

Introduction
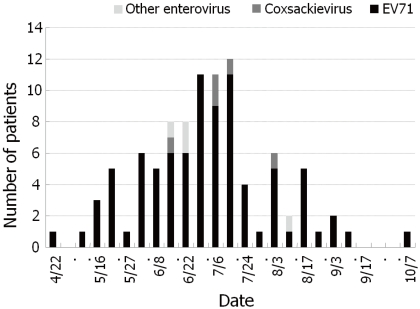
On April 18 2009, a 21-month-old girl was referred to the pediatric emergency room of the Ewha Womans University Mokdong Hospital. She had progressive weakness of the lower limb, which had begun 3 days earlier. She was treated at the local hospital with the hand-foot-mouth disease (HFMD). Her consciousness was clear. She did not have any rash on the skin and showed asymmetric lower leg weakness with more severity on left leg. She was immunized with 3 doses of inactivated polio vaccine. On CSF examination, pleocytosis was noted, but chemistry profiles were normal. Because of her acute asymmetric flaccid paralysis of lower limb, her stool was sent to the Division of Enteric and Hepatitis Viruses, National Institute of Health, Korea Centers for Disease Control and Prevention under the impression of poliomyelitis-like paralysis due to enterovirus 71 (EV71). On her stool examination, EV71 with C1 type was discovered. She was the first confirmed case of enterovirus 71 infection on 2009 epidemics in Korea1). In the spring of 2009, a large nationwide outbreak of HFMD caused by HEV71 occurred in Korea (Fig. 1). Most of the cases were in children <6 years of age and one case was fatal. EV71 became an emerging concern in Korea. The purpose of this review is to overview the recent outbreaks of EV71 infection in Korea with exploring epidemiology, virology, clinical manifestations and management.
Virus and genotypes
The genus Enteroviruses are nonenveloped, single-stranded, positive-sense viruses in the Picornaviridae ("small RNA virus") family. The human enteroviruses were originally classified echoviruses, coxsackieviruses, polioviruses by their replication patterns in tissue culture and animals. Recently they have been reclassified based on molecular properties into 5 species, polioviruses, human enterovirus A, human enterovirus B, human enterovirus C, and human enterovirus D. EV71 discovered in California in 19692) belongs to the human enterovirus A3).
In recent epidemics in the Asia-Pacific region, the predominant EV71 genotypes were various. In Sarawak during 1997 and Singapore during 1998, genotype B3 was most prevalent. EV71 isolated from patients in the Taiwanese epidemic during 1998 belonged to genotype C24, 5). During the epidemics in Malaysia and Singapore in 2000, the predominant genotype was B45). And, the EV71 outbreaks in Brunei, Sarawak and Singapore in 2006 were caused by subgenogroup B5 virus6). EV71 in the outbreak in China during 2007-2008 belonged to subgenotype C4a7, 8). The increasing fatality of EV71 infection in recent epidemics has been thought to be due to both endemic and epidemic circulation of the virus and its evolution. The possible occurrence of inter-typic recombination of EV71 may play important roles in the emergence of various EV71 subgenotypes with varied virulence and clinical manifestations9).
Since 2000, the laboratory surveillance system for early detection of EV71 has been operating in Korea. On 2000, EV71 were isolated for the first time from 12 patients with HFMD in Korea. They belonged to genotype C3, which has been identified rarely in other epidemics in recent years4, 10). During outbreaks in China in 2008-2009, the most frequent genotype among the EV71 strains isolated from patients was C4a. Genotype C1 viruses were isolated from cases of uncomplicated HFMD in Singapore and Sarawak during 1998 and in Sarawak and Western Australia during 2005,11). It does not appear that a single neurovirulent genotype is associated with the severe and fatal cases12). Further study is needed to elucidate the factors influencing the virulence of EV71.
