




Introduction
The prevalence of childhood obesity is dramatically increasing in South Korea, which has been associated with changes in lifestyle, such as Westernized high-calorie, high-fat diet with sugar-sweetened beverages, sedentary lifestyles, and decreased physical activity [1]. In a recent report, the prevalence of obesity in children aged below 6 years increased from 1.4% in 2008 to 2.8% in 2015, and that in children and adolescents aged 7 to 18 years rapidly increased from 8.4% in 2008 to 14.3% in 2016 [1]. Accordingly, the prevalence of obesity-related physical, psychosocial, and metabolic complications, such as metabolic syndrome and nonalcoholic fatty liver disease (NAFLD), is also increasing in Korean children and adolescents [2].
Childhood obesity may persist lifelong if not treated properly; it can lead to adulthood obesity and a variety of metabolic and cardiovascular complications later in life. Thus, pediatric obesity is regarded as one of the priority health issues, and the treatment of childhood obesity and its complications may be one of the most effective strategies to reducing morbidities and mortalities and to saving hospital costs later in life.
Strict guidelines or consensus statements on the diagnosis and treatment of pediatric obesity have been published and updated in Western countries. However, to date, there are no evidence-based guidelines on pediatric obesity in Asia, including South Korea. Therefore, the Committee on Pediatric Obesity of the Korean Society of Pediatric Gastroenterology, Hepatology and Nutrition (KSPGHAN) developed an evidence-based guideline on the diagnosis and treatment of obesity in children and adolescents, to deliver a systematic approach to childhood obesity in South Korea.
Materials and methods
To develop the first evidence-based clinical practice guideline on the diagnosis and treatment of obesity in children and adolescents in South Korea, the Committee on Pediatric Obesity of the KSPGHAN established a Guideline Task Force (TF) in March 2017. This TF was composed of pediatric gastroenterologists with an expertise in clinical nutrition, as well as pediatric neuropsychiatrists, clinical nutrition specialists, and exercise specialists. Experts from these areas were designated to each TF subgroup according to their professional specialty.
A systematic protocol for the establishment of an evidence-based guideline for the diagnosis and treatment of obesity in children and adolescents was prepared and established through regular TF meetings. The basic format of the guideline was determined to encompass a total of eight topics within 5 different sections as follows:
(1) Definition and diagnosis of overweight and obesity in children and adolescents
(2) Principles of the treatment of pediatric obesity
(3) Behavioral interventions for children and adolescents with obesity
• Diet
• Exercise
• Lifestyle
• Mental health
(4) Pharmacotherapy in children and adolescents with obesity
(5) Bariatric surgery in children and adolescents with obesity
Each TF working subgroup searched all references related to pediatric obesity in each assigned field through PubMed search using MeSH terms, as well as all available references published in South Korea using appropriate systematic search strategies. These references included randomized controlled trials (RCTs), observational studies (e.g., case-control studies, prospective and retrospective cohort studies, case series studies), meta-analyses, systematic reviews, and previous obesity guidelines or position papers or consensuses on both children and adults with obesity through the entire period using a last search date of September 30 2018. Subsequently, each TF subgroup reviewed, analyzed, and summarized all related documents and references in each field.
To establish a systematic evidence-based guideline, the strength of evidence and grade of recommendation were determined for each recommendation according to a previously adapted classification system for evidence-based guidelines (Table 1) [3-5]. The strength of evidence was classified from level I to level V based on the value of the evidence in the literature, including systematic review, meta-analysis, and scientific papers: RCTs, well-designed trials, consensus studies, and opinions of research groups, respected authorities, and expert committees. Level I represents the strongest evidence.
The grade of recommendation was determined according to the strength of evidence and importance of the recommendation. Levels I to III evidence were decided to correspond to grades A to C of recommendations, which were regarded as highly recommended or recommended, respectively. Levels IV and V recommendations for were basically regarded as grade D; the final grade was decided through voting consensus of the entire TF. A total of three face-to-face meetings were held in Seoul and Jeju Island and 14 online video meetings to achieve consensus on all of the recommendations. All recommendations were voted on and accepted when 100% agreement was achieved.
1. Definition and diagnosis of overweight and obesity in children and adolescents
1-1. We suggest to use the Korean National Growth Charts body mass index (BMI) percentile to diagnose overweight and obesity in children and adolescents over 2 years of age. (strength of evidence, level III; grade of recommendation, C)
1-2. We suggest to diagnose overweight when the BMI is above the 85th but less than the 95th percentile for age and sex, and obesity when the BMI is above the 95th percentile in children and adolescents >2 years of age. (strength of evidence, III; grade of recommendation, C)
1-3. We suggest that children <24 months of age be diagnosed as overweight if their weight for height is above the 95th percentile on the Korean National Growth Charts, which introduced the World Health Organization (WHO) growth standards in this age valid. (strength of evidence, V; grade of recommendation, C, based on committee voting)
1-4. We recommend to assess comorbidities: NAFLD, dyslipidemia, hypertension, prediabetes, type II diabetes mellitus (DM), polycystic ovary syndrome, obstructive sleep apnea, and psychosocial problems. (strength of evidence, V; grade of recommendation, A, based on committee voting)
1-1. We suggest to use the Korean National Growth Charts BMI percentile to diagnose overweight and obesity in children and adolescents over 2 years of age. (strength of evidence, level III; grade of recommendation, C)
The Korean National Growth BMI charts are accepted as valid for Korean children and adolescents over 2 years of age and provide a means for determining changes in pediatric obesity prevalence [6]. The 2017 Korean National Growth Charts are recommended for the evaluation of body size and growth of Korean children and adolescents to use in practice and in the public health sector in South Korea [6].
A systematic review by the United States Preventive Services TF reported that the BMI of children and adolescents correlate well to the percentile of body fat [7]. In 1990s, an expert committee recommended using BMI for screening overweight in children and adolescents [8]. In the 2000 Centers for Disease Control (CDC) Growth Chart and 2011 United Kingdom (UK) Growth Chart (http://www.rcpch.ac.uk/growthcharts), the BMI chart is available for children and adolescents aged 2 to 20 years [9]. Meanwhile, a considerable proportion of boys and girls with relatively normal fat mass appear to be misclassified and may be at risk of being overweight based on the BMI criteria in a Korean study using the Korea National Health and Nutrition Examination Survey; their findings indicated that body fat mass and fat-free mass would be helpful for complementary assessment [10]. Despite some limitations, BMI is currently the most reasonable method for diagnosing overweight and obesity in children over 2 years old.
