

Introduction
Dapsone (4,4'-diaminodiphenylsulfone, DDS) is a potent antibiotic and anti-inflammatory agent that belongs to the sulfonamide drug class. It is primarily used in the management of leprosy, bullous dermatoses and other refractory inflammatory skin diseases. Drug-induced hypersensitivity syndrome (DIHS), also called drug rash with eosinophilia and systemic symptoms (DRESS), is a severe reaction to drugs, such as carbamazepine, phenytoin, phenobarbital, allopurinol, minocycline, sulfasalazine, and dapsone, mimicking severe sepsis or viral infection. DIHS is usually characterized by fever, rash, and multiorgan failure, occurring 1 to 8 weeks after drug introduction. It is thought to be an immune-mediated reaction involving macrophage and T-lymphocyte activation and cytokine release1). When features of DIHS have occurred clearly after dapsone medication, the term, 'dapsone hypersensitivity syndrome (DHS)' is commonly used.
To the best our knowledge, there are few reported cases of DHS with multiorgan dysfunction in Korean children2-4). Most of their symptoms resolved within 2 or 3 weeks of steroid treatment, however, one case progressed to coma on 6th hospital day (HD) and died a few days later2). An international review of 336 patients with DHS showed that, more than 70% of the patients were from Asia, and the prevalence rate and fatality rate of hypersensitivity reactions to dapsone were 1.4% and 9.9%, respectively5). We report a Korean boy who presented with DHS with a review of the literature.
Case report
An 11-year-old Korean boy presented with three days of pruritic erythematous rashes on both cheeks in a butterfly distribution, and circumoral pallor. The following day, he developed high fever with rice-grain-sized rashes that spread to the trunk. The patient's medical history revealed that he had been referred to a dermatological clinic at our hospital 2 months prior to presentation due to papular skin lesions on both forearms, elbows, and ankles that had appeared 4 months ago, and were refractory to conventional therapies. A diagnosis of linear IgA bullous dermatosis was made after biopsy, and he was started on dapsone at a dose of 50 mg per day for 4 days, then increased to 100 mg a day, methylprednisolone 8 mg once a day, and ranitidine 75 mg twice a day. A marked improvement of the skin lesions was noted after 6 weeks of treatment, which completed before he came to pediatric clinic with this new facial rash, and fever. Physical examination revealed a lethargic appearance with a temperature of 39.0Ōäā, heart rate of 82 beats/min, respiratory rate of 20 breaths/min, blood pressure of 120/80 mmHg, injected tonsils, hepatosplenomegaly, and bilateral enlargement of lymph nodes in the axillary and inguinal regions up to 3 cm in diameter. Given these findings, the patient was admitted to the pediatric ward with a working differential diagnosis of drug hypersensitivity versus autoimmune disease versus viral infection.
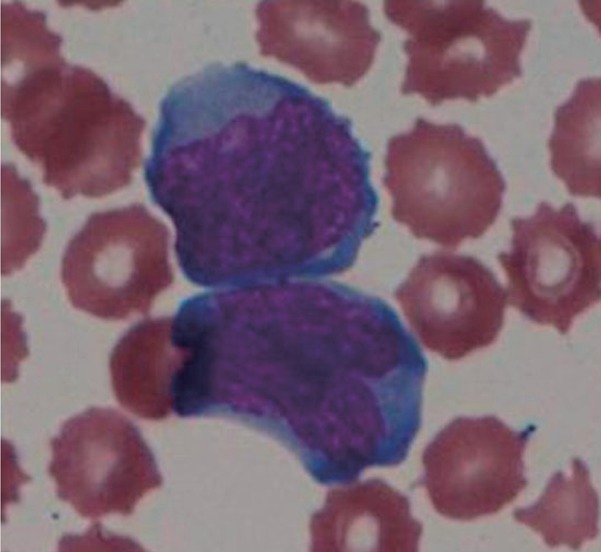
Initial blood count revealed a total leukocyte count of 600/mm3 (neutrophil 6%, lymphocyte 91%, eosinophil 0%), a hemoglobin of 11.8 g/dL, reticulocyte count of 3.4%, and platelet count of 180.000/mm3. The white blood cell count, checked 5 weeks prior to admission, was 4,000/mm3 with 46% neutrophils. Atypical lymphocytes were observed, and the differential count fluctuated between 4% and 29% during the first 2 weeks of hospitalization (Fig. 1). No eosinophilia was noted. A blood chemistry panel showed an aspartate aminotransferase of 107 IU/L, alanine aminotransferase of 101 IU/L, total bilirubin of 1.1 mg/dL, and a methemoglobin of 1.1%. Serologic tests for Epstein-Barr virus, cytomegalovirus, parvovirus, measles, antinuclear antibody, anti-ds DNA antibody, and lupus anticoagulant antibody were all negative. A polymerase chain reaction assay for 7 species of common respiratory viruses with nasal aspirates was positive for parainfluenza virus. Blood culture results on 1st HD were negative.