Epidemiology
EV71 infection has the seasonal distribution of a peak in the spring and summer months. The transmission of enterovirus occurs within families, daycare centers, playgrounds and hospital nurseries. More children would be congregating in a limited space, which provides a readily available reservoir for the rapid circulation of the virus13). The fecal-to-oral route is considered a major transmission route. Long periods of viral shedding may account for the widespread transmission of EV7114). Chung et al15) demonstrated that EV71 is excreted through the stool of infected patients for up to 6 weeks. Chang et al16) presented that the culture-positive rate of throat swabs was higher than that of rectal swabs in the patients. Viruses in throat through the saliva or respiratory droplets of patients may be transmitted during the acute stage of the disease17). Although hand-washing precaution is important for the period of virus excretion through feces, it is not sufficient to limit the spread and transmission of the virus and to prevent further epidemics. Therefore, isolation of infected patients within single rooms with masks should be considered during hospitalization of patients14).
It is not clear why a certain region has experienced an increased incidence of EV71 infection. A change in clinical presentation could coincide with a change in the viral transmission pathway. An epidemiological parameters like crowding, lack of sanitation, and climate, could enhance virus transmission. An increased susceptibility of the population to EV71 infection could be another explanation.
Pathogenesis
Infants and young children are very susceptible to EV71 infection. Immature immunity is therefore suspected to associate with increased morbidity and mortality. Moreover individual host genetic factors may affect clinical severity
Lymphopenia, depletion of CD4 and CD8 T lymphocytes, and decreased cellular immunity in the peripheral blood were noted in patients with brain stem encephalitis and pulmonary edema18).
However, some clinical studies showed that elevated cellular immunity was linked with unfavorable outcomes19). The clinical manifestations are reflecting the contribution of immunopathological process in addition to cytopathic damage to neuronal cells12, 20, 21). Cytokines in the central nervous system and systemic inflammatory responses play important roles in the pathogenesis of EV71-associated encephalomyelitis. Destruction of vasomotor in the brainstem by EV71 produces autonomic nervous system dysregulation prior to the pulmonary edema. The pulmonary edema is the result of increased pulmonary vascular permeability caused by the direct brainstem lesions and/or a systemic inflammatory response syndrome produced by the release of cytokines and chemokines.
Clinical Manifestations
Enterovirus serotypes are distinguished by antigenic and genetic sequence differences. Although no enterovirus disease is uniquely associated with any specific serotype, certain manifestations are preferentially associated with specific serotypes.
About half of EV71 infections are asymptomatic22). Most symptomatic EV71 infections commonly result in HFMD or herpangina. EV71 infections can cause pharyngitis, herpangina, stomatitis, gastrointestinal complaints, pericarditis, ventricular dysfunction, macular, maculopapular, vesicular or exanthema22). These clinical manifestations can be associated with neurologic syndromes frequently. Children having only febrile illness without mucocutaneous manifestations may have neurologic complications23). HEV71 is closely related to coxsackie virus A16 (CA16), the other major causative agent of HFMD, but unlike CA16, HEV71 is also associated with cases of acute neurologic disease including poliomyelitis-like paralysis, encephalitis, and aseptic meningitis.
Neurologic syndromes observed in EV71 include meningitis, meningoencephalomyelitis, poliomyelitis-like paralytic disease, Guillain-Barr├® syndrome, transverse myelitis, cerebellar ataxia, opsoclonus-myoclonus syndrome, benign intracranial hypertension, and brainstem encephalitis3, 12) (Table 1).
Neurologic disorders have been prominent in recent epidemics of EV71 disease. In the outbreaks in Taiwan in 1998 and in Australia in 1999, virological studies found that HFMD and herpangina epidemics were caused by EV71 and coxsackievirus A16 but the cases presenting with acute pulmonary edema and other neurological diseases were caused by brainstem encephalitis resulting from acute EV71 infection16, 24, 25).
HFMD with EV71-associated neurological syndrome has increased continually in many countries during the last 10 years, especially in the Asia-Pacific region8, 26). In some countries, outbreaks occur in a cyclical pattern every three years, predominantly caused by strains that are distinct from previous outbreaks27). In Singapore, since the first outbreak of HFMD in 1970, many epidemics have occurred by predominantly circulating strain coxsackievirus A16 or EV71, and the largest one was caused by EV71 with 3,790 cases and four deaths in 200013, 28). In 2006, Brunei reported that 1,681 children were affected with three deaths resulting from severe neurologic disease6). In the same year, an outbreak of EV71 affected approximately 14,400 children in Sarawak, Malaysia29). In the outbreak of China in 2008, a total of 488,955 HFMD cases were reported including 126 fatal cases, mostly caused by EV717). Possible reasons suggested for the outbreaks were mutation of the virus with increased virulence and the presence of host factors including the accumulation of susceptible populations and individual genetic susceptibility30, 31).