1-2. We suggest to diagnose overweight when the BMI is above the 85th but lower than the 95th percentile for age and sex, and obesity when the BMI exceeds the 95th percentile in children and adolescents over 2 years of age. (strength of evidence, III; grade of recommendation, C)
1-3. We suggest that children <24 months of age be diagnosed as overweight if their weight for height is above the 95th percentile on the Korean National Growth Charts, which introduced the WHO growth standards in this age group, as the Korean Society of Pediatrics has accepted this standard as valid. (strength of evidence, V; grade of recommendation, C, based on committee voting)
The Korean National Growth Chart recently revised the BMI cutoffs of obesity in children and adolescents. The criteria of obesity for children aged >2 years have changed from a BMI of ≥95th percentile for age and sex or BMI ≥25 kg/m2 to a BMI of ≥95th percentile for age and sex [6]. When applying a new BMI cutoff and a recently developed Korean National Growth Chart, a study reported that the prevalence of obesity is 10.3% in South Korea [6]. These criteria, based on the BMI percentiles, are the same as those used in United States of America (US), based on the CDC growth chart, and in the UK (http://www.rcpch.ac.uk/growthcharts) [9,11]. We could not find any meta-analysis or systematic review to justify applying the adult standards of BMI ≥25 kg/m2 to children, regardless of risk evaluations of comorbidities. In children aged under 2 years, the criteria of overweight were changed from weight for age to weight for height in a recent 2017 Korean Growth Chart after the introduction of the WHO Child Growth Standards [12].
Data suggest that severely obese children and adolescents have a worse risk factor profile compared with less obese children. In a large cross-sectional and longitudinal study in the US, 59% of children with BMI≥99th percentile had at least 2 risk factors, whereas 39% of children with BMI ≥95th percentile had at least 2 risk factors [13]. Consequently, expert committees in the US and Italy have suggested BMI≥99th percentile as severe obesity in older children [14,15]. In another proposed US guideline, extreme or class 2 obesity in children is defined as a BMI exceeding 120% of the 95th percentile or >35 kg/m2, and class 3 obesity to be BMI exceeding 140% of the 95th percentile or >40 kg/m2 [11]
WHO provides the values of BMI as ≥99th percentile and +3 standard deviations of z scores [16]. The WHO definition for severe obesity differs between age groups. The 99th percentile identifies “obesity” in the younger age group (0–5 years) and “severe obesity” in the older age group (5–18 years). This approach takes into account the difference in growth process between younger and older children. Few data are available on the significance of the cutoffs for the upper end of the BMI in preschool-aged children. Moreover, the WHO cutoffs for severe obesity have not been assessed yet.
The Korean Growth Chart also provides the curves of BMI ≥99th percentile and +3 standard deviations of z scores in its website (http://www.cdc.go.kr/).
2. Principles of the treatment of pediatric obesity
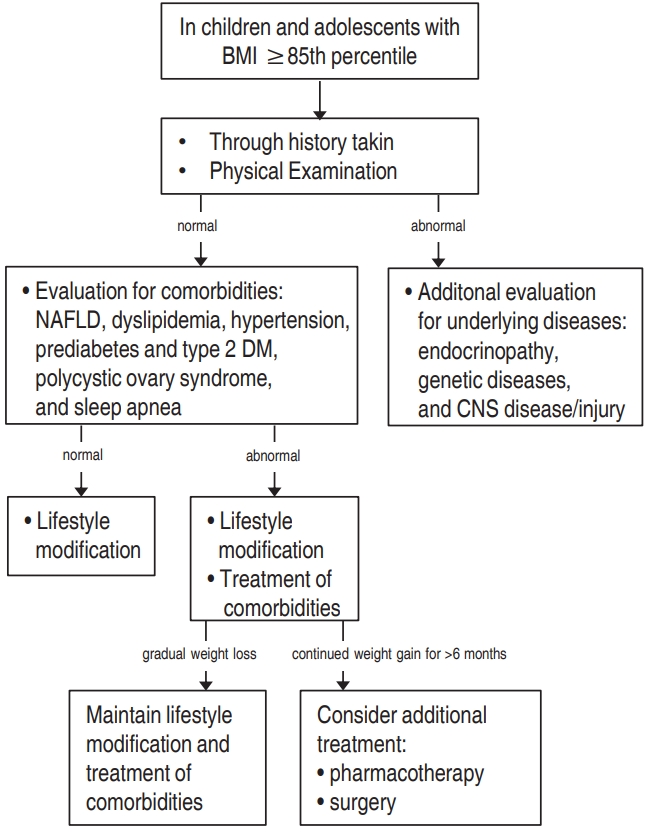
2-1. We recommend a treatment algorithm to help physicians determine the appropriate weight management stage for each patient, on the basis of his or her age, BMI percentile, and comorbidities. (strength of evidence, I; grade of recommendation, A)
2-2. We recommend a family-based, comprehensive, multidisciplinary team approach to succeed in behavioral interventions (active vigorous physical activity and reduction of inactivity, accompanied with calorie-controlled diet) for the treatment of obesity in children. (strength of evidence, I; grade of recommendation, A)
2-3. We recommend that pharmacotherapy and bariatric surgery be considered only in patients with morbid obesity with major comorbidities after a formal program of intensive lifestyle modification has failed. (strength of evidence, V; grade of recommendation, A, based on committee voting)
2-1. Treatment algorithm to help physicians determine the appropriate weight management stage for each patient, on the basis of his or her age, BMI percentile, and comorbidities (strength of evidence, I; grade of recommendation, A)
Behavioral interventions for lifestyle modification represent the key principle recommended for the treatment of overweight and obesity in children and adolescents. The following are the staged treatment strategies for pediatric obesity according to age and BMI percentile [23]:
1) Children aged 2–5 years
(1) BMI 85th–94th percentile (overweight)
The weight goal is weight maintenance until reaching a BMI below the 85th percentile or slowing of weight gain, as indicated by the downward deflection in the BMI curve.
(2) BMI 95th–98th percentile (obesity)
The weight goal is weight maintenance until reaching a BMI below the 85th percentile; however, if weight loss occurs with healthy, adequate-energy diet, it should not exceed 0.5 kg/mo. If greater weight loss is noted, monitor the patient for causes of excessive weight loss.
