




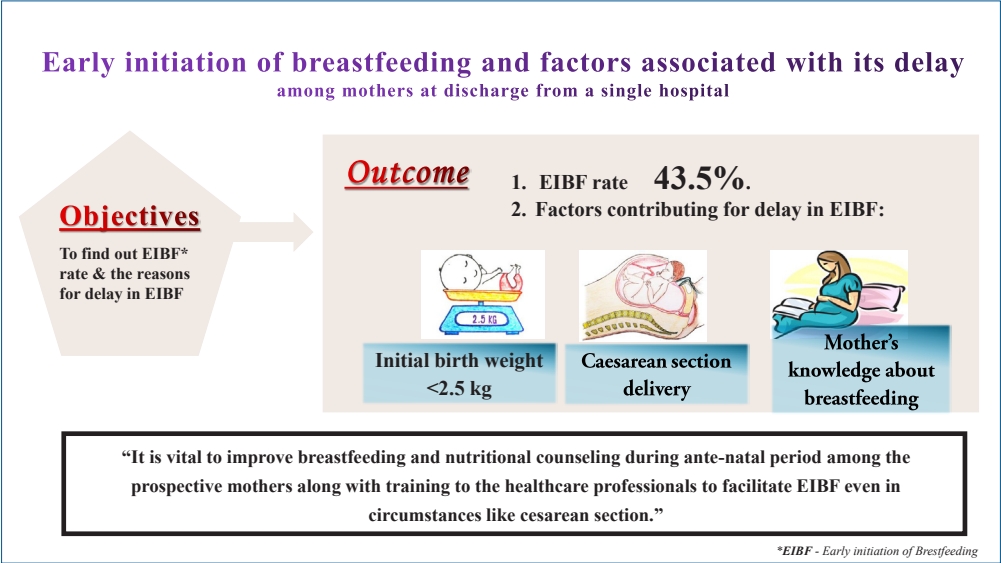
Graphical abstract
Introduction
Early initiation of breastfeeding (EIBF) is defined as ŌĆśprovision of mothersŌĆÖ breast milk to infants within the first hour of birth and ensures that the newborn receives colostrum[1]. EIBF is crucial as it ensures that the baby receives a colostrum, a yellow liquid contains crucial nutrients and antibodies to newborn acts as a first feed and first immunization [1]. EIBF provides a unique opportunity for the infants to obtain balanced nutrition and energy required for their growth and development at the earliest. Similarly, it creates the bonding between the infant and the mother, which enhances the cognitive development. It also reduces the risk of developing noncommunicable disease and obesity in prime of life [1,2].
Not only that, EIBF also protects the infants during their critical window period from diseases like diarrhea, neonatal sepsis, and pneumonia and at the same time improves maternal-infant bonding [2-4]. It is evident from the previous studies that EIBF not only plays a crucial role in reducing neonatal mortality and also increases the chances of continuing exclusive breastfeeding at later months [3,4].
It is expected that delivery conducted in a health institution escalates the chances that a newborn will be initiated on early breastfeeding [2,5,6]. But unexpectedly, though 7.9% of the babies were institutionally delivered in India, only 42.6% of them were breastfed within one hour of birth [7]. Subsequently, various maternal and facility-level factors have proven to have impact on EIBF [6,8]. Our hospital is planning to move towards the baby-friendly hospital initiative (BFHI) policy, in which one of the key components is ŌĆ£to facilitate immediate and uninterrupted skin-to-skin contact and support mothers to initiate breastfeeding as soon as possible after birth.ŌĆØ [9] Identifying these factors and intervening at an early stage will help to accentuate EIBF at the facility level [5]. Hence, the current study was planned with the following objectives: (1) to estimate the proportion of EIBF among postnatal mothers at the point of discharge in a tertiary care hospital in Puducherry and (2) to find out the determinants of delayed initiation of breastfeeding among postnatal mothers.