Ooi et al32) studied about the clinical risk factors to help detect children at risk of neurological involvement. They noticed that total duration of fever >or= 3 days, peak temperature >or= 38.5Ōäā and history of lethargy were independent risk factors for neurological involvement.
Mortality was high in EV71 brainstem encephalitis complicated with pulmonary edema, particularly in children below 5 years of age. There have been several large epidemics of EV71 infection causing high fatalities. The first report of severe epidemics of encephalitis and acute flaccid paralysis due to EV71 came from Bulgaria in 1975, in which 44 deaths occurred33). In 1978, 45 patients died of neurologic diseases with HFMD in Hungary34). Since 1997, three major epidemics have occurred in the Asia-Pacific region. They were in Sarawak, Malaysia in 1997, Taiwan in 1998, and China in 2008, and 31, 78, and 126 fatal cases were reported, respectively7, 24, 35).
In Korea, EV71 were isolated for the first time from 12 patients with hand foot mouth disease on 2000 laboratory surveillance. During 2009 outbreaks in Korea, about 90% isolates were from patients with HFMD and 10% from those with herpangina. Most patients with EV71 who presented neurologic symptoms were associated with HFMD. They were diagnosed as meningitis or meningoencephalitis, and Guillain-Barr├® syndrome, poliomyelitis-like paralytic disease and myoclonus. Gene analysis showed that most of them were caused by EV71 subgenotype C4a, which was prevalent in China in 2008. EV71 infections with severe cases with complications including death become a public health issue1).
During 2009 outbreaks in Korea, 16 patients were hospitalized with neurologic manifestations related with HFMD at Ewha Womans University Mokdong Hospital (Table 2). Their ages ranged from a month to eight years and the mean age was 29 months. The male to female ratio was 1.7:1 (M:F). Fever resolved in 2 to 7 days (mean, 4.5 days) and the range of peak of fever was 38.0 to 40.1Ōäā (mean, 39.3Ōäā). In most of the patients, neurologic symptoms developed between day 2 and day 3 (range, day 1 to day 5) after the onset of fever or skin lesions. Among the 16 patients, the most frequent neurologic manifestation was meningitis (62.5%), which included 8 definite cases with meningeal irritative symptoms and signs with CSF pleocytosis (>5 cells/mm3) and 2 suspected cases in whom spinal tappings were not performed. Three cases had Guillain-Barr├® syndrome and one of them had meningoencephalitis. One patient presenting asymmetric lower limb weakness (left>right) after HFMD showed enhancement in the left anterior horn of the spinal cord (T11 level) on magnetic resonance image. EV71 were detected in the 16 patients presenting neurologic manifestations by realtime PCR. Clinical samples included stools, respiratory secretion, or cerebrospinal fluid obtained from the patients, but viruses were detected from only stools. Subgenotypes of enteroviruses were C1 in the poliomyelitis-like paralytic disease patients, and C4a in eleven patients presenting Guillain-Barr├® syndrome, meningitis or myoclonus. Among the patients, only one girl presenting poliomyelitis-like paralytic disease still had limping when she was running at three months after discharge, but no death or severe complication with serious disease was observed in any of the other patients1).
Diagnosis
For virus isolation and detection, proper selection and handling of specimens are most important. Collection of materials from multiple sites is important. Specimen should be collected form nasopharynx, throat, stool, blood, urine, CSF, and other body fluids. Swabs from throat or rectum should be placed in a carrying medium. Fluid specimens should be collected sterile vials. In general, specimen should be refrigerated immediately after collection and during transportation to the laboratory. If an extended period will elapse before examination in the laboratory, shipping and storing it frozen are advisable.