2) Children aged 6–11 years
(1) BMI 85th–94th percentile (overweight)
The weight goal is weight maintenance until reaching a BMI not exceeding the 85th percentile or slowing of weight gain, as indicated by the downward deflection in the BMI curve.
3) Adolescents aged 12–18 years
(1) BMI 85th–94th percentile (overweight)
The weight goal is weight maintenance until reaching a BMI not exceeding the 85th percentile or slowing of weight gain, as indicated by the downward deflection in the BMI curve.
2-2. We recommend a family-based, comprehensive, multidisciplinary team approach to succeed in behavioral interventions (active vigorous physical activity and reduction of inactivity, accompanied with calorie-controlled diet) for the treatment of obesity in children. (strength of evidence, I; grade of recommendation, A)
The interactions between parents and children and parenting styles strongly affect the unhealthy lifestyle habits of children [24]. Obese children are more likely to be bullied and have fewer friends or are less popular among classmates compared with thinner peers [25]. Parents, teachers, and friends have indicated that youths who are obese are easily isolated and have poorer social relationships compared with their counterparts [26]. Those with low self-esteem and higher BMIs are more likely to smoke and drink alcohol [27]. These children are also less athletic and are not expected to have romantic relationships. Thus, they tend to demonstrate teasing, worsening of self-esteem, feeling of loneliness, depression, anxiety, and an introverted personality [28].
Data from 133 RCTs enrolling 30,445 patients through 16 systemic reviews presented an evidence profile for each intervention, including medication, surgery, and lifestyle or community-based interventions, in overweight or obese children or adolescents. Physical activity interventions decrease systolic blood pressure (BP) and fasting glucose (low to moderate quality of evidence). Dietary interventions with low-carbohydrate diets have shown an effect in terms of BMI reduction (moderate quality of evidence). Educational interventions reduce waist circumference, BMI, and diastolic BP (low quality of evidence). Pharmacological interventions reduce BMI (metformin, sibutramine, and orlistat) and waist circumference (sibutramine and orlistat) as well as increase high-density lipoprotein cholesterol (sibutramine) but also raise systolic and diastolic BP (sibutramine). Surgical interventions (laparoscopic adjustable gastric banding, Roux-en-Y gastric bypass, and sleeve gastrectomy) have shown the largest BMI reduction (moderate quality of evidence). Combined interventions consisting of dietary modification, physical activity, behavioral therapy, and education significantly reduce systolic and diastolic BP, BMI, and triglycerides. Combined parent-child and parent-only interventions have similar effects on BMI (low quality of evidence) [29].
A school-based intervention reportedly reduces BP and body fat in young teenagers. Short-term cardiovascular health in children-targeted interventions showed successful results in demonstrating affected physiological variables according to increased time spent in moderate to vigorous physical activity at school (20 minutes per day in elementary schools, 30 minutes in middle schools) [30]. Both school-designed workout and adult supervision in physical activities affected the amount of physical activity of sixth to eighth graders participating in their free time [31].
A systemic analysis of 24 reports reviewing 15 studies showed strong evidence that reduced screen time and enhanced physical activity could prevent obesity. Data from 11,000 preschool children 4 to 6 years of age linked increased caloric intake from snacks and sugar-sweetened beverages with increased screen time [32]. Another study revealed that decreasing screen time also decreases sedentary time [33]. A 2-generation study associated increased BMI with 2 hours of screen time per day for both parents and offspring [34].
In a prospective cohort study in England of a family-based behavioral treatment in 33 families with severely obese children aged 8 to 13 years, the families were advised to practice self-monitoring, keeping daily food and activity records, goal setting, positive reinforcement, and stimulus control to modify the child’s eating and exercise behaviors. Foods were categorized into “traffic light” food colors of red, yellow, and green foods; physical activity aspects were also advised. Severely obese children were reported to have lost 8.4% of BMI over 3 months, maintained at the 3-month follow-up. Self-esteem and depression also improved significantly [35].
A study concerning the relationship between parenting style and development of obesity in children showed that authoritarian parenting is highly associated with the risk of being overweight among young children [24].
Interviews performed in children with obesity and parents with obese children revealed that a lifestyle behavior improvement program benefits from parental support and needs help from family, peers, and friends [36]. The studied children with obesity benefited from the persistent involvement of supportive persons in the maintenance of lifestyle behavior changes. The respondents expected to achieve weight reduction by physical activity or eating healthy meals. The parents reported struggling with adopting new rules and insufficient support from family members. Children reported suffering from inconsistent parenting and low support from their parents. Their experience of bullying at school was an obstacle to their ability to achieve the necessary changes. Support from peers stimulated their progress. Parents identified that the general practitioner is required to discuss overweight in a nonoffensive manner and to present interest in the process of weight reduction. The general practitioner should play a more supportive role [36].
The Oklahoma Chapter of the American Academy of Pediatrics Obesity Committee developed a resource toolkit for pediatric primary care providers to be used in behavioral counseling of obese children. Eight topics were selected for the handouts: sugarssweetened beverages, daily screen time, sleep, proper breakfast, family mealtime, physical activity, balanced meals, and food quality. The resource toolkit sets four steps, utilizing motivational interviewing techniques, to assist with facilitating behavior change: (1) obtaining patient history, (2) discussing health habits and the family’s reasons for changing habits, (3) setting a realistic goal for change, and (4) realizing goals. This handout also provides a patient questionnaire on health habits to assist with the identification of behaviors to be changed, eight provider and parent handouts on healthy behaviors, and a motivational interviewing guide [37].
Behavioral interventions target lifestyle change (e.g., counseling on diet, increasing physical activity or decreasing sedentary behavior, and addressing behavior change) to limit weight gain or decrease weight [38]. Effective behavioral interventions include parental support and the delivery of basic instructive information on healthy nutrition and physical activity. Additional components of the most effective interventions include the following: (1) being conducted in a specialty setting; (2) targeting both children and their parents; (3) helping parents and children engage in stimulus control (e.g., limiting access to tempting foods and limiting screen time); and (4) assisting participants in identifying goals, self-monitoring, and problem solving to accomplish their selected goals. Other common components include contingent use of rewards or reinforcement, motivational interviewing, teaching of coping skills, addressing body image, and the option of individual–family counseling to address family-specific issues. All of the effective studies have emphasized eating healthy foods and using moderate portions.
