium intake as estimated by urinary sodium excretion (e.g., urinary sodium concentration, urinary sodium concentration to urinary creatinine ratio, urinary sodium concentration to specific gravity ratio) was positively associated with insulin resistance or metabolic abnormalities in children and adolescents [79-82]. Further studies are needed to explore the association between excessive sodium intake and long-term health among Korean children and adolescents. Developments in dietary/nutritional education programs targeting children and adolescents are also important for reducing excessive sodium intake.
Nutritional status
1. Vitamin D
Vitamin D plays a significant role in the regulation of calcium metabolism and mineral and calcium homeostasis [83]. The key role of vitamin D is improving calcium absorption ability in the small intestine [84]. Vitamin D is formed by the action of ultraviolet light from the sun on chemicals naturally found in the skin. However, it is difficult to obtain adequate amounts of vitamin D from food alone; sunlight is its most important source [85].
Serum 25-hydroxyvitamin (25(OH))D concentration is the most widely used measurement of vitamin D status [86]. However, the normal range of vitamin D concentrations in children and adolescents in Korea has not been established. Vitamin D status differs by region and race, so it is difficult to adopt recommendations from countries that do not consider Korean characteristics and geographical factors. The dietary vitamin D requirement depends on the amount of exposure an infant receives to sunlight [87]. A nursing baby’s vitamin D levels do not change with the mother’s dietary intake of vitamin D. The AAP recommends that all children, including EBF infants, be supplemented with 400 IU of vitamin D per day because human milk typically contains a vitamin D concentration of 25 IU/L or less [22,88,89].
Dietary reference intakes for Koreans consider the minimum required intake to prevent vitamin D deficiency, the intake needed to prevent the risk of adverse effects from excessive vitamin D intake, and the consumption behavior and lifestyles of Koreans. Because the scientific evidence needed to estimate vitamin D requirements in Koreans is still lacking, a reference was set as an adequate intake (AI) that reflects the intake when serum 25(OH)D levels reach the optimal range. The AI of vitamin D is 5 µg (200 IU)/day for infants and children under 11 years of age and 10 µg (400 IU)/day for anyone 12 years of age and older. Supplementation with vitamin D or an adequate dietary intake of vitamin D is required for children who are infrequently outdoors, which makes it difficult to synthesize vitamin D from ultraviolet rays [90].
Several studies have used KNHANES data to examine the prevalence and trends of vitamin D status in children and adolescents (Table 4). Studies using KNHANES 2008–2014 data reported a significant trend toward lower serum 25(OH)D levels and a significant increase in the prevalence of vitamin D deficiency in all age groups [91,92]. In addition, studies have noted that winter season, higher education levels, lack of vitamin D supplementation, old age, female sex, urban residence, and a high BMI were independent factors contributing to a low vitamin D level [93,94]. Vitamin D supplementation could be suggested depending on the mentioned risk factors associated with a low vitamin D status.
In addition to demonstrating one’s bone health, vitamin D levels are considered related to chronic diseases, including CVD, hypertension, diabetes, MetS, autoimmune conditions, infectious/inflammatory diseases, and cancer [83,87]. Recent studies of Korean children and adolescents reported that vitamin D deficiency is associated with obesity, nonalcoholic fatty liver disease, MetS, insulin resistance, and cardiometabolic risks (Table 4) [95-99]. In addition, based on KNHANES data studies have associated the prevalence of vitamin D deficiency with dental caries, ID, myopia, and immunoglobulin E levels [100-103]. The mechanisms of the association between vitamin D and chronic diseases remain unclear, and further investigations are needed to elucidate the pathogenesis.
2. Iron
Iron is an important factor for virtually all living organisms that participates in a wide range of metabolic processes, including oxygen transport, deoxyribonucleic acid synthesis, and electron transport [104,105]. In the human body, iron exists predominantly in complex forms bound to protein (hemoprotein) as heme compounds (hemoglobin or myoglobin), heme enzymes, or nonheme compounds (flavin-iron enzymes, transferrin, and ferritin) [106,107].
ID in children is a common problem associated with defects in cognitive and psychomotor development, behavioral problems, diminished growth, and diminished immune response, even in the absence of anemia [108,109]. To prevent ID anemia (IDA), the AAP, ESPGHAN, and WHO emphasize the need to provide dietary sources of iron (e.g., beef, iron-fortified grain meals) from the introduction of CF rather than medicinal iron supplementation [24,33,110]. The majority of full-term babies are born with sufficient iron stores that are not depleted until they are 4–6 months of age [107], and breastfeeding is more beneficial for preventing ID than formula because of the high bioavailability of iron in breastmilk. However, if a full-term breastfed infant is unable to consume enough iron from CF after 6 months of age, an oral iron supplement should be used [88,110]. Raw milk should not be fed to children younger than 12 months, and consuming iron-rich foods along with vitamin C is a great way to prevent ID.
