




Kawasaki disease is an acute systemic vasculitis in children with a predilection for the coronary artery. Inflammation of the coronary arteries destroys the arterial wall and causes aneurysm formation. The outcomes of damaged coronary arteries depend on lesion severity. Mildly dilated and inflamed arteries may resolve spontaneously. However, large aneurysms cannot be resolved [1].
Coronary vasculopathy in Kawasaki disease is characterized by 3 linked processes: necrotizing arteritis, subacute/chronic vasculitis, and luminal myofibroblastic proliferation. Myocardial infarction can occur throughout the course of vasculopathy [1]. Therefore, echocardiographic evaluation of the coronary artery is crucial for the diagnosis, treatment, and long-term management of Kawasaki disease.
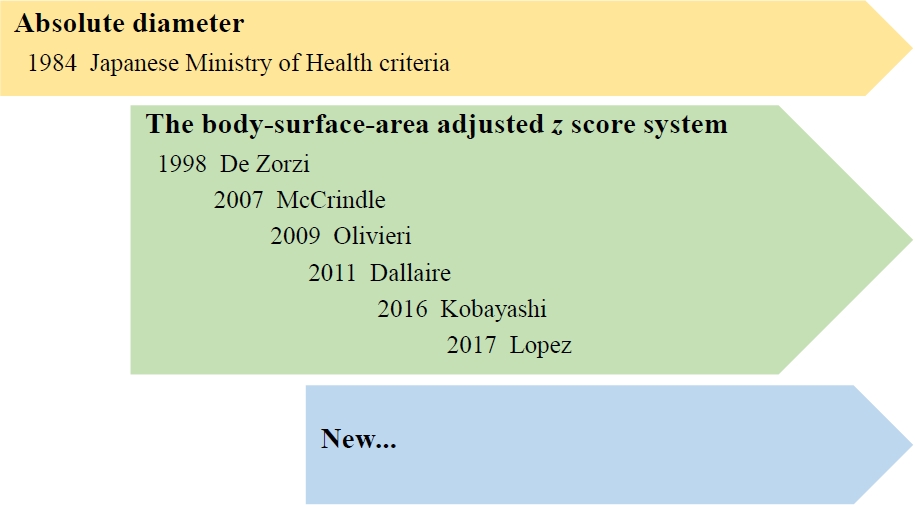
The diagnosis of coronary artery abnormalities has historically been based on absolute internal lumen diameter by the 1984 Japanese Ministry of Health criteria, which did not consider patient body size.
Considering that Kawasaki disease affects children with various body sizes, coronary artery diameter requires normalization to the body surface area (BSA) as a z score, standard deviation units from the mean. Several BSA-adjusted z score formulas for the coronary arteries have been established using various methods (Fig. 1) [2-7].
Since the 2004 American Heart Association guideline incorporated coronary artery z scores instead of previous absolute diameter, recently revised guidelines have updated and accepted the BSA-adjusted z score system to identify coronary artery abnormalities.
In the revised 2017 American Heart Association, 2019 European, 2020 Japanese Circulatory Society guidelines, coronary artery abnormalities are important criteria in the diagnosis of Kawasaki disease, and the BSA-adjusted z score systems have been accepted to define coronary artery abnormalities and classify coronary artery aneurysms [1,8,9]. Notably, when using z scores, a small error in the measurement of the coronary artery diameter can translate into a larger difference in z scores, which may change the patient’s risk classification [1]. Thromboprophylaxis and follow-up plans are recommended according to the risk classification of coronary artery abnormalities based on the z score system. In a recent article, the author reviewed recent guidelines for the diagnosis of coronary artery abnormalities in Kawasaki disease and the adaptation of various z score systems [10].
Z scores can be computed using several methods. Based on the data gathered from healthy children, various z score systems are available on the referenced website. The classification of coronary artery aneurysms using the z score system correlates well with clinical outcomes. Each z score formula yields slightly different results that could influence the diagnosis of coronary artery abnormalities, and the discrepancy of calculated Z scores is greater in cases of larger coronary aneurysm dimensions [10]. This discrepancy may have various reasons. These BSA-adjusted z score systems used different BSA equations derived from other normal population sizes and differences in sex and race. Regression methods also differed according to the z score system.
The echocardiographic evaluation of patients with suspected Kawasaki disease should focus on imaging the left main coronary artery, left anterior descending (LAD), left circumflex (LCX), right coronary artery (proximal, middle, and distal segments), and posterior descending coronary arteries. Normalization of luminal dimensions for BSA as z scores was used to define coronary abnormalities. The z score formula of LAD by Lopez produced the highest z scores among McCrindle, Olivieri, Dallaire, and Kobayashi [10]. The z score calculation for the LCX is only available in the formulas of Dallaire and Kobayashi [5,6]. Because the z score system is strongly related to risk stratification; each z score formula yields different results that could influence the diagnosis of coronary artery abnormalities, so the z score formula should be selected carefully and consistently.
Until now, no coronary artery z score formula has been derived from a large Korean population despite research for its development being conducted for several years.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