During 2009 outbreaks in Korea, examinations for the viruses were carried out at the Division of Enteric and Hepatitis Viruses, Korea Centers of Diseases Control and Prevention. EV71 was isolated from specimens by real time-PCR. Viral RNA was extracted using ZR Viral RNA Kit (Zymo Research, Orange, CA, USA) according to the manufacturer's instructions. The whole genomic RNA was reverse transcribed for cDNA synthesis. Amplicons of the VP1 genes were generated by using primers as follows: forward primer, SO224 (5'-GCIATGYTIGGIACICAYRT-3'), and reverse primer, SO222 (5'-CICCIGGIGGIAYRWACAT-3') (1st-PCR); forward primer, AN89 (5'-CCAGCACTGACAGCAGYNGARAYNGG-3'), and reverse primer, AN88 (5'-TACTGGACCACCTGGNGGNAYRWACAT-3') (2nd-PCR). These PCR products were then sequenced using ABI PRISM dye terminator cycle sequencing ready reaction kit (Perkin Elmer, Waltham, Massachusetts, USA), and run on an ABI 3100 sequencer (Applied Biosystems, Foster City, CA, USA). Nucleotide sequences were determined by the DNASTAR1).
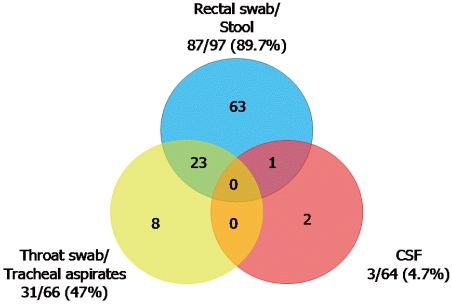
The virus was detected from rectal swab, stool, throat, tracheal aspirates and CSF specimens with various detectable rates (Fig. 2).
Treatment
The mainstay of treatment for EV71 disease is supportive management. There is currently no specific antiviral agent to treat or vaccine to prevent EV71 diseases.
All patients who demonstrate the neurological symptoms and signs should be hospitalized. If the patient has been diagnosed with uncomplicated brainstem encephalitis, close monitoring of the myoclonic jerks and vital signs is mandatory. Since the target central neurologic system is the brainstem, rather than the cerebrum, increased intracranial pressure is rarely encountered and the administration of osmotic diuretics is usually unnecessary36).
Treating severe EV71 brainstem encephalitis patients with intravenous immunoglobulin is associated with significantly decreased mortality by attenuated sympathetic activity and cytokine (IL-6 and IL-8) production. Furthermore, patients presenting with acute flaccid paralysis combined with pleocytosis in the CSF should also receive IVIG infusion. A specific recommendation dose is unknown. Experts recommend that IVIG 1 g/kg should be initiated for the first day, and if ANS dsyregulation does not improve, a second dose should be administered the following day37). The antiviral drug pleconaril offers promise for the treatment of enteroviral infection. It prevents the virus from attachment to cellular receptors and the uncoating and subsequent release of viral RNA into the host cell. Pleconaril is not available in Korea.
Infection control and prevention
As it has been reported that some serious cases causing death or severe neurologic complications were associated with the EV71 infection in 2009, EV71 infection has become an important issue in public health in Korea.
Public health measures, in particular, personal and environmental hygiene must target daycare centers, kindergartens, and schools where highly susceptible children congregate. In Singapore, to stem the spread of infection, preschools where transmission persisted for more than 2 incubation periods have been recommended to close, and trigger criteria for voluntary closure were instituted in April 2008. During closure, operators are to clean the centers thoroughly before they are allowed to reopen. In addition, parents are advised to ensure that their children adopt high-standard personal hygiene and to keep infected children at home until full recovery13).
In June 2009, Korea added HFMD and enterovirus infection to its list of nationally notifiable infectious diseases, for which all diagnosed cases must be reported within 7 days. This is expected to allow a more accurate and extensive survey of enterovirus infections nationwide and to lead to continuous collection of data about the incidence of EV71 infection and circulating viruses in Korea.
Prospects
Although HFMD is usually a benign disease, severe neurologic and cardiopulmonary complications can be developed in cases caused by EV71. In the Korean epidemic in 2009, these complications including death were reported. Because the outbreaks occur in a cyclical pattern, we need to establish a surveillance system to predict upcoming outbreaks and to develop adequate public health measures to control the outbreaks.
There are many aspects to be clarified for EV71 infections and controls such as understanding molecular genetics of EV71 virulence, identification of the receptor(s) for EV71, development of antiviral agents to ameliorate neurological disease and development of vaccine to prevent infection.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