The distinguishing characteristics of comprehensive multidisciplinary interventions are increased intensity of behavioral change strategies, greater frequency of patient-provider contact, and involvement of specialists in the treatment. Formalized behavioral therapy and a multidisciplinary treatment team exceed the capacity of the services most primary care providers can supply.
Systematic evaluation of body measurements, dietary intake, and physical activity should be conducted at baseline and at specific intervals throughout a program. For the implementation of a comprehensive multidisciplinary intervention, the comprehensive treatment should be provided by a multidisciplinary obesity care team, including a behavioral counselor (for example, social worker, psychologist, other mental health care provider, or trained nurse practitioner), registered dietitian, and exercise specialist (physical activity specialist or another team member with training or a community program prepared to assist children with obesity).
2-3. We recommend that pharmacotherapy and bariatric surgery be considered only in patients with morbid obesity with major comorbidities after a formal program of intensive lifestyle modification has failed. (strength of evidence, V; grade of recommendation, A based on committee voting)
Pharmacotherapy should only be performed in accordance with lifestyle modification [39]. The prescription of weight-reducing medicines used off-label to adolescents under 16 years of age should be discouraged for the following reasons: (1) the lack of U.S. Food and Drug Administration (FDA) approval, (2) insufficient number of safety and efficacy studies performed in children and adolescents with obesity, (3) limited efficacy for most agents, and (4) the problem of drug-induced adverse reaction related with potential obesity-related morbidity and mortality. For obese youth who are unable to achieve sufficient weight loss with lifestyle interventions alone, adjunctive use of more intensive treatments, including pharmacotherapy, may be appropriate. However, the search for obesity medications that are proved to be safe for long-term use, efficacious to promote sufficient weight reduction, and have a good risk–benefit ratio remains fruitless. Nevertheless, there is great hope in the successful development of more effective, etiology-based antiobesity therapies for children and adults.
FDA-approved pharmacotherapy for obesity should be administered only with a concomitant lifestyle modification program of the highest intensity available, and only by clinicians who are experienced in the use of antiobesity agents and aware of their risk for adverse reactions [40]. Medication should be discontinued, and the patient re-evaluated, if the reduction in BMI or BMI z score is less than 4% after antiobesity medication for 12 weeks at full dosage [11].
In adolescents with extreme obesity, clinicians may consider bariatric procedures if the patient shows poor response to medical treatment for weight loss. Indications for bariatric surgery include BMI of >35 kg/m2, accompanying comorbidities of obesity such as type 2 DM, moderate-to-extreme sleep apnea, pseudotumor cerebri, debilitating orthopedic problems, and nonalcoholic steatohepatitis with advanced fibrosis. Another candidate profile for bariatric surgery is a BMI of >40 kg/m2 with mild comorbidities (hypertension, dyslipidemia, moderate orthopedic problems, mild sleep apnea, nonalcoholic steatohepatitis, and extreme psychological distress that is secondary to the obesity) [41,42].
3. Behavioral intervention for children and adolescents with obesity: diet
3-1. We recommend the decrease in intake of sugar-sweetened beverages. (strength of evidence, I; grade of recommendation, A)
3-2. We recommend the reduction in total energy intake. (strength of evidence, I; grade of recommendation, A)
3-3. We suggest the use of small-sized plates or bowls. (strength of evidence, III; grade of recommendation, C)
3-4. We suggest the decrease in consumption of fast food. (strength of evidence, III; grade of recommendation, C)
3-1. We recommend the decrease in intake of sugar-sweetened beverages. (strength of evidence, I; grade of recommendation, A)
The Korean National Health and Nutrition Examination Survey performed between 2008 and 2011 revealed that the mean amount of daily sugar-sweetened beverage consumption was 98.7 mL/day in school children, which tended to increase with age [43]. This Korean study revealed that overweight and obesity are significantly associated with high sugar-sweetened beverage intake among boys aged 7–12 years (odds ratio, 1.72) [43]. A randomized trial performed in adolescents aged 13 to 18 years demonstrated that BMI changes are significant between a sugar-sweetened beverage restricted group and a control group among subjects in the upper-baseline BMI percentile [44]. A more recent randomized trial that investigated the effects of an intervention designed to decrease consumption of sugar-sweetened beverages on weight gain showed significant differences in the BMI changes between the intervention group and control group at both 1 and 2 years among Hispanic adolescents [45]. Similar to the results from studies in older children, sugar-sweetened beverage consumption has been positively associated with BMI z scores in children at 4 and 5 years in a large-scale, longitudinal cohort study [46]. A recent systematic review revealed a significant positive association between sugar-sweetened beverage consumption and total adiposity among children under 12 years old [47]. A cross-sectional analysis of children’s dietary data reported that sugar-sweetened beverage intake is independently associated with alterations in lipid profiles, increased markers of inflammation, and increased waist circumference [48].
3-2. We recommend the reduction in total energy intake. (strength of evidence, I; grade of recommendation, A)
Current evidence suggests that weight status can be improved in overweight or obese children and adolescents by a reduced-energy diet. However, the association between weight improvement and macronutrient distribution of a reduced-energy diet is controversial in children and adolescents [49].
In an adult systemic review, the overweight and obese population who consumed low glycemic index food lost more weight and showed better improvement in lipid profiles [50]. A pediatric systematic review comparing low glycemic index/low glycemic load with high glycemic index/high glycemic load diets did not reveal the effect of weight loss; however, it reported decreases in serum triglyceride and HOMA (homeostasis model assessment) index [51].
Meanwhile, studies on the association between eating quickly and overweight/obesity have showed conflicting results. Several cohort studies conducted in Japan have demonstrated that eating quickly is significantly associated with overweight in girls [52,53]. A populationbased study conducted in Portugal reported no significant association between eating quickly and overweight/obesity [54].
There is weak evidence regarding the association between breakfast intake and obesity [55-58]. Likewise, current evidence does not show that the consumption of fruits and vegetable is associated with overweight and obesity in children and adolescents [59,60]. In an adult study, energy density independently affects energy intake; however, data are lacking for children and adolescents [61].