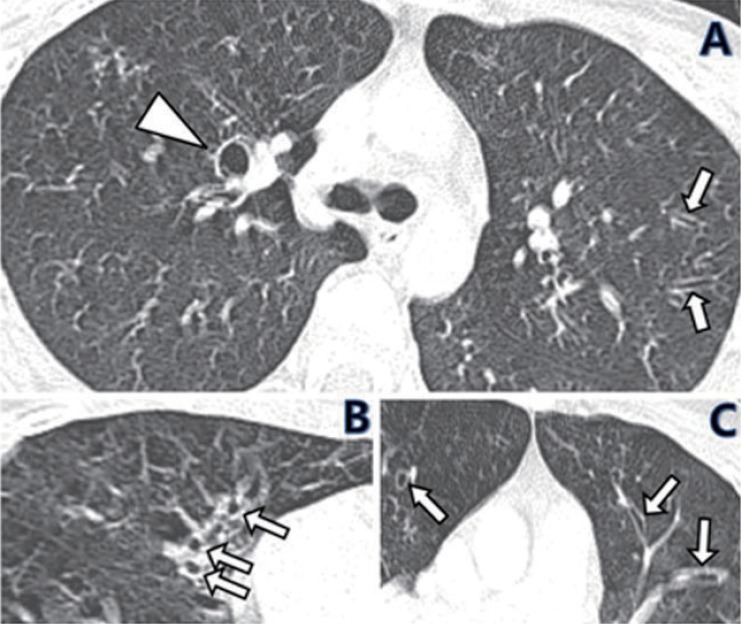
Dapsone was stopped immediately after the onset of fever. After admission, antihistamines, ibuprofen, prednisolone, ampicillin-sulbactam and intermittent dexamethasone injection were given. Prednisolone was administered at a dose of 1 mg/kg/day for 8 weeks. A subsequent study with ultrasound and computerized tomography (CT) of the abdomen revealed thickening of the gall bladder wall with some sludge, localized edema around the gall bladder, and moderate hepatosplenomegaly. Persistent fever, vomiting, dyspnea, and hypotension led to sequential blood cultures and ampicillin-sulbactam was replaced by meropenem from 8th HD. Culture results were positive for Klebsiella pneumoniae on the 8th HD, but negative on the 9th HD after introduction of meropenem for 1 day. Analysis of cerebrospinal fluid (CSF) on the 10th HD day showed a leukocyte count of 675 cells/mm3 (lymphocytes 100%), protein level of 136 mg/dL, and glucose level of 46 mg/dL. The CSF cultures for bacteria and fungi were negative. The patient's dyspnea and hypotension improved 2 days later and follow-up CSF study 5 days later showed a leukocyte count of 9 cells/mm3 (lymphocytes 62%, monocytes 38%), protein level of 33 mg/dL, and glucose level of 74 mg/dL. Sepsis, which appeared to be associated with Klebsiella pneumoniae, was followed by colitis, disseminated intravascular coagulation, syndrome of inappropriate antidiuretic hormone secretion, aseptic meningitis, pneumonia, pleural effusions, and peritonitis. Starting on 35th HD, he had renal failure for 10 days with fluctuating serum creatinine levels from 1.8 to 3.5 mg/dL. Chest CT, taken on 38th HD because of recurrent severe productive cough and rales, despite normal chest X-ray finding, showed tubular and cystic bronchiectatic changes (Fig. 2). Out of 19 blood cultures during the hospital stay, there was only one positive result for Klebsiella pneumoniae on 8th HD. The culture results were negative the following day with only three doses of meropenem. At that point, it is uncertain whether it is a rapid response to new antibiotics or contamination.