Methods
1. Study methods
The study was conducted in the postnatal ward by the Department of Community Medicine in collaboration with the Paediatrics Department in a tertiary care teaching hospital in Puducherry, India. This tertiary care institute is equipped with state-of-the-art equipment conducive to proficient stalwarts in conducting normal vaginal delivery and cesarean sections, followed by unmitigated postnatal care for both the mother and the newborn. The annual breastfeeding week celebration is organized by both departments, which has a beneficial response in elevating the breastfeeding habits in this hospital. It was a hospital-based analytical cross-sectional study. Data collection was done for 3 months. All postnatal mothers who delivered in the hospital (vaginal & cesarean delivery) during the study period were included in the study. Considering the prevalence of EIBF to be 14% [10] with 6.5% absolute precision and 10% nonresponse rate, the sample size was 108 (calculated using OpenEpi software ver. 3.01; Open Source Epidemiologic Statistics for Public Health). Consecutive sampling technique was used to include all the postnatal mothers for the study until the desired sample size was achieved.
2. Data collection procedure
After obtaining informed consent, data were collected using a pretested structured questionnaire. The questionnaire included demographic details, baby details, obstetric history, breastfeeding history, infant feeding practices, and rooming-in. Besides, open-ended questions were used to find out the reasons for delayed initiation of breastfeeding and rooming-in. A trained Community Medicine postgraduate paid visit to the postnatal mothers in the ward and conducted a face-to-face interview on the day before discharge. Confidentiality, anonymity, and privacy of the participants were guaranteed throughout the study.
3. Data analysis
The collected data were entered in Epi_Info (ver. 7.2.2.6; Centers for Disease Control and Prevention, Atlanta, GA, USA, and World Health Organization) software and analysed using IBM SPSS Statistics ver. 24.0 (IBM Co., Armonk, NY, USA). Bivariate and multivariate analyses were done to find out the determinants of delay in EIBF. In the first stage, an association between the delayed initiation of breastfeeding (dependent variable) and 15 independent variables such as baby age, babyŌĆÖs sex, birth weight of the baby, motherŌĆÖs age, area of the respondent, motherŌĆÖs occupation, motherŌĆÖs education, family type, socioeconomic status, religion, birth order, delivery type, prelacteal feeds, rooming-in and breastfeeding knowledge in mothers were done using bivariate analysis. In the next stage, 11 variables, (4 variables with higher odds ratio and 7 significant variables) obtained from bivariate analysis were included for multivariate logistic regression. The level of significance was set at 5% (P<0.05). The multiple coefficient of determinance (R2) was used as a goodness-of-fit statistic for the model.
4. Ethical consideration
Ethical clearance was obtained from the Institutional Ethics Committee (IEC) of Sri Mankula Vinayagar Medical College and Hospital, Puducherry (IEC Code no: 37/2019).
5. Guidelines used for reporting the study
To ensure the present hospital-based cross-sectional studyŌĆÖs systemic reporting, STROBE (Strengthening The Reporting of an OBservational study in Epidemiology) guideline was followed [11].
Results
The sociodemographic details of the baby and the mothers were given in Table 1. The mean┬▒standard deviation age of the postnatal mothers was 26.16┬▒4.22 years.
1. Breastfeeding and related practices
The median breastfeeding initiation time was 90 minutes (interquartile range [IQR], 30ŌĆō180 minutes) among the participants. Out of 108 respondents, about 47 mothers (43.5%) initiated breastfeeding within one hour of the delivery (vaginal and cesarean delivery). Nearly 107 of infants (99.1%) were breastfed. Of the infants, 84 (77.4%) were exclusively breast milk-fed (breast milk+expressed breast milk), and more than half 73 (67.6%) were exclusively breastfed by natural mothers from the day of birth until discharge. Only 1 of infants (0.9%) received bottled feed as the mother was on antiarrhythmia drug. Of 108 mother-baby pairs, only 47 (43.5%) practiced rooming-in, and the reasons stated for low rooming-in practice were cesarean section and the requirement of neonatal intensive care unit (NICU) admission for babies for their medical illness.