In Korea, the EAR was calculated using the amount of basic iron loss, increased blood volume during the growth period, and the amount needed to increase tissue and stored iron. The EAR was then used to establish the recommended dietary allowance (RDA). The AI of iron for 0- and 6-month-old infants has been estimated as 0.3 mg/day, largely based on the iron intake of EBF infants. The RDA for infants aged 6–11 months is 6 mg/day, while the tolerable upper intake level for those aged 0–14 years is 40 mg/day. The RDA of iron is 9 mg/day for children 6–8 years of age, 10 mg/day for those 9–11 years of age, 14 mg/day for those 12–18 years of age, and 16 mg/day for females aged 12–14 years to reflect menstrual blood loss [90].
Since 1998, the prevalence of anemia using KNHANES data has been reported as 7.4%–9.5% overall, with a prevalence of 2.2%–4.8% in men and 11.9%–16.5% in women [111]. Using KNHANES data from 2010, Lee et al. [112] showed that the prevalence of IDA in the Korean population aged 10 years and older was 0.7% in males and 8.0% in females and that low income, underweight status, or an iron- or vitamin C-poor diet was associated with IDA (Table 5). In a previous study based on KNHANES 2008 data, Kim et al. [113] showed that the prevalence of ID in males and females was 8.6% and 17.2% at ages 10–14 years and 3.9% and 24.1% at 15–17 years. Interestingly, a study based on KNHANES 2010–2012 data reported that the development of IDA in adolescents was correlated with a family history of IDA [114]. This finding indicates that maternal awareness and feeding practices can influence the risk of IDA in children. Further studies are needed to better understand the relationship between family characteristics and IDA in infants and adolescents. Two studies based on KNHANES 2010–2011 data investigated the association between ID and the levels of other divalent metals, such as cadmium and lead, in adolescents. ID was associated with increased blood cadmium concentrations and lead levels [115,116]. Iron shares similar absorption mechanisms with cadmium and lead; therefore, ID would result in excess cadmium and lead absorption [117]. In addition, animal studies have shown that ID predisposes animals to lead toxicity by increasing its absorption in the gastrointestinal tract [118]. Cadmium is a carcinogenic metal, while lead is a potential neurotoxin. Therefore, it is necessary to assess iron and hematologic status when addressing environmental exposure to cadmium or lead.
Chronic diseases and nutrition
1. Obesity
Obesity and overweight are characterized by excessive fat accumulation that can impair health. The WHO estimated that 38.2 million children under the age of 5 years were overweight or obese in 2019, while over 340 million children and adolescents aged 5–19 years were overweight or obese in 2016. The prevalence of overweight and obesity in that population was just over 18% in 2016 [119]. BMI, the most widely used measure for obesity and overweight, is defined as weight in kilograms divided by square of height in meters (kg/m2). Because KNHANES data regarding diagnoses of specific diseases were obtained through self-questionnaire and interviews, there are limitations in diagnostic accuracy compared to that by a physician. However, since the diagnosis of obesity can be defined by objective anthropometric measurements, many studies on obesity have been conducted using KNHANES data. A study on KNHANES and National School Health Examination (NSHE) data showed that the prevalence of obesity in children aged 6–18 years increased from 8.7% in 2007 to 15.0% in 2017 in the NSHE, while that in children aged 2–18 years increased from 8.6% in 2001 to 9.8% in 2017 in the KNHANES. In addition, there was a higher increase in the prevalence in boys and high-school students than in girls and younger students (Table 6) [120]. Obesity is a preventable disease, and it is important to identify its associated risk factors. There have been several studies of environmental risk factors associated with obesity. A study of KNHANES 2010–2012 data reported that current maternal smoking habits, low paternal education level, and low family income were potential risk factors for obesity in Korean children, although not statistically significant [121]. Another study of KNHANES 2008–2010 data identified that obesity was significantly associated with a mother’s working hours, especially among girls [122]. A recent systematic review and meta-analysis showed that childhood obesity is significantly associated with adult CVD risk factors including high blood pressure, high TG level, and low high-density lipoprotein cholesterol (HDL-C) [123]. A study of KNHANES 2005–2014 data found that a high waist circumference in adolescents was associated with an increased incidence of CVD risk factors [124]. The prevalence of MetS is high in childhood obesity and associated with CVD-related mortality [125]. When the modified National Cholesterol Education Program diagnostic criteria were applied to KNHANES data, the prevalence of MetS in Korea was 8.9% in 1998, 12.4% in 2001, 10.6% in 2005, 5.3% in 2008, and 4.8% in 2010 [126]. Cho et al. [127] reported that adolescents with severe obesity (≥120% of 95th BMI or a BMI >35 kg/m2) were associated with metabolic risk factors of HDL-C <40 mg/dL, TG ≥150 mg/dL, and a systolic blood pressure ≥130 mg/dL. In addition, there are several studies that obesity in adolescence was associated with thyroid dysfunction [128,129], reduced bone mass and density [130], and pulmonary dysfunction [127].