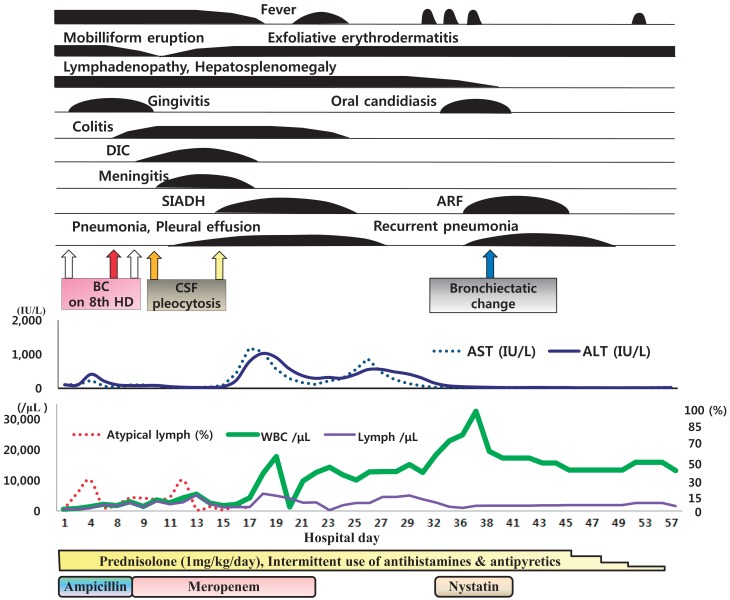
The maculopapular rashes initially developed on the face and trunk of the patient became confluent, spread to involve the entire body, and lately developed secondary desquamative changes in the 7th week of illness. With 2 months of supportive care, most of the patient's systemic symptoms resolved, with the exception of the skin scaling and generalized red tone or 'erythroderma' (Fig. 3), both of which slowly faded over the following 4 months. A severe neutropenia with absolute neutrophil counts ranged from 0 to 36/mm3 that lasted the first 2 weeks of hospitalization. It was slowly replaced by moderate neutrophilic leukocytosis after administration of prednisolone. All of the clinical events that occurred to the patient during the admission period are shown in the diagram (Fig. 4)
Discussion
By definition, sulfonamides are compounds that contain a sulfamoyl group (-SO2NH2). They were first synthesized as dyes derived from coal tar for the fabric industry in the early 20th century6). Dapsone is the structurally the simplest of all the sulfones. It was mainly used as a first-line treatment for leprosy7,8), and has also been used for a number of other dermatologic diseases, including Hailey-Hailey disease, bullous pemphigoid, acne, linear IgA dermatosis, urticarial vasculitis, and leukocytoclastic vasculitis9,10).