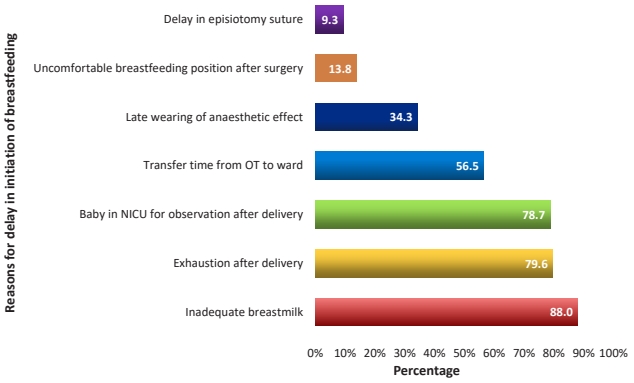
2. Reasons for delayed initiation of breastfeeding
Among 61 mothers who delayed initiation of breastfeeding, majority of them 95 (88.0%) stated that inadequate breast milk was the reasons for the delay. Other reasons stated by the mothers include that, about 86 mothers (79.6%) were exhausted after delivery, 37 participants (34.3%) said extended recovery time from anesthesia (late wearing of anaesthetic effect), 15 mothers (13.8%) explained the uncomfortable breastfeeding position after cesarean section and 10 mothers (9.3%) stated that delayed in episiotomy suture. Added to that, 85 of mothers (78.7%) quoted that their baby was in NICU observation after delivery and 61 mothers (56.5%) said there was an increased time for the transfer of baby form NICU after observation to ward or transfer of mother from operational theater to ward delayed the breastfeeding initiation (Fig. 1).
3. Factors associated with delayed initiation of breastfeeding
In multivariate analysis, 3 variables emerged as significant predictors for the delay in EIBF. Mothers who had babies with a birth weight of less than 2,500 g had 4.33 times higher odds (95% confidence interval [CI], 1.12ŌĆō16.82; P=0.034) in delayed initiation of breastfeeding when compared to babies with birth weight more than or equal to 2,500 g. Mothers who had a cesarean section (95% CI, 1.57ŌĆō13.92; P=0.005) had 4.68 times higher odds of not initiating breastfeeding earlier than mothers who had a vaginal delivery. Similarly, the odds of delay in EIBF among mothers who had poor knowledge about breastfeeding was 4.61 times (95% CI, 1.44ŌĆō14.72; P=0.010) higher when compared to the mothers with breastfeeding knowledge. The Nagelkerke pseudo-R2 value for the final model was 36.7 percentages (Table 2). The EIBF rates and associated factors from other studies were summarized in Table 3.
Discussion
The present study showed that, out of 108 postnatal mothers, 47 (43.5%) initiated breastfeeding within 1 hour after delivery. The median breastfeeding initiation time was about 90 minutes (IQR, 30ŌĆō180 minutes). Approximately 73 infants (67.6%) were breastfed exclusively by their mothers, but the rooming-in rate was 47 (43.5%) only. Babies with birth weight less than 2,500 g; mothers who had cesarean section delivery and reduced awareness and knowledge about breastfeeding were found to be significant factors for delayed initiation of breastfeeding.
In the present study, EIBF rate was found to be 43.5%, despite the breastfeeding rate of 99.1%, which was similar to the EIBF rate at the national level (42.6%); however, it was found to be lower than the Puducherry state-level report (64.6%) [7,12]. Besides, the prevalence of EIBF observed in our study was lower than that observed in studies done in other states such as Maharashtra (45.2%), Andhra Pradesh (75.6%), and Tamil Nadu (97.5%) but higher than Madhya Pradesh (38.6%), Nagpur and Odisha (36.4%), and Bihar (24.86 percentage) [13-19]. This deviations of the rate within nation might be owing to study setting, sampling procedures in other studies, and possible effects from cultural factors. Similar cross-sectional studies done outside India, in Africa, Central America, Nepal, and Bangladesh showed higher prevalence of EIBF ranging from 47.3% to 80% while results from Uganda, Nigeria, and Northwest Romania showed lower EIBF rate (range, 19.7%ŌĆō34.7%) than our study findings [2,6,20-27]. (Table 3). The wide variation in EIBF rates may be due to disparities in social, cultural, and ethnographic factors, in breastfeeding practice.
Mothers who had delivered their baby by cesarean section were found to be associated with delay in initiation of breastfeeding (aOR, 4.68; 95% CI, 1.57ŌĆō14.72; P=0.005) as compared to those who had a vaginal delivery. This association has also been observed with the studies from India and other countries globally [2,6,13,15,18,20-23,26-28]. Maternal factors, such as maternal lassitude, inconvenient breastfeeding position due to post-cesarean pain, and insufficient breastmilk (due to reduced oxytocin release followed by anesthesia) [29] might have hampered the immediate direct skin-to-skin contact, was observed in this study also contributed for the delay [2,6,8,13,18,20-23,27,30]. This can be overcome by providing physical and psychological support to these mothers by their family members and healthcare providers immediately after ceserean section might improve the EIBF.