3-3. We suggest the use of small-sized plates or bowls. (strength of evidence, III; grade of recommendation, C)
Systematic reviews in adults have consistently shown that energy intake increases with larger portion sizes [61]. A recent systematic review showed that children also consistently consume more food and drink when offered larger-sized portions, packages, or tableware than when offered smaller-sized versions [62]. Total calorie consumption reportedly decreases in those receiving small portion sizes among children under 6 years of age [63,64]. A recent observational study revealed that reduced portion sizes are associated with BMI reduction after 1 and 2 years among children and adolescents [65].
3-4. We suggest the decrease in consumption of fast food. (strength of evidence, III; grade of recommendation, C)
The intake of fast food has an effect on overweight and obesity in school children and adolescents. Composition data from leading fast food company websites show that fast foods have very high energy density [66,67]. A Korean nationwide observational study performed in 2001 reported contrasting results regarding the association between fast food intake and overweight and obesity [68]. However, a recent large-scale observational study performed in Jeju Island revealed that obese children had significantly higher rates of fast food consumption [69].
4. Behavioral intervention for children and adolescents with obesity: exercise
4-1. We recommend physical activity, which is beneficial to all children and adolescents. (strength of evidence, I; grade of recommendation, A)
4-2. We recommend moderate to vigorous levels of physical activity, including regular and steady exercise, which is helpful in promoting a decrease in weight. The recommended duration of moderate to vigorous exercise is at least 20 minutes, with a goal of 60 minutes, 5 days per week. (strength of evidence, I; grade of recommendation, A)
4-3. We recommend programmed exercises, which are helpful in reducing body fat in children and adolescents. (strength of evidence, I; grade of recommendation, A)
4-1. Physical activity is beneficial to all children and adolescents. (strength of evidence, I; grade of recommendation, A)
Physical activity is especially effective in enhancing cardiovascular fitness, decreasing body fat, and lowering risk factors for diabetes [70-73]. Apart from the benefits for maintaining weight and reducing health risks related to childhood obesity, physical activity may prove to enhance aspects of children’s brain activation, including cognitive development [74,75]. Therefore, the WHO, American Alliance for Health, Physical Education, Recreation and Dance, British Association of Sport and Exercise Medicine, and Canadian Academy of Sport and Exercise Medicine recommend for children to participate in physical activities as early as possible. Guidelines that recommend suitable physical activities for each age group have also been formulated in developed countries.
(1) Children and youth aged 5–17 years should accumulate at least 60 minutes of moderate- to vigorous-intensity physical activity daily.
(2) Physical activity greater than 60 minutes in duration provide more health benefits.
(3) Most of the daily physical activity should be aerobic. Vigorous-intensity activities should be incorporated, including those that strengthen muscle and bone, and performed at least 3 times per week.
4-2. Moderate to vigorous levels of physical activity, including regular and steady exercise, are helpful in promoting a decrease in weight. (strength of evidence, I; grade of recommendation, A)
Regular exercises improve weight and BMI, as well as blood sugar and triglyceride levels [70,76-78]. The degree of weight loss is maximized when exercise is combined with decreased calorie intake, which is also helpful in sustaining improved weight after weight loss. The degree of weight loss is minimal in the absence of calorie intake restriction.
Moderate exercise refers to exercise that causes mild increases in breathing and heart rate [71,74]. In other words, conversation is doable during moderate exercise, whereas singing is difficult to perform simultaneously. Brisk walking, cycling, and practice in such sports as soccer, basketball, and badminton, are examples of moderate exercise. Meanwhile, conversation is difficult and singing impossible during vigorous exercise, owing to significant increases in breathing and heart rate. Running fast, jump rope workout, inline skating, and playing a game of soccer, basketball, or badminton are examples of vigorous exercise. At least 20 minutes of moderate exercise is recommended, with a goal of 60 minutes, 5 days per week, whereas vigorous exercise is effective when done 3 times per week [75,79,80].
4-3. Programmed exercises are helpful in reducing body fat in children and adolescents. (strength of evidence, I; grade of recommendation, A)
The effect of exercise programs is maximized with the involvement of a specialist to instruct the activity or when friends or family members participate in together [81-83]. The type, frequency, intensity, and duration of exercises should be included in the prescription of the program. Moreover, prescriptions for resistance training programs should be individualized to stimulate all of the major muscle groups and use all of the muscle groups [72].
In addition, exercise intensity should be adjusted stepwise according to age and BMI, rather than engaging in high-level exercise from the beginning [14]. Especially in patients with high-level obesity, weight-bearing exercise, such as excessive jump rope, should be avoided because repeated impact may be applied to parts such as knees, ankles, and hip joints (Table 3). However, according to a recent meta-analysis that investigated the impact of physical education on obesity prevention in children, adolescents, and adults, although physical education has positive effects on obesity-related body indices and health status, its effect is statistically insignificant. Moreover, there is lack of evidence based on data [72].
5. Behavioral intervention for children and adolescents with obesity: lifestyle
5-1. We recommend increasing physical activity and limiting sedentary time (nonacademic screen time, digital activities) to 1 to 2 hours per day for weight reduction. (strength of evidence, I; grade of recommendation, A)
5-2. We recommend maintaining adequate sleep duration for the prevention of obesity in children and adolescents. (strength of evidence, I; grade of recommendation, A)
5-3. We recommend a family-centered approach, including parents, to prevent and treat children’s obesity effectively; parental obesogenic lifestyle habits are related to children’s obesity. (strength of evidence, I; grade of recommendation, A)
5-4. We recommend the development of specific public health interventions as essential to overweight and obesity control in children with lower socioeconomic status (SES). (strength of evidence, I; grade of recommendation, A)
5-5. We recommend that obesity interventions be conducted in multiple key childhood environments, including family, school, and community. (strength of evidence, I; grade of recommendation, A)
5-1. We recommend increasing physical activity and limiting sedentary time (nonacademic screen time, digital activities) to 1 to 2 hours per day for weight reduction. (strength of evidence, I; grade of recommendation, A)
Obese children tend to commute to school by school bus rather than walk to school [84-86]. The sedentariness of obese children is higher than that in normally weighted children; the former have been shown to like to lie down when staying indoors and use the elevators more than stairs [84,87,88]. Obese children spend a high proportion of their day watching television or using the personal computer compared with normally weighted children [84,89-91]. Increased television-viewing time decreases physical activity, and can increase the consumption of high-calorie diet through being exposed to television commercials of high-calorie foods, such as fast food, snack, and soft drinks [84,92-96]. The effort to walk as much as possible and exercise regularly is significantly related to losing body weight [86].