2. Allergic diseases
Diet might affect allergic disease susceptibility because it contributes to the regulation of the immune system [131]. Many recent studies reported the effects of the Western diet [132], vitamins [133,134], fiber [135], and fatty acids [136,137] on the development of allergic diseases and allergic sensitization. Furthermore, ideas have changed about the ways in which the introduction of CF could influence the development of food allergies. Current evidence does not support the idea that delaying the introduction of allergenic foods, including peanuts, eggs, and fish, beyond 4–6 months of age, prevents allergic diseases [138,139]. In infants at high risk for peanut allergy, recent guidelines now recommend the early introduction of peanut-containing products to prevent its development [140]. There is also a lack of data to indicate that partially or extensively hydrolyzed formula prevents allergic diseases [138,141]. EBF for 3–4 months has a weak protective effect on wheezing in the first 2 years of life, during which wheezing is associated with vital respiratory infection rather than atopic asthma [142]. However, it is important to evaluate which diet patterns might have preventive effects on allergic disease in Koreans because genetic-environmental interactions play a crucial role in the development of allergic diseases and food consumption patterns vary widely among geographical regions and cultures [143].
The KNHANES and KYRBS surveys provide data about the diagnoses of allergic diseases, including AD, asthma, and allergic rhinitis, through self-administered questionnaires. A few studies in the past 5 years have used these Korean survey data to examine the association between childhood allergic diseases and nutrition (Table 7). Lee et al. [144] reported that parents with allergic diseases preferred breastfeeding (37.5%) for a longer duration (mean, 11.06 months) than those without allergic diseases (28.5%; mean duration of breastfeeding, 9.93 months). Breastfeeding has been believed to have protective effects in preventing the development of AD [145,146]. However, a recent Cochrane review of 23 independent studies concluded that EBF beyond 3–4 months does not reduce the risk of AD [147]. In the Korean study by Lee et al. [144], EBF and breastfeeding duration were not significantly associated with AD.
Kim et al. [148] reported that a high consumption of fast food, snacks, sweetened beverages, vegetables, and fruits was significantly associated with allergic diseases. Kang et al. [149] found that a high consumption of fast food was significantly correlated with recent asthma and that there was no association between the consumption of fruits, vegetables, and milk and recent asthma. These results were consistent with those of previous studies in Western countries. An English birth cohort study showed that children aged 8 years who predominantly consumed a Western-style diet were significantly more likely to have doctor-diagnosed asthma [150]. Fast food, processed meat, cheese, and other dairy products are rich sources of saturated fat in the Western diet [151,152]. A high consumption of saturated fatty acids was significantly correlated with current asthma in Spanish school-aged children [153]. Thus, a strategy for managing a high fast food intake may be required in adolescents with allergic diseases.
Conclusions
Comprehensive data related to nutrition monitoring of infants, children, and adolescents gathered in the continuous KNHANES and KYRBS are publicly available to researchers on related websites. Because of standardized methods and protocols in these surveys, many studies have been published in the last 5 years about dietary intake (breakfast, fast/processed food, sugary beverages, sodium), and nutritional status, including vitamin D, iron, and obesity, based on laboratory tests and anthropometric measurements. There has been an increasing trend in children and teenagers who skip breakfast, eat fast food, consume sugary drinks, have vitamin D deficiency, and are obese. The identification of risk factors and the use of personal approaches to avoid these dietary patterns and nutritional status are required in clinics and schools. However, few studies have examined infant feeding patterns, food intake frequency in toddlers, objective laboratory nutritional status in children younger than 10 years, and dietary factors associated with allergic diseases. Further studies using Korean survey data are needed to identify dietary patterns in the first 2 years of life since they are important factors in neurodevelopment health and the development of atopic diseases.
This review could help pediatricians, nutritionists, and other health care practitioners who monitor the growth and development of Korean children and adolescents understand recent trends in dietary intake and nutritional status. It also may inform researchers and policymakers about diet-related policies and strategies for the prevention of chronic diseases in Korean children and adolescents.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