Orally administered dapsone is absorbed readily from the gastrointestinal tract with an estimated bioavailability of greater than 86%. After absorption via the gastrointestinal tract, dapsone is transported to the liver by portal circulation, where it is metabolized via either acetylation or N-hydroxylation7). Dapsone N-hydroxylation is mediated primarily by human liver microsomal enzymes P450 3A4, 2C6, and 2C1111,12). This pathway is thought to represent the initial step in the formation of toxic intermediate metabolites. While sulfonamide-induced hypersensitivity syndrome typically appears 10 or more days after exposure13), dapsone-induced disease usually develops more than 4 weeks after starting the medication11). Additionally, the data suggest that dapsone-induced hypersensitivity syndrome carries a higher risk of hepatic involvement11,14). Our patient developed DHS six weeks after drug introduction.
The precise pathogenetic mechanism of adverse drug reactions is unclear. However, delayed hypersensitivity directed by drug-specific T cells seems to be involved, since widespread skin lesions, generalized lymphadenopathy, hepatitis, and sometimes nephritis or pneumonitis develop 2 to 8 weeks after administration of the offending drugs, and these clinical features last even after withdrawal of the drugs. Visible atypical lymphocytes in peripheral blood as in our case support this hypothesis.
Another common side effect of dapsone therapy is dose dependent hematologic problems, including methemoglobinemia and hemolytic anemia, both of which result primarily from hydroxylamine and other hydroxylated metabolites acting as potent oxidants15). Those findings were not observed in our case. Other rare, serious, and unpredictable hematologic side effects associated with dapsone include agranulocytosis11). Prolonged agranulocytosis increases a person's risk for infections and sepsis. However, one cannot conclude that the sepsis in the case was caused solely by an infection.
The pathogenesis of meningitis and bronchiectatic changes in this case was one of the major questions. It is possible that the patient had partially treated bacterial meningitis (PTBM) since 3 doses of intravenous meropenem was given before the CSF cultures became negative. However, drug induced aseptic meningitis (DIAM) due to dapsone, or even to amoxicillin or ibuprofen, other possible scenarios in this case, cannot be excluded on the basis of the CSF profiles. Although there is no report that DIAM is related to dapsone, DIAM due to trimethoprim-sulfamethoxazole or ibuprofen16-19) is well-known. CSF findings alone, however, cannot discriminate DIAM from other disease, such as PTBM or viral meningitis17-19). Reports of DIAM following ingestion of drugs in patients with diverse autoimmune disease18), or a report of high CSF protein level of 312 mg/dL in a patient with DIAM19) provide us meaningful reference. The bronchiectatic changes with uncommon cystic dilatation, which were first noted on 38th HD, are another intriguing point. The term, bronchiectatic change, was used instead of bronchiectasia since follow-up study was not made. Dapsone is known to induce pneumonitis20), but we failed to find a report indicating a relationship between dapsone and bronchiectasis or bronchiectatic changes. While it seems to be safe to attribute the causes of the patient's meningitis and bronchiectatic changes to infections, or, at least, interplay between infection and a drug reaction, it is very challenging to attribute the causes primarily to the drug reaction.
Systemic steroids are known to be effective in treating DHS. In the case presented here, prednisolone was used at a dose of 1 mg/kg/day for 8 weeks. DIHS is usually treated with oral corticosteroids in dose of 1-1.5 mg/kg/day. It needs to be determined whether higher steroid doses can produce better results. Notably, the steroid dose should not be tapered too early, as dapsone toxic metabolites can persist in organs for up to 35 days via protein binding and the enterohepatic circulation11), and worsening of dermatitis and hepatitis can occur as a rebound phenomenon15). After 2 months of hospital treatment, most of the systemic symptoms were resolved, with the exception of the skin scaling and erythema which faded over the following 4 months.
Although, DHS is rarely encountered in the field of pediatrics, clinicians need to familiarize themselves with the prominent features of DHS which may be prototypical of all DIHS. In our case, agranulocytosis, atypical lymphocytosis, sepsis, aseptic meningitis, bronchiectatic changes, and prolonged course are some of the most peculiar findings that can differentiate this case from others.

 PDF Links
PDF Links PubReader
PubReader PubMed
PubMed Download Citation
Download Citation