5-2. We recommend maintaining adequate sleep duration for the prevention of obesity in children and adolescents. (strength of evidence, I; grade of recommendation, A)
A school-based, cross-sectional study of 3,785 Korean adolescents in middle and high school between the ages of 11 and 18 years showed the significant association of longer sleep duration on both week day and weekends with decreased BMI for both sexes [97]. A study using data of 489 adolescents aged 12 to 18 years from the Korean National Health and Nutrition Examination Survey from 2013 to 2014 showed that the risk of obesity decreases with increased sleep duration [98]. Researches in Canada, Japan, and China showed an inverse correlation between sleep duration and obesity in children [98-101].
Sleep restriction results in significant increases in caloric intake [102,103]. Short sleep is associated with decreased moderate to vigorous physical activity and increased sedentary time [102,104]. A significant negative association has been observed between sleep duration and screen time [102,105]. Short sleep is also associated with insulin resistance [102].
5-3. We recommend a family-centered approach, including parents, to prevent and treat children’s obesity effectively; parental obesogenic lifestyle habits are related to children’s obesity. (strength of evidence, I; grade of recommendation, A)
According to a meta-analysis conducted with studies published between 2000 and 2009, the majority of studies (70%) have shown statistically significant moderate to large effect size changes in child BMI after participation in a family-based intervention for weight loss. Of these, 50% reported statistically significant weight loss changes at 6-month, 1-year, and 2-year follow-up, albeit with small to moderate effect sizes [106].
In a study of Korean first-grade elementary school students and their parents, parental lifestyle habits were shown to induce children’s obesity [107]. Children of obese parents are more likely to be diagnosed as overweight compared with children of normal-weight parents. Among the paternal lifestyle habits, hours of watching television or computer usage, and consumption frequency of soda, ice cream, cake, and chips are related to the children being overweight. Among the maternal lifestyle habits, hours of watching television or computer usage, frequency of eating breakfast, and frequency of overeating are related to the children being overweight. Parents’ lifestyle habits can affect children’s weight via an effect on the children’s lifestyle habits. The degree of obesity between parents and children tends to be similar because parents and children share not only genes but also the same family environment. Family environment plays an important role in forming children’s lifestyle, including eating habits and physical activity through parents’ lifestyles. As the mother tends to take the main role in rearing children, maternal obesogenic lifestyles have greater influence on children’s obesity.
5-4. We recommend the development of specific public health interventions as essential for overweight and obesity control in children with lower SES. (strength of evidence, I; grade of recommendation, A)
According to a study based on data of the Korea National Health and Nutrition Examination Survey 2007–2010 conducted by the Korea Centers for Disease Control and Prevention, SES does not affect the observed relationships of overweight or obesity in children aged 2–18 years [108]. However, recent published systematic reviews and meta-analyses have showed that children with lower SES have higher risks of being diagnosed with overweight and obesity [109,110]. Another systematic review and meta-analysis of studies published between 1990 and 2014 showed that low SES is associated with a 10% higher risk of overweight and a 41% higher risk of obesity in children aged 0–15 years [109]. In a subgroup analysis, this relationship was prominent in high-income countries and in more economic developed areas, including North America, Europe, and Oceania [109]. Another systematic review to describe the relationship between SES and childhood/adolescent weight status in papers published in rich countries from 1990 through 2013 showed a predominantly inverse relationship [110].
Adolescents from areas with low SES more often skipped breakfast and more often ate snacks compared with adolescents from high SES areas [111,112]. SES has been positively associated with food frequency intake scores in both sexes. Adolescents with low SES tended to show an irregular meal pattern [31,33]. High household SES is also associated with increased intakes of vegetables, fruits, and dietary fiber, and with decreased intakes of fat [111,113,114].
A study on the association among parental socioeconomic level, overweight, and eating habits with diet quality in Korean sixth-grade school children showed that a lower SES (in terms of parental income or parental education level) relates to the consumption of significantly fewer fruits [111]. In the same study, the children in the lower socioeconomic group had a lower food habit score (high frequency of breakfast skipping and ramen noodle consumption), diet quality, and intake of nutrients compared with those in the higher socioeconomic group. Lower maternal education status is also associated with a higher risk for being overweight in girls. Specific public health interventions should support parents and children with lower SES to develop health-related behaviors that may prevent childhood obesity.
5-5. We recommend that obesity interventions be conducted in multiple key childhood environments, including the family, school, and community. (strength of evidence, I; grade of recommendation, A)
Most strategies for preventing or reducing childhood obesity have focused on individual behavior modification with limited success [115,116]. The environment of children with obesity, including family, schools, after-school programs, and community, as well as the policy level, can be changed to promote healthier lifestyles through multilevel obesity interventions [115,117]. The family represents the closest environment of children; thus, the family is important to forming the healthy lifestyle of children [115,107]. School is the place where students spend most of their time beginning with the time they reach schooling age [115,118]. Children can maintain and manage a healthy lifestyle through teacher–pupil interaction and peer interaction [115,118]. In the treatment or prevention of childhood obesity, a variety of support systems through parents, peers, and teacher relationships can induce changes in the overall environment surrounding children, thereby raising the effectiveness of any obesity intervention [115]. Multidisciplinary interventions can make obese children continue a healthy lifestyle [115]. Obesity in children and adolescents is linked to adult obesity and various diseases, leading to an increase in public medical expenses. Therefore, national policy is needed in leading efforts to preventing obesity fundamentally and to establishing education and policy for health promotion.
6. Behavioral intervention for children and adolescents with obesity: mental health
6-1. We recommend that obese children be monitored for psychological problems and screened for the need for psychiatric treatment. (strength of evidence, I; grade of recommendation, A).
6-2. We recommend that physicians emphasize family functioning and let the family participate in the treatment of the obese child. (strength of evidence, I; grade of recommendation, A).
6-3. We recommend cognitive behavioral therapy, which may be beneficial to treating child obesity. (strength of evidence, III; grade of recommendation, C)
6-1. We recommend that obese children be monitored for psychological problems and screened for the need for psychiatric treatment. (strength of evidence, I; grade of recommendation, A)
Obese children may be suffering from low self-esteem, body shape dissatisfaction, depression, eating disorder, obesity stigma, teasing, or bullying by peers [119-125]. They also live with significantly lower health-related quality of life compared with normal weighing children, or several pediatric chronic diseases [126]. Obese children complain of a low quality of life associated with physical and psychosocial health, and emotional, social, and school functioning [126,127].