Institutional factors for EIBF among ceserean section mothers such as extended recovery time from spinal anesthesia and reduced rooming-in rate which were also found in our study might have contributed to this delay [2,6,8,13,18,20-23,27,30]. This reduced practice of EIBF in postoperative room immediately after C-section by healthcare professionals who assist in motherŌĆÖs recovery rather than initiating breastfeeding might lend to this factor [23]. This can be overcome by initiating maternal-infant skin-to-skin contact at the earliest through practices like breast-crawl that proven to have a major impact on EIBF even in cesarean deliveries [31,32]. Thus, healthcare providers and nursing staff need to be sensitized about these bottlenecks in initiating EIBF and need to be trained about the different breastfeeding positions, and practice of breast-crawl in cesarean sections. This also requires, appropriate guidelines and policy regarding the cesarean delivery at the healthcare center to improve the EIBF.
BabyŌĆÖs birth weight of less than 2,500 g was a significant factor for delayed breastfeeding initiation (aOR, 4.33; 95% CI, 1.12ŌĆō16.82; P=0.034) found in the study. Our findings were similar to the studies done in inside and outside India [2,13,15,20]. The possible explanation of the delay in EIBF could be due to poor suckling capacity, swallowing difficulty and poor co-ordination of a premature baby and requirement of admission in a NICU due to medical conditions like respiratory distress, jaundice, meconium aspirations, and again low birth weight [5,6,13,20] were also asserted in our study. These barriers can be addressed by providing early skin-to-skin contact and initiating breastfeeding immediately after delivery to improve their suckling reflex and giving expressed breast milk to the babies admitted in NICU to improve their nutrition and well-being. This explicates the want of practice and training to healthcare providers in handling low birth weight babies and counseling to the prospective mothers during the antenatal care (ANC) clinic to achieve the early initiation and continuation of breast milk feeding in low birth weight babies.
The current study showed that mothers who had poor knowledge about breastfeeding had 4.61 times higher odds to delay initiation of breastfeeding than mothers with knowledge about breastfeeding (95% CI, 1.44ŌĆō14.72; P=0.010). This was consistent with the findings of the studies done previously [13,26,28]. ANC visit or appointments acts as a bridgehead of the mothers to have contact with the healthcare professionals [33]. Multiple researches have revealed that approaches like health promotion and breastfeeding counseling during the ANC visit can enhance the rate of timely initiation of breastfeeding [5,9,22,24,27,34,35]. Thus, scaling up of intervention programs among antenatal mothers at the institutional level helps the mothers to be more receptive and provide them good opportunity to acquire knowledge about it to prepare them for timely initiation of breastfeeding [5,34]. In addition to that, healthcare professionals need to be trained on skills requires for efficient initiation of breastfeeding for its promotion and support along with nutritional education. Furthermore, this explains the paramount importance of implementing the baby-friendly initiatives at the institution level.
The major strengths of the study are the use of pretested structured questionnaire and data collection by a single investigator throughout the study. Collection of data at the point of discharge helps to minimize the maternal recall bias. However, being a cross-sectional study, temporality of association could not be assessed. Also, this was a hospital-based single centric study, in which the results cannot be extrapolated to the general population.
EIBF was practiced by less than half of the postnatal mothers, determined by birth by cesarean section, the babyŌĆÖs birth weight and mothersŌĆÖ awareness about breastfeeding. We recommend that additional support, training, and education need to be provided to the healthcare practitioners to increase breastfeeding initiation to the mothers predominantly who had cesarean sections to enable early skin-to-skin contact. Overall, this study also implies that comprehensive breastfeeding education programs and counseling targeting antenatal mothers need to be scaled up at the institution level. Added to these, there is an imperative need to focus on full implementation of the BFHI and infant young child feeding policies at the institutional level to intensify the EIBF and childŌĆÖs well-being.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link PubMed
PubMed Download Citation
Download Citation