Extremely obese adolescents have higher rates of mood, anxiety, somatoform, and eating disorders compared with a populationbased control group [128]. The screening tools for psychological problems include the Korean-Child Behavior Checklist, Children’s Depression Inventory, Korean version of the Eating Attitude Test-26, somatotype drawings, and Pediatric Quality of Life Inventory [121-123,126-127].
6-2. We recommend that physicians emphasize family functioning and let the family participate in the treatment of the obese child. (strength of evidence, I; grade of recommendation, A)
Poor family functioning is associated with increased risk of obesity and overweight [129,130]. The elements of poor family functioning related to obesity are poor communication, poor behavior control, high levels of family conflict, and low family hierarchy values [130]. Although standardized family functioning measures are necessary, half of the identified intervention studies reported a significant relationship between family functioning and changes in child weight [130]. Contrary to these reports, several studies have reported that family functioning is not associated with child obesity; rather, an overweight mother is largely linked to child obesity [131,132]. Given the high correlation of parental or mother’s obesity with child obesity, parental behavior changes in the family should be considered [132,133]. Family-based treatment is crucial to control nip successfully child obesity.
6-3. We suggest cognitive behavioral therapy, which might be beneficial to treating child obesity. (strength of evidence, III; grade of recommendation, C)
Cognitive behavioral therapy (CBT) is effective in treating childhood obesity [134-136]. The treatment goal is weight control by healthy changes in lifestyle rather than weight reduction. The key element of this therapy is self-regulation, with techniques including learning self-instructions (e.g., “stop and think”), self-observation, self-evaluation, and self-reward [136]. To train self-regulation skills, modeling (showing the coping skills to the child), behavior rehearsal, and homework have been used [136]. Coping skills are taught for different stressful situations (e.g., feeling alone) and relapse moments (e.g., feeling hungry) [134,135]. The progression of CBT is concentrated on one new small change in food and exercise behavior (e.g., drinking water instead of soft drinks, walking instead of taking the car) [135,136]. Self-monitoring—recording one’s behavior—is perhaps the most important component of behavioral treatment. Patients keep detailed records of their food intake, physical activity, and body weight, which they review with their interventionist to identify areas of success and for improvement [137].
Parents participate in CBT as helpers. For the stimulus control of the obese child, parents are taught the importance of ending restrictions on the places and times for eating. Motivation of the obese child is enhanced by allowing his or her own choices in planning the program and using a child-friendly approach with respect to developmental demands; for example, providing activities involving cooking, moving, and playing [134,135]. Braet et al. [135] reported that in the long-term follow-up over 4.6 years, 71.6% subjects treated with CBT showed no further increase in percentage overweight.
Negative body image is a major concern of overweight persons. CBT includes the information to change negative stereotypes of obesity, modification of intrusive thoughts of body dissatisfaction and overvalued beliefs regarding physical appearance, exposure to avoided body image situations, and elimination of body checking. CBT has significantly improved the body image, psychological symptoms, self-esteem, overeating, and guilt eating in obese subjects [138].
7. Pharmacotherapy of children and adolescents with obesity
7-1. We recommend that pharmacologic treatment is not used as a primary treatment nor sole therapy mode in pediatric obesity. (strength of evidence, I; grade of recommendation, A)
7-2. We recommend that the response and adverse reaction to pharmacologic treatment be monitored closely. The decision to continue or discontinue should be made by accounting for the monitoring result. (strength of evidence, V; grade of recommendation, A, based on committee voting)
7-1. We recommend that pharmacologic treatment not be used as a primary treatment nor lone therapy method in pediatric obesity. (strength of evidence, I; grade of recommendation, A)
Only a few studies have been conducted in pharmacologic treatment for childhood obesity. In a prepubertal age group (younger than 12 years old), the effectiveness and safety of pharmacologic treatment of obesity are low because of issues of appropriate dosage, safety, adverse event, and ethical aspects [139,140]. Research data on adolescents over the age of 12 years are not sufficiently accumulated as well. However, some weight loss effects could be expected [139-141]. Therefore, in case of primary treatment failure, an approved drug could be considered added, along with behavioral intervention.
Orlistat, metformin, glucagon-like peptide 1 (GLP-1) agonists, and topiramate are available in adult obesity, and there have been a considerable number of efforts to use these agents in childhood obesity [142-146]. Orlistat is the only drug that the FDA has approved for childhood obesity over the age of 12 years, but it is not recommended to use as a primary nor single therapy [141,147]. Data on the single drug use of orlistat without behavioral therapy are not available. In case of concerns on side effects, only behavioral therapy is recommended, instead of adding drugs.
1) Orlistat
Orlistat, a fat absorption inhibitor, is the only agent that the Korea Food and Drug Administration had approved for long-term use (one year) for weight control in pediatric obesity [148]. It is the only FDA-approved drug that can be prescribed 3 times a day for childhood obesity in children aged 12 to 16 years [142,147]. However, it is not recommended as a primary treatment for weight control in childhood obesity, especially between the ages of 2 and 11 years [140,149]. Orlistat inhibits lipid digestion by the suppression of pancreatic and gastric lipase. The decreased lipase activity in the gastrointestinal tract hinders consumed fat to be absorbed as a form of fatty acids and monoglycerols. Fat thus remains in the stool in triglyceride form [150]. A placebo controlled study of obese children aged 12 to 16 years showed a significant reduction in BMI compared with the controls, but also reported significant side effects. Another study among obese teenagers aged 14 to 18 years failed to show significant weight loss [151].
Orlistat should be taken with meals, which makes it difficult to prescribe to school-aged children. In some reports, orlistat interferes with the absorption of fat-soluble vitamins, such as vitamins E and D [141]. For many obesity-control drugs proven safe and effective for long-term use in adults, pediatric data are limited. Orlistat may cause adverse effects, such as steatorrhea, soiling, bloating, and increased number of bowel movement. Such adverse events have been reported in pediatric use. Younger patients are recommended to take multivitamins because orlistat can hinder the absorption of fat-soluble vitamins, such as vitamins A, K, and β-carotene. There have also been rare reports of hepatic and renal damage in adults, and of oxalate nephrolithiasis and oxalate nephropathy with renal failure [152].
2) Metformin
Metformin can be used safely in type 2 DM children over the age of 10 years and has been known to result in weight loss. It can be used at about 1,500 mg a day in children with type 2 DM between the ages of 12 to 14 years with BMI of 26–40 kg/m2 [153]. Although metformin can be used by type 2 DM children, it is not recommended as treatment for only obesity; indeed, it has not been FDA approved as an obesity treatment [154-156]. Metformin reduces hepatic glucose production, increases peripheral insulin sensitivity, and lowers appetite [157].
A study has shown BMI reduction after 6 to 12 months of use of metformin. A previous study reported that metformin has some effects in children with insulin resistance [158]. Although metformin could be used in the short term, along with behavioral therapy, it is not recommended as a single drug for obesity treatment because of the limited effect of weight control [159].
3) Liraglutide
Liraglutide is a GLP 1 analog that can be used for long-term treatment of adult obesity [159]. GLP-1 is the incretin hormone released by the ileal L-cells after food consumption, inducing satiety by delaying gastric emptying and glucagon secretion. It also controls appetite and satiety in the hypothalamus [141,149]. In adult type 2 DM, GLP-1 is an effective primary therapy for controlling hemoglobin A1c (HbA1c) and weight. For obesity in adolescents, a significant decrease in BMI has been observed after 3 months of use [11,142].
Liraglutide needs to be injected daily, which can be a limitation in pediatric application. Safety and pharmacokinetics have been tested in children with type 2 DM aged between 10 and 17 years: it has similar effects as in adults. However, about half of the subjects experienced at least one side effect [159]. Among GLP-1’s side effects are nausea, vomiting, diarrhea, and low blood glucoses. However, rare but serious side effects have also been reported, such as kidney failure, suicidal impulse, pancreatitis, and gallbladder disease [152]. Therefore, it is not recommended to use liraglutide for childhood obesity treatment.
4) Topiramate
Topiramate is a gamma-aminobutyric acid receptor antagonist that is known to be a treatment for epilepsy (for those aged 2 years and older) and migraine (for those aged 12 years and older). The weight loss effect of zonisamide (voltage-dependent sodium channels and T-type calcium blocker) was observed in the study of epilepsy, which might be related with the serotonin effect [141,152-153]. Despite the weight control effect of topiramate and zonisamide, the findings of epilepsy studies cannot be directly generalized into simple treatment for childhood obesity [149].
No proven safety or efficacy data are available with combined therapy of phentermine-topiramate in pediatric obesity [152]. The effect of zonisamide in pediatric obesity was reported in case reports of limited subjects [153]. Headache, nausea, vomiting, thirst, decreased appetite, abdominal pain, anxiety, speech disorders, attention and memory deficit, somnolence, and diarrhea have been associated with topiramate and zonisamide [143-144,146]. Serious side effects were reported in children using topiramate, such as glaucoma, stroke, metabolic acidosis, cognitive disorders, hyperammonianemia, encephalopathy, and kidney stone [152]. Therefore, it is not recommended to use topiramate for the treatment of childhood obesity.
7-2. We recommend that the response and adverse reaction of pharmacologic treatment be monitored closely. The decision to continue or discontinue treatment should be made with consideration for the monitoring result. (strength of evidence, V; grade of recommendation, A, based on committee voting)
Although cumulative data on the effectiveness of pharmacologic treatment of childhood obesity are insufficient, reports of adverse reactions related to those agents exist in many references, including adults’ studies [11,141,150,152,160]. Therefore, pharmacologic treatment of childhood obesity should be taken cautiously, and careful observation and evaluation of its adverse reactions and effects are essential.
8. Bariatric surgery for children and adolescents with obesity
8-1. We recommend that bariatric surgery be an appropriate option to improve health when adolescents with a BMI >40 kg/m2 or >35 kg/m2 and obesity-related comorbidities fail to respond to behavioral interventions (with or without pharmacotherapy) for sufficient weight loss to achieve targeted health outcome goals and when they attain Tanner IV or V pubertal development and final or near-final adult height. (strength of evidence, V; grade of recommendation, A, based on committee voting)
The timing for surgical treatment of extremely obese adolescents remains controversial and depends, in most cases, on the compelling health needs of the patient [82]. Physiologic maturation is generally complete by sexual maturation (Tanner) stage IV. Bariatric surgery is considered only under the following conditions: when the patient has attained Tanner IV or V pubertal development and final or nearfinal adult height, BMI >35 kg/m2 with major comorbidities (type 2 DM, moderate to severe sleep apnea of apnea-hypotonia index >15, pseudotumor cerebri, and severe nonalcoholic steatohepatitis) or BMI >40 kg/m2 with other comorbidities (hypertension, insulin resistance, glucose intolerance, dyslipidemia, sleep apnea with apnea-hypopnea index >5, and substantially impaired quality of life or activities of daily living). Skeletal maturation (adult stature) is normally attained by the age of 13 to 14 years in girls and 15 to 16 years in boys. If uncertainty exists on whether adult stature has been attained, skeletal maturation (bone age) can be objectively assessed with a radiograph of the hand and the wrist. From this view, bariatric surgery would not be recommended for prepubertal adolescents [161,162].
Adolescent psychological development also impacts the ability to participate in surgical decision-making and postoperative dietary compliance. Cognitive development refers to the development of the ability to think and reason [163].
Conclusion
This evidence-based clinical practice guideline on the diagnosis and treatment of pediatric obesity in children and adolescents in Korea was produced by all members of the Pediatric Obesity Committee of the KSPGHAN and experts from all related fields.
The most essential concept for the effective treatment of obesity in children and adolescents recommended in this guideline is a family-based, comprehensive, multidisciplinary behavioral intervention focused on lifestyle modification, including calorie-controlled balanced diet, active vigorous physical activity and exercise, and reduction of sedentary habits, and support by the entire family, school, and community. Evidence for the effectiveness and safety of most pharmacotherapy and bariatric surgery treatments remains limited in adolescents and insufficient in children.
For better outcomes, the prevention and treatment of obesity and obesity-related morbidity should be started from early in life to control and manage the risks for developing NAFLD, metabolic complications, and obesity-related physical and psychosocial comorbidities in childhood, and to reduce cardiovascular and metabolic morbidities and premature mortality later in adulthood as well. As the disease burden of obesity on the overall health status has become a key issue of health care system worldwide, including South Korea, this guideline would be beneficial not only in clinical practice but also in establishing health care policies.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


